HemosprayTM powder is a highly absorptive mineral powder, used for initial hemostasis in the setting of non-variceal upper gastrointestinal bleeding. Furthermore, its effectiveness has been studied in lower gastrointestinal bleeding. However, to the best of our knowledge, there has been no report of its use in the setting of bleeding from a non-gastrointestinal lesion. Herein, we present a case of successful HemosprayTM usage for temporary control of massive bleeding from a non-gastrointestinal tumor. Written informed consent was obtained from the patient for publication as per hospital policy.
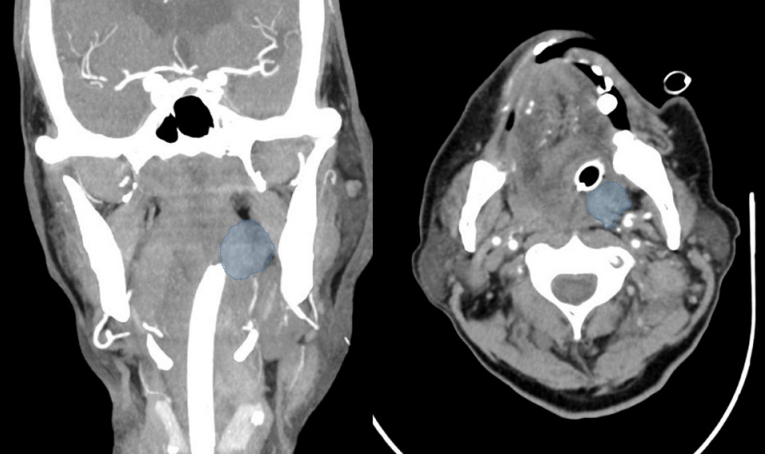
A 69-year-old male with a past medical history of Childтs A liver cirrhosis, secondary to alcoholic liver disease, was admitted with the complaint of per oral bleeding. He was recently diagnosed with metastatic hypopharyngeal carcinoma. A month ago, he presented with a painless neck lump and a computed tomography scan of the neck had revealed a 1.6 cm У 4.5 cm hypopharyngeal mass in contact with the aryepiglottic folds, with necrotic adenopathy of bilateral cervical lymph nodes. Nasal endoscopy revealed irregular lesions at the posterior pharyngeal wall and left pyriform fossa, with no airway obstruction.
On the present hospital admission, he presented with a large amount of per oral bleeding, and in order to protect the airway from the aspiration of massive hemorrhage, emergency otorhinolaryngologic examination was arranged after oral endotracheal intubation, and the craggy posterior pharyngeal wall tumor was noted to be actively bleeding. The patient was sent for a computed tomography angiogram demonstrating the mass (Fig. 1), but there was no contrast extravasation at the time of the study.
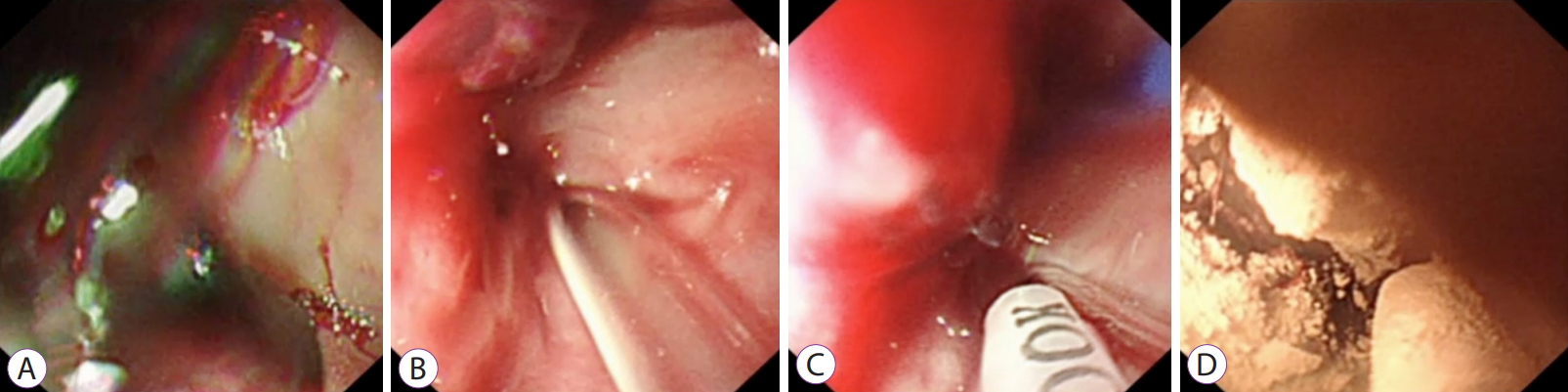
As the patient had a known case of liver cirrhosis, there was a concern of the possibility of variceal bleeding as the cause of per oral bleeding. An esophagogastroduodenoscopy was done, which showed no varices or upper gastrointestinal tract bleeding. On endoscopy, a large clot overlying the hypopharynx was seen (Fig. 2A), and it was flushed away to reveal the bleeding tumor (Fig. 2B). As the airway had already been secured and the bleeding was brisk, after discussion with the on-site otorhinolaryngologist, the decision was made to apply a hemostatic powder (TC-325 HemosprayTM; Cook Medical, Bloomington, IN, USA) to the hypopharyngeal tumor (Fig. 2C, D), which was done successfully. The bleeding stopped and the patient underwent palliative radiotherapy after six days. Further details are elaborated in a Supplementary video 1. The patient remained intubated for 9 days in the intensive care unit, and after the completion of 2 sessions of palliative radiotherapy, he was successfully extubated. He completed the course of palliative radiotherapy inpatient and remained asymptomatic for 6 months post-bleeding.
TC-325 HemosprayTM; Cook Medical is a hemostatic powder, with a two-fold mechanism for hemostasis: firstly, through the formation of a mechanical barrier at the bleeding site and secondly, by the promotion of thrombus formation via a concentration of platelets and clotting factors [1]. It is approved for use in non-variceal upper gastrointestinal bleeding, as either the primary or salvage therapy, for example, in cases of malignancy related bleeding [2]. We present a case of successful HemosprayTM usage for temporary control of massive bleeding from a non-gastrointestinal tumor. Hypopharyngeal tumors are usually within the purview of otorhinolaryngology, as this case illustrates, but the need for hemostasis transcends all borders and fields.
The use of HemosprayTM has potential risks [3], and there are several clinical pre-requisites for the use of HemosprayTM in the pharynx. Firstly, upper airway intubation is essential due to aspiration risk from severe tumor bleeding, as well as a similar risk from the inhalation of the mineral powder during application. Due to the proximity of the tumor location to the mouth, there is also a potential risk of powder exposure to the endoscopist and assistant, and personal protective equipment (surgical mask and eye-shield) are, therefore, recommended. Secondly, to optimize the efficacy of the powder in hemostasis, it is suggested to leave the sprayed region undisturbed for a day unless there is overt evidence of further bleeding.
Thirdly, the hypopharynx is a confined space, and as HemosprayTM has a spray application, it requires a typical distance of 1т2 cm from the lesion for efficient application [4]. Care must be taken during manipulation of the spray catheter in such a confined space. Finally, HemosprