INTRODUCTION
Colon interposition is a surgical procedure for reconstructing the esophageal conduit after esophagectomy, especially in situations in which the stomach cannot be pulled upwards to the oral side. First introduced by Kelling and Vulliet in 1911, colon interposition has been applied to benign conditions, such as esophageal stricture and esophageal cancer [1]. Briel et al. conducted a study on 393 patients who underwent esophagectomy and reported that the rates of short-term complications, such as conduit ischemia, anastomosis leak, and stricture, after colon interposition were 7.4%, 6.1%, and 8.7%, respectively [2]. Importantly, adenoma and adenocarcinoma may develop in interposed colons during a long-term follow-up period; however, only few reports addressed long-term outcomes such as adenoma and adenocarcinoma in interposed colon grafts. Here, we report a case of intramucosal adenocarcinoma in an interposed colon, which was treated by repeated endoscopic resection. Based on our experience as well as literature reviews, we suggest a strategy for appropriate screening and surveillance endoscopies for neoplasia in interposed colons.
CASE REPORT
A 68 year old female visited the gastroenterology department at our center due to abnormal findings on an esophagogastroduodenoscopy carried out at an outside hospital. The patient had undergone an esophagectomy with right colon interposition for lye-induced corrosive esophagitis 40 years ago. Five years following the esophagectomy, the patient underwent adhesiolysis and small bowel segmental resection with anastomosis due to mechanical ileus resulting from intra-abdominal adhesions. Since then, no follow-up endoscopy or fecal occult blood test had been performed.
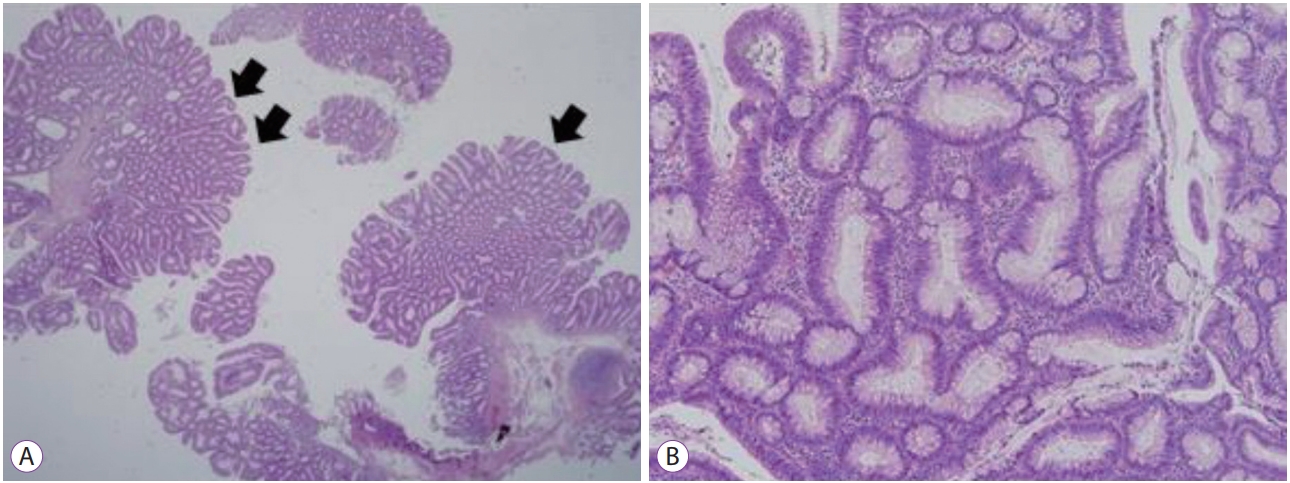
Recently, the patient experienced mild dysphagia and visited an outside hospital; a 20-mm sized non-pedunculated polyp at a distal portion of the interposed colon was detected on esophagogastroduodenoscopy, and endoscopic mucosal resection was attempted. However, en bloc resection could not be achieved due to technical difficulty; therefore, piecemeal resection was performed instead (Fig. 1). Consequently, complete resection was not achieved, and part of the lesion remained. Histological examination of the resected specimen showed a 4-mm sized moderately differentiated adenocarcinoma in the background of a villotubular adenoma. The adenocarcinoma component was confined to the lamina propria (i.e., intramucosal cancer) (Fig. 2). The resection margin was positive due to incomplete piecemeal resection. Per-anal colonoscopy was also performed to the native colon. Three polyps of 5 mm or less in size were removed by endoscopic polypectomy. Histopathology findings showed tubular adenoma. The patient was referred to the gastroenterology department of our center for management of the incompletely resected tumor at the interposed colon.
