CME for
KSGE members
Yang and Park: A Stone in Remnant Cystic Duct Causing Mirizzi Syndrome Following Laparoscopic Cholecystectomy
Quiz
A 63-year-old woman was admitted to the hospital with obstructive jaundice. Thirteen years prior, she underwent laparoscopic cholecystectomy for gallstones.
Computed tomography (CT) showed dilatation of the proximal common hepatic duct and intrahepatic duct ( Fig. 1A). A round signal void was then observed on magnetic resonance cholangiopancreatography ( Fig. 1B). On endoscopic retrograde cholangiopancreatography (ERCP), the bile duct was cut off at the level of the common hepatic duct; this suggested the presence of 1.5-cm filling lesions that led to the obstruction of the common hepatic duct ( Fig. 1C). Mass-like extrinsic compression in the common hepatic duct and clogging of the cystic duct orifice were observed on endoscopic findings of single-operator peroral cholangioscopy (SOPC) ( Fig. 1D). To address the jaundice, a plastic stent was inserted in the intrahepatic bile duct. What is the most likely diagnosis?
Answer 
Bile duct stone in the remnant cystic duct resulting in Mirizzi syndrome, following laparoscopic cholecystectomy.
Based on radiologic imaging and SOPC, it was suspected that either a stone in the remnant cystic duct resulted in common hepatic duct obstruction as Mirizzi syndrome or an inflammatory mass in the remnant cystic duct was present.
On follow-up ERCP, transpapillary biopsy and balloon dilation for the biliary stricture were performed ( Fig. 2A). Afterwards, numerous cholesterol stones were retrieved via basket extraction ( Fig. 2B). Transpapillary biopsy revealed a negative result for malignancy. A follow-up CT scan showed no residual stones or mass lesions in the bile duct ( Fig. 2C). Mirizzi syndrome is defined as the obstruction of the common hepatic duct, caused by extrinsic compression from an impacted stone in the cystic duct or infundibulum of the gallbladder [ 1, 2]. Patients with Mirizzi syndrome may present with jaundice, fever, and right upper quadrant pain [ 1, 2]. This condition is difficult to diagnose and treat. Its signs and symptoms may mimic that of gallbladder cancer. Notably, this patient had already undergone cholecystectomy 13 years prior. Therefore, the diagnosis of Mirizzi syndrome due to the extrinsic compression of gallstones in the remnant cystic duct was made even more difficult. SOPC and balloon dilation, resulting in the fragmentation of stones, may aid in the diagnosis of Mirizzi syndrome [ 3, 4]. The condition is often not recognized preoperatively in patients undergoing cholecystectomy and, thus, may lead to perioperative bile duct injury [ 1- 4]. Meanwhile, the jaundice may be managed preoperatively with transpapillary endoscopic stent placement across the biliary stricture [ 2]. Therefore, there should be a high index of suspicion for Mirizzi syndrome in jaundiced patients with common hepatic duct obstruction with a cystic duct stone and no obvious mass on radiologic imaging.
Fig.Т 1.
(A) Computed tomography scan showed the dilatation of the proximal common hepatic duct and intrahepatic duct. (B) A round signal void was seen on magnetic resonance cholangiopancreatography. (C) The bile duct was cut off at the level of common hepatic duct, suggesting 1.5-cm filling lesions that obstructed the common hepatic duct, as seen on endoscopic retrograde cholangiography. (D) Mass-like extrinsic compression in the common hepatic duct and clogging of the cystic duct orifice was found upon single operator peroral cholangioscopy. 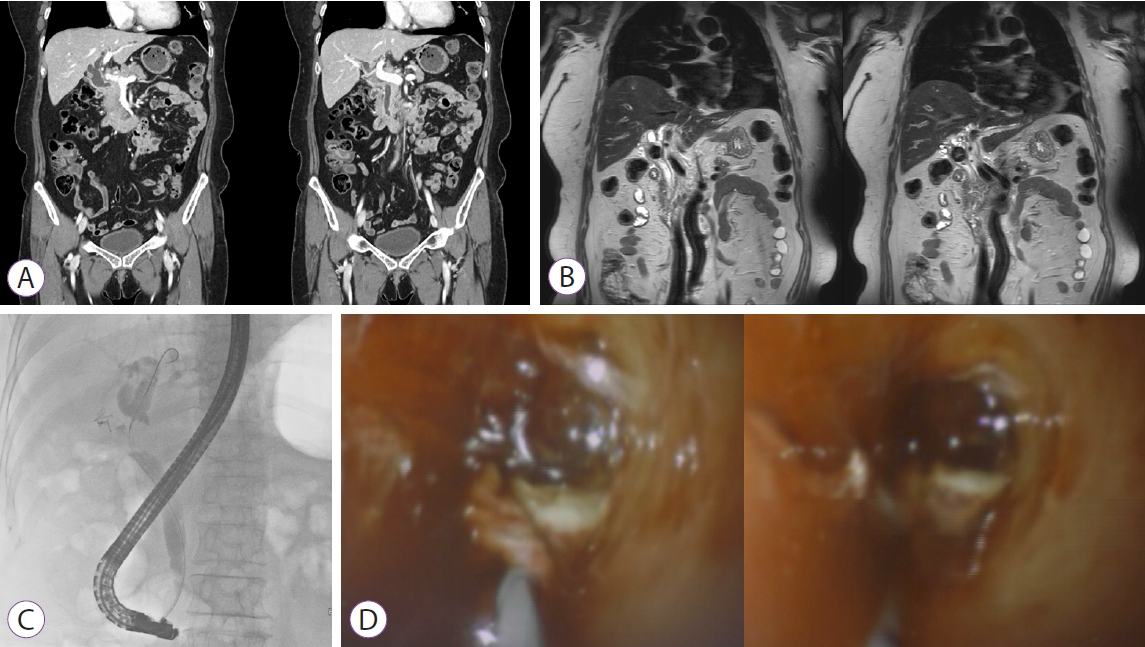
Fig.Т 2.
