Introduction
Polyethylene glycol and picosulfate (Picolight powder; Pharmbio, Seoul, Korea) are equally effective bowel cleansers that are widely used in colonoscopy procedures [1]. However, picosulfate powder is easier to administer because of its orange flavor and smaller liquid volume requirement. When picosulfate powder is dissolved in water, magnesium oxide and citric acid combine to form magnesium citrate, which acts as an osmotic laxative, and sodium picosulfate as a stimulant laxative [2]. Picosulfate powder must, therefore, be completely dissolved in water and cooled before drinking because it produces an exothermic reaction, which occurs immediately after the substance comes into contact with water [3]. Six cases [3-8] of corrosive mucosal injuries on the oropharynx, esophagus, or stomach caused by undissolved sodium picosulfate powder have been reported, all of which improved without further complications [3-8]. The development of esophageal strictures from corrosive esophageal injury has never been previously reported. Nevertheless, this report presents a case of esophageal stricture following corrosive esophagitis from undissolved picosulfate powder.
Case report
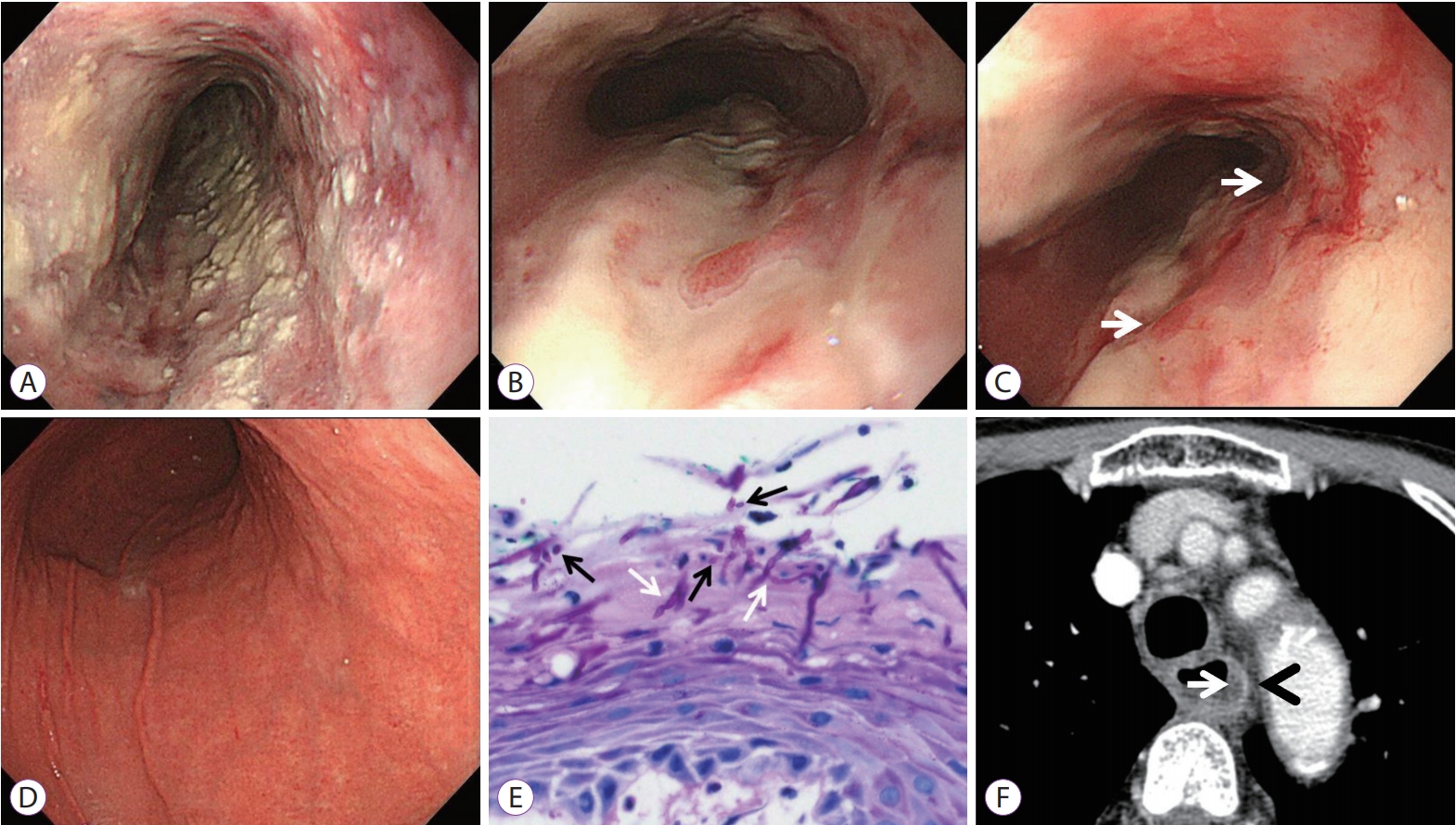
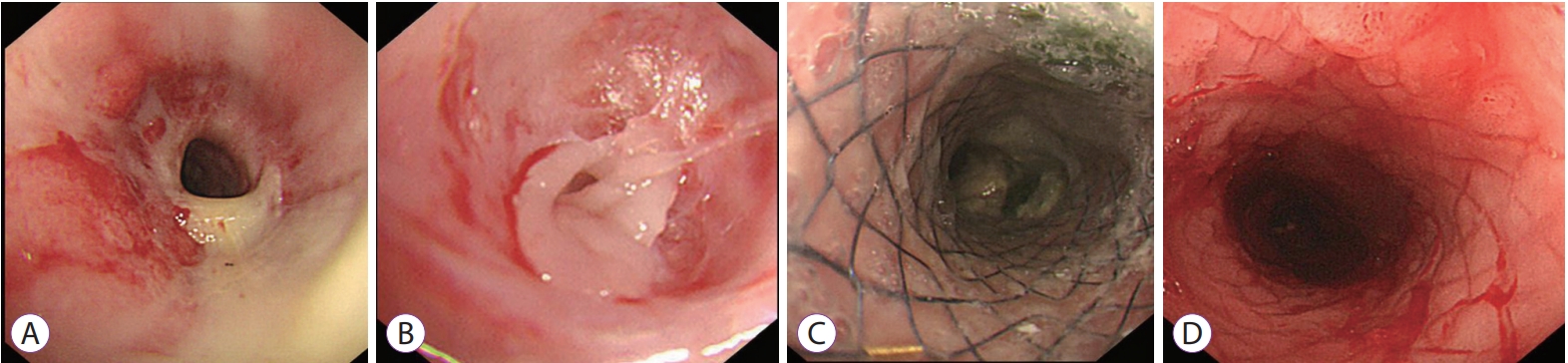
A 75-year-old woman came to our emergency department with severe sore throat and chest pain during food ingestion. One week previously, she had scheduled an esophagogastroduodenoscopy (EGD) and colonoscopy at her medical check-up. She was prescribed picosulfate powder as a colon cleansing agent with detailed education about the ingestion method. However, she took the powder and drank a small amount of water afterwards because she thought that would be easier than dissolving it. Immediately right after, a burning sensation developed in her chest. Ten hours later, she went to her follow-up appointment and was performed EGD, which showed a submucosal hemorrhage, ulcerative lesions, and spotty necrosis along the entire esophagus and corresponding mild erythematous lesions in the stomach (Fig. 1). She did not disclose her mistake and refused the physicianŌĆÖs advice for admission. For the next 7 days, she stayed at home, followed a liquid