See ŌĆ£Accuracy of Endoscopic Diagnosis for Mild Atrophic Gastritis Infected with Helicobacter pyloriŌĆØ by Takuma Okamura, Yugo Iwaya, Kei Kitahara et al., 362-367
Helicobacter pylori infection is responsible for chronic gastritis. The progression from chronic gastritis, atrophy, and intestinal metaplasia to dysplasia is an important mechanism of gastric carcinogenesis. A meta-analysis showed that H. pylori eradication reduced the risk of the development of gastric cancer [1]. However, a later study showed that the risk of gastric cancer was still increased in the presence of gastric mucosal atrophy, even after H. pylori infection was eradicated [2]. These findings may imply that gastric cancer is entirely preventable by H. pylori eradication in patients with atrophic gastritis. On the basis of previous evidence, we surmise that eradication therapy for H. pylori infection could be more efficient in preventing gastric cancer when mucosal atrophy is mild or absent. It is likely that the progression to gastric cancer can be blocked before gastric atrophy develops. In other words, endoscopists should be aware that the identification of mild atrophic gastritis associated with H. pylori infection is important in the primary prevention of gastric cancer. This is especially important in the training of beginner endoscopists.
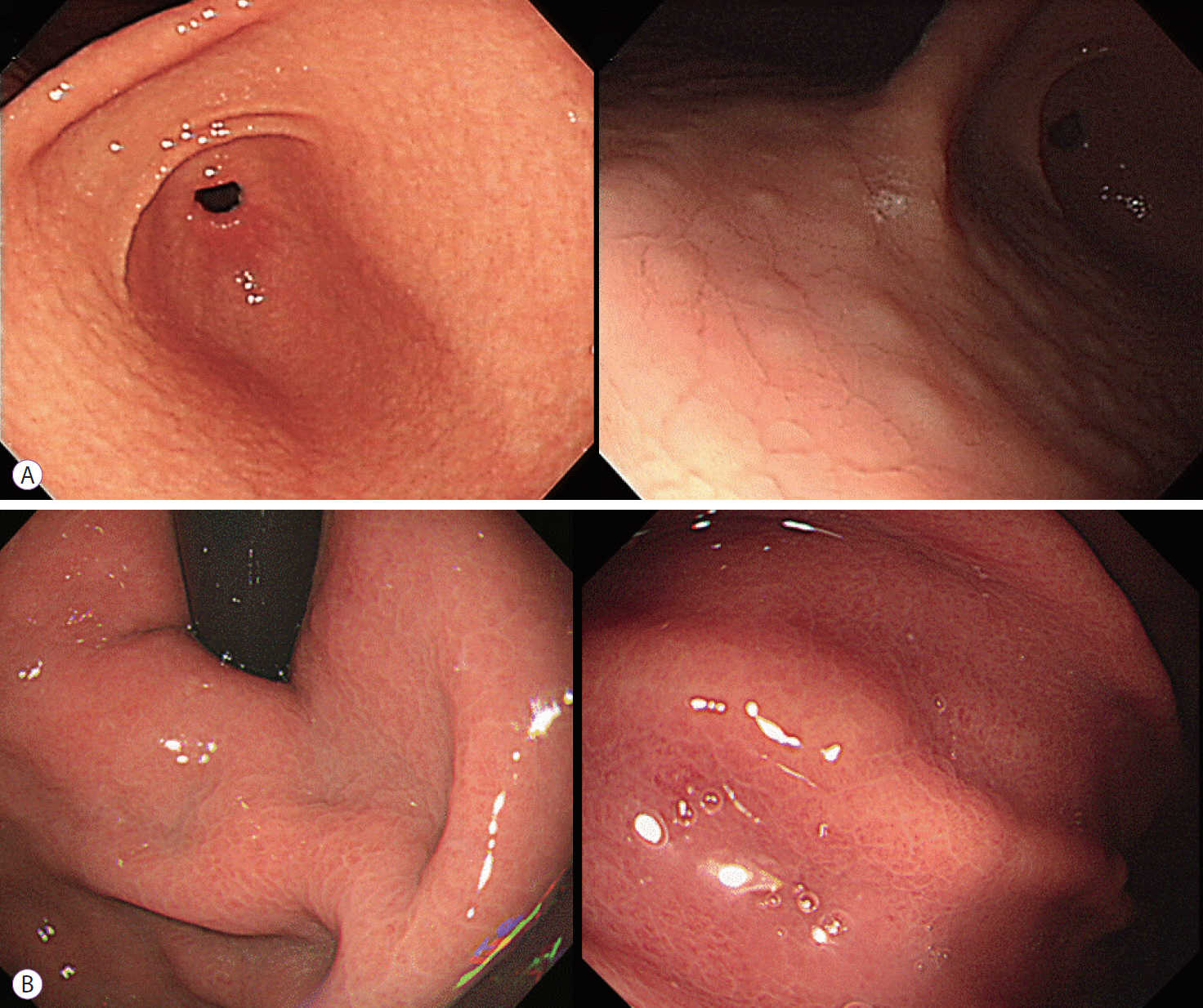
This study showed that the accuracy of endoscopic diagnosis of H. pylori infection in patients with/without mild atrophic gastritis (C-0, C-I) was approximately 67% [3]. In previous studies, the following distinctive endoscopic features were reported and were closely associated with H. pylori infection: atrophy, hyperplastic polyp, map-like/patchy/spotty redness, xanthoma, hematin, red streak, intestinal metaplasia, mucosal swelling, depressed erosion, enlarged fold, sticky mucus, fundic gland polyp, multiple white and flat elevated lesions, correctly identified regular arrangement of collecting venules, nodularity, and raised erosion [4-8]. Among these endoscopic features, nodularity had the highest diagnostic accuracy for H. pylori infection (89.3%), followed by mucosal swelling (76.6%) When endoscopists identified nodularity or mucosal swelling, the rate of diagnostic accuracy was high (Fig. 1). The characteristic histological finding of nodularity is hyperplasia of lymphoid follicles, whereas mucosal swelling is characterized by inflammatory cell infiltration and mucosal edema. In the progression of atrophy, nodularity begins to disappear from the antrum and becomes more localized with scattered type. Therefore, endoscopists should search carefully for characteristic nodularity, especially at the gastric angle and anterior/posterior walls of the antrum. Mucosal swelling is easier to recognize in the gastric body than in the antrum. Close attention to nodularity and mucosal swelling may improve the accuracy of endoscopic diagnosis of H. pylori infection in mild atrophic gastritis.