(A) On follow-up endoscopic retrograde cholangiopancreatography, transpapillary biopsy and balloon dilation for biliary stricture was performed. (B) Numerous cholesterol stones were retrieved via basket extraction. (C) Follow-up computed tomography scan showed no residual stones or mass lesions in the bile duct. 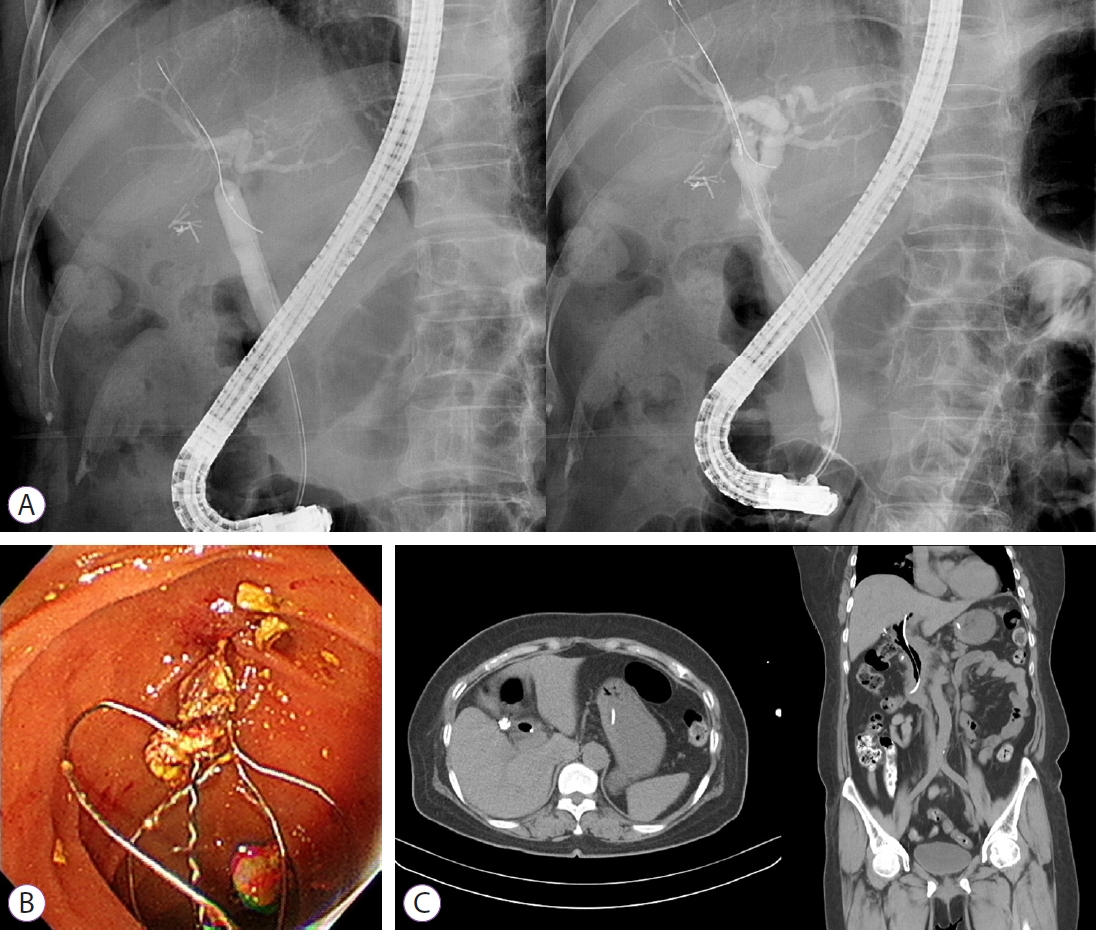
|
|