She had no past medical history, family history, or social history. Initial vital signs were within normal range: blood pressure of 135/86 mm Hg, respiration rate of 18/min, pulse rate of 68/min, and blood temperature of 36.7┬░C. Her body weight and height were 54.6 kg and 152 cm, respectively. Laboratory findings were within the normal range.
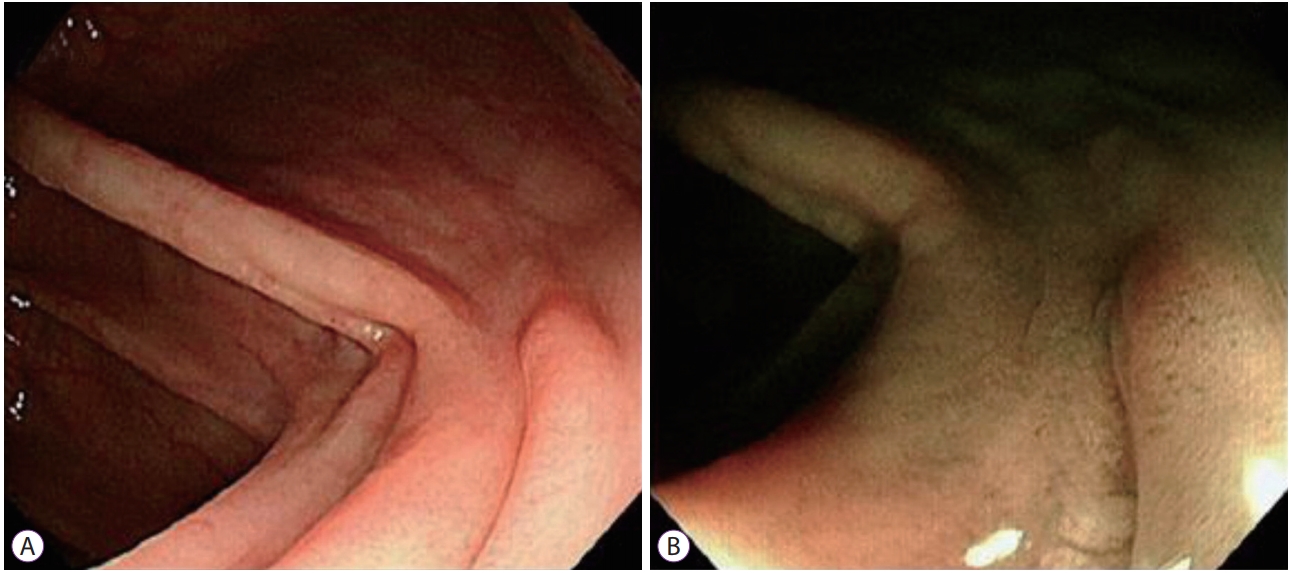
Esophagogastroduodenoscopy was carried out with a gastroscope (GIF HQ 290; Olympus Co., Tokyo, Japan). The proximal anastomosis site between the esophagus and the interposed colon was found 18 cm from the upper incisor, and the distal anastomosis site between the interposed colon and high body of the stomach was found 50 cm from the upper incisor. The stomach showed normal mucosal findings. A 12 mm sized residual sessile tumor was found at the interposed colon 38 cm from the upper incisor. Endoscopic resection was attempted, and piecemeal resection was performed with 2 pieces of the specimen. Gross complete resection was achieved with no visible residual lesion. Argon plasma coagulation (APC) was conducted at the post-resection ulcer base and ulcer edge to eliminate possible residual lesions, thereby, minimizing the risk of local recurrence (Fig. 3). There was no complication during the procedure. Histopathologic examination confirmed tubular adenoma (Fig. 4).
The patient underwent a follow-up esophagogastroduodenoscopy 1 year after the resection, which showed no evidence of recurrence (Fig. 5).
