Endoscopic submucosal dissection (ESD) is a minimally invasive treatment and enables en bloc resection of large lesions. However, ESD is a technically demanding and time-consuming procedure.1 Here, we report a "two-sword fencing" technique with an injection needle and an ESD knife.
A 74-year-old man presented with a laterally spreading tumor (LST), 7 cm in diameter, on the right wall of the rectum, and occupying half of the colonic lumen on colonoscopy. The tumor extended distally to the dentate line. Histological examination of biopsy specimens indicated tubular adenoma.
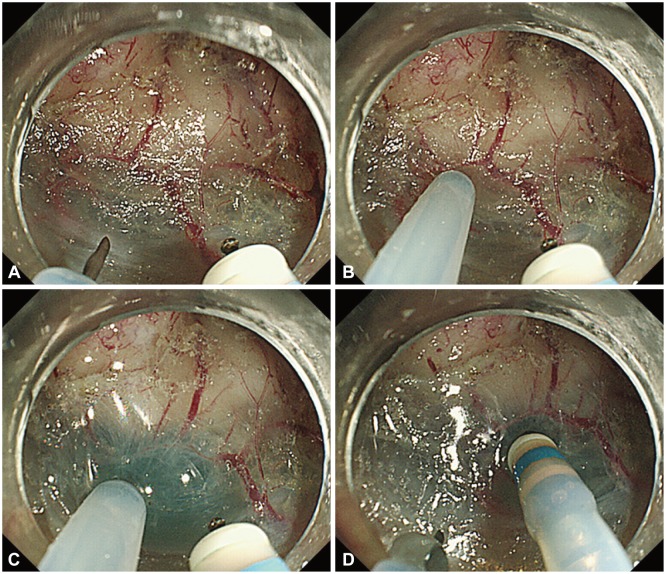
ESD of the rectal LST was carried out using a double-channel endoscope with a multibending system (GIF-2TQ260M; Olympus, Tokyo, Japan). Glycerol (Glyceol; Chugai Pharmaceutical Co., Tokyo, Japan) mixed with a small volume of epinephrine and indigo carmine dye was injected into the submucosal layer with the injection needle (IFH-SG; Top Corp., Tokyo, Japan). ESD was performed with a dual knife (KD-650Q; Olympus). "Dual" refers to the two extension lengths of the cutting knife; it has no capacity for injection. The electrosurgical unit (VAIO300D; ERBE, Tubingen, Germany) was set as follows: drycut (effect 2, 30 W) for circumferential incision; and swift-coag (effect 4, 30 W) for dissection. For the "two-sword fencing" technique, an injection needle and an ESD knife were inserted through either channel of a double channel endoscope (Fig. 1). Using ESD, en bloc resection of the tumor was performed in 140 minutes. Histological examination of the resected tissue revealed well-differentiated mucosal adenocarcinoma. Both the vertical and horizontal margins were negative.
Although flush knives (Fujifilm Medical, Tokyo, Japan) have a water-jet system that allows rapid needle-free infusion of solution into the submucosa, other knives such as the dual knife, flex knife, or hook knife lack this function.2 Takeuchi et al.3 compared the efficacy of flush knives with water-jet functionality to that of flex knives (electrosurgical endo-knife without a water-jet function). A total of 49 patients with superficial colorectal neoplasms were randomly assigned to undergo ESD using a flush knife or a flex knife. The median number of endoscopic device changes was 22 (range, 8 to 44) in the flex knife group and 9 (range, 1 to 35) in the flush knife group (p<0.0001). The mean operation time was 87.3 minutes (95% confidence interval [CI], 71.3 to 103.4) in the flex knife group and 61.0 minutes (95% CI, 49.3 to 72.7) in the flush knife group (p=0.02). The endoscopists using flush knives did not need to switch their devices as often. This helped reduce the total operation time, and enabled the endoscopists to perform their procedures without interruption. The "two-sword fencing" technique also saves time in changing endoscopic devices. The "two-sword fencing" technique allows dissection of the submucosal layer just after injection, before the collapse of the submucosal cushion. When the injected solution leaks from the submucosa, the "two-sword fencing" technique may be useful for speedy submucosal dissection.