Although a number of studies have discussed endoscopic diagnosis of H. pylori infection, the findings have been ambiguous and contradictory. It was previously reported that the accuracy of endoscopic diagnosis of H. pylori infection was only 41.8% [9]. In a series of studies, several researchers insisted that endoscopic diagnosis of H. pylori infection was of no use in clinical practice, because of relatively low diagnostic yield (43%ŌĆō64%) [10,11]. On the other hand, a study in highly-endemic areas of H. pylori infection revealed that the accuracy of endoscopic diagnosis reached 79.5% [12]. Taken together, the inconsistency of diagnostic yields might stem from differences in regional prevalence of H. pylori infection. The results of this study were quite acceptable, although the diagnostic yield was relatively low compared with that of previous studies. The reason was that the study was performed only in cases of mild or non-atrophic gastritis. In previous reports, regular arrangement of collecting venules, hemorrhage, and fundic gland polyps showed high positive predictive value and specificity for an H. pylori-negative stomach [6,13-15]. Moreover, the diagnostic yield in H. pylori-negative cases was high, and inter-observer agreement was good. In the wake of this research, there are several problems to be solved. First, as for nodularity and mucosal swelling, inter- and intra-observer agreement is questionable. Second, it is necessary to confirm whether endoscopists can distinguish between H. pylori infection and H. pylori eradication.
Recently, artificial intelligence technology was evaluated in the diagnosis of H. pylori gastritis based on endoscopic images, and was able to diagnose H. pylori gastritis with higher accuracy [16]. It also shortened the diagnostic time, compared with manual diagnosis by an endoscopist. Endoscopic diagnosis using artificial intelligence has an infinite potential, and it will be supplemented and completed by the accumulation of these findings.
In conclusion, early detection of H. pylori gastritis and prompt eradication is a good therapeutic strategy for the prevention of gastric cancer. From this point of a view, this result is promising and will contribute to the early detection of H. pylori gastritis.