diet, and took pain killers. However, her symptoms worsened; thus, she visited our hospital. Her laboratory tests were normal, however, an emergent EGD revealed presence of diffuse ulcers with yellowish exudate throughout the esophagus (Fig. 2A-D). An endoscopic biopsy showed esophageal ulcers and candidiasis (Fig. 2E), nonetheless, she tested negative for Helicobacter pylori infection. A neck computed tomography (CT) scan revealed esophageal edema and increased wall enhancement (Fig. 2F). We treated her with fasting and parenteral nutrition, fluconazole 100 mg once daily for 10 days, and a parenteral proton pump inhibitor, pantoprazole 40 mg twice daily. After one week of admission, she complained of dysphagia with solid foods. A follow-up EGD revealed multiple ulcers and scars at the mid esophagus and a 25 cm luminal stricture from the upper incisor (UI) (Fig. 3A) although her candidiasis had resolved. After two weeks of admission, the patientŌĆÖs chest pain was endurable, and she could tolerate a liquid diet. However, 11 weeks after the picosulfate powder ingestion, she developed liquid food dysphagia. An ultrathin EGD revealed severe esophageal strictures ranging from 25ŌĆō30 cm from the UI (Fig. 3B). Consequently, esophageal stenting was performed using a 10 cm fully covered metal stent (Hanarostent; M.I. Tech, Pyeongtaek, Korea) through the scope (Fig. 3C). The esophageal stenosis was relieved after the stent was indwelling for 3 months (Fig. 3D). However, restenosis occurred 4 weeks later (Fig. 4A). We treated this with esophageal balloon dilation using a 20 mm controlled radial expansion balloon catheter (Microvasive; Boston Scientific Co., Natick, MA, USA) (Fig. 4B, C). The esophageal strictures improved after one year (Fig. 4D), and she was monitored for more than 3 years afterwards without symptoms.
Discussion
Caustic ingestion can cause severe esophageal and gastric injury. Tissue injury caused by corrosive alkaline and acidic substances vary depending on the type, quantity, concentration, and contact time [9]. Acidic agent-driven corrosive esophagitis is rare; however, it can lead to a similar [10] or sometimes worse outcome [9] than that induced by alkaline agents.