DISCUSSION
Colon interposition was first introduced in 1911 as a substitute for gastric pull-up surgery for cases in which esophagectomy was required but the stomach could not be used due to prior stomach surgery or combined tumor infiltration in the stomach. Lee et al. analyzed 1,011 Korean cases from June 2000 to June 2013 [3]; in their study, 67 patients underwent colon interposition and 944 patients underwent gastric pull-up surgery, and there was no statistically significant difference between the 2 groups regarding postoperative complications such as anastomosis site leakage, stricture, and fistula. The authors thus concluded that colon interposition is a reasonable alternative for gastric pull-up. Similarly, DeMeester reported that morbidity and mortality rates between colon interposition and gastric pull-up were not significantly different in benign esophageal illnesses such as esophageal stricture [4]. The short-term outcomes after colon interpositions are relatively well-known; however, only few reports have described the long-term follow-up outcomes in patients with colon interposition. This is because colon interposition is usually performed in patients with esophageal cancer, whose long-term survival rates are low. In contrast, our patient underwent colon interposition due to benign esophageal stricture caused by corrosive esophagitis; therefore, she was able to survive for 40 years after colon interposition before intramucosal cancer developed in the interposed colon.
Intramucosal carcinoma in the colon is limited to the mucosa and is known to have no risk of lymph node metastasis [5]. Therefore, complete endoscopic resection of intramucosal carcinoma in the colon can achieve a cure without risk of recurrence and/or metastasis. In our current case, complete resection failed at the initial attempt, and repeat endoscopic resection was performed to achieve complete resection of the residual lesion. Although there is no definite consensus on the management of grossly residual intramucosal cancer and/or positive histological resection margin after a grossly complete resection of intramucosal cancer, repeat local eradicative resection may be a plausible option, considering the non-metastatic features of intramucosal colorectal cancer. This suggestion was supported by our previous report on the clinical outcomes of 38 patients with intramucosal colon cancers, which were grossly removed by endoscopic resection but showed positive or uncertain histopathological resection margins. These patients showed neither local recurrence nor distant metastasis for an average of 18.3 months of follow-up without additional intervention [6]. For a more definite eradication of possible residual lesions, we additionally performed APC after the repeated endoscopic resection. Previous reports showed that APC decreased the risk of local recurrence after piecemeal resection and/or difficult endoscopic resection for recurrent polyps at the fibrotic scar sites [7,8]. Moreover, the specimen of repeated endoscopic resection revealed only benign tubular adenoma with no evidence of malignancy, although the initial endoscopic resection specimen from the other hospital was confirmed as intramucosal carcinoma. This indicates that all carcinoma components were resected in the first endoscopic resection, and only the benign adenoma component remained.
Currently, screening colonoscopy is recommended at 5ŌĆō10 year intervals after 50 years of age in the average-risk asymptomatic population [9-11]. Because of the rarity of interposed colons, there is no consensus on a screening endoscopy interval for people with interposed colons. Furthermore, compared to native colons, interposed colons may have differences in intraluminal chemical composition and diversity of intraluminal microbiota because of their different anatomical positions [4]. Despite such uncertainty, it may be reasonable that the general guidelines for colorectal cancer screening for native colons be applied to interposed colons as well, considering the slowly progressing adenoma-carcinoma sequence during prolonged periods. Another issue regarding endoscopy screening of interposed colons is the necessity of gastric cancer screening. The Korean national cancer screening program for gastric cancer recommends that screening esophagogastroduodenoscopies be carried out every 2 years starting from 40 years of age. Therefore, if we consider the screening program for both the stomach and the colon, an adequate screening strategy for early detection of adenoma and adenocarcinoma in interposed colons should be conducting esophagogastroduodenoscopy every 2 years, because it can observe interposed colons as well as the stomach.
Reports on adenoma and adenocarcinoma in interposed colons are rare: since the first report in 1968 by Goldsmith et al., 21 cases have been reported [12]. Nine of the 21 patients underwent esophagectomy with colon interposition due to malignancy, and the remaining had benign esophageal illnesses. In Korea, the first case was reported in 2007 by Hwang et al., which was of an intramucosal cancer in the interposed colon managed by endoscopic resection [13]. Two more Korean cases were reported afterwards in 2010 and 2012, which were advanced cancers in the interposed colons [14,15]. Similar to our current case, all reported cases in Korea underwent esophagectomy with colon interposition because of corrosive esophagitis. Supplementary Table 1 summarizes the literature review of adenoma and adenocarcinoma in interposed colons.
In conclusion, we here report a patient who underwent colon interposition surgery due to corrosive esophagitis and was later diagnosed with intramucosal cancer in the interposed colon. The tumor was completely removed by repeated endoscopic resection. Based on our experience and literature review, we suggest that screening endoscopy should be performed for the detection of early neoplasia in the interposed colon; considering the increased possibility of adenoma and adenocarcinoma development, this is especially recommended in patients who survive for a long period after esophagectomy. When considering the necessity of screening esophagogastroduodenoscopy for gastric cancer in the population aged 40 years, interposed colon screening may be performed via esophagogastroduodenoscopy.