Picolight is dispensed in a powder form (sodium picosulfate 0.01 g, magnesium oxide 3.5 g, citric acid 12 g per sachet). Magnesium oxide and citric acid form magnesium citrate when the powder is dissolved in water. It is metabolized by gut bacteria into the active compound 4,4ŌĆÖ-dihydroxydiphenyl-(2-pyridiyl)-methane [2], which is a stimulant laxative that increases bowel peristalsis and mucosal secretions and blocks water absorption in the intestine [2]. However, when picosulfate is dissolved in water, it induces an exothermic reaction that can cause chemical burning in the gastrointestinal tract mucosa [3-8]. To prevent Picolight-associated tissue injury, dissolution of this powder in more than 200 mL of water is strongly recommended [2]. On the other hand, dissolving it in a low volume of water results in a more acidic liquid, which can lead to corrosive esophageal injury.
Six cases of corrosive injuries in the oropharynx [6], esophagus [3,5,8], or stomach [3-5,7] caused by partially dissolved or undissolved picosulfate powder have been reported (Table 1). The most common symptoms were burning sensations or pain in the throat, epigastrium, or chest, with hematemesis [5,8] or hoarseness [6] also occurring in some cases. The injury sites were determined by where the picosulfate powder is attached to. In one case, airway obstruction developed from oropharyngeal injury, which required endotracheal intubation [6]. In another case, the patient drank a large quantity of water immediately afterward, leading to acute gastric ulceration; however, no esophageal injury was noted [7]. All cases were conservatively treated with fasting, parenteral nutrition, and proton pump inhibitors, with additional empirical antibiotics in some cases [3-8]. The three cases involving the esophagus [3,5,8] did not progress to esophageal strictures. Therefore, partially dissolved powder, ingestion of large volumes of water afterward, or early treatment may reduce the risk of esophageal stricture development [3-8]. Conversely, in the present case, severe esophageal injury progressed to an esophageal stricture. Despite severe mucosal injury to the entire esophagus, treatment was delayed by 1 week. Additionally, the second EGD 1 week after ingestion revealed esophageal candidiasis in addition to extensive esophageal ulcers. Although chest pain improved two weeks after treatment, liquid food dysphagia occurred 11 weeks after ingestion as a result of the stricture formation. Therefore, drinking a small volume of water after ingestion and delaying treatment may induce severe mucosal injury and esophageal stricture. Hence, we perceive that the esophageal candidiasis did not influence the development of the esophageal stricture in this case, because it is a superficial infection and was easily treated using fluconazole.
An early endoscopy is a safe, reliable, and accurate diagnostic tool [11]. It is necessary since the mucosal injury grading is crucially significant for the management and prognosis of esophageal injuries [12]. Of the various endoscopic grading systems, Zargar classification is most commonly used [11]. Corrosive esophageal injuries of grade I (edema and erythema of the mucosa) and grade IIA (hemorrhage, erosions, blisters, and superficial ulcers) heal completely without sequelae. However, up to 70% of patients with grade IIB (circumferential lesion) and more than 90% of patients with grade III (focal or extensive deep gray or brownish-black ulcers) are likely to develop esophageal strictures or gastric scarring [11,12]. In this case, the patient was diagnosed with a grade IIIA esophageal injury since there were deep ulcers and focal necrosis that progressed to esophageal strictures. In addition to an endoscopy, a CT-based classification of esophageal corrosive injuries was a reliable tool for predicting long-term complications [13]. After 7 days, present case was characterized as grade II since there was wall and soft tissue edema but with increased wall enhancement.
There is no consensus about the ideal timing and method of endoscopic management of corrosive esophageal injury [14]. Endoscopic dilation with bougination or ballooning is generally recommended as first line treatment, and esophageal stents are used for caustic strictures resistant to dilation [14]. However, a recent study reported that esophageal dilation for caustic esophageal injury failed in three-fourths of the patients studied, and that long stricture length is a risk factor for failure [15]. Therefore, we treated this case conservatively during the acute phase of esophageal injury without stricture prevention procedures. Intralesional steroid injections or topical mitomycin have been reported as adjunctive endoscopic treatment options for complex strictures [16]. However, we treated the esophageal stricture using esophageal stenting instead of bougination or balloon dilation because there was a high risk of perforation in this case. Recent data revealed that esophageal stents should be removed within 12 weeks and clinical success with caustic strictures was 35%ŌĆō45% with a migration rate of 25%ŌĆō35% [17]. In this case, re-stenosis developed following the stent removal that eventually improved with esophageal balloon dilation.
We reported a case of esophageal stricture caused by undissolved picosulfate powder that the patient accidentally took. As this case demonstrates, detailed information emphasizing that undissolved picosulfate powder induces corrosive esophageal injury should be provided to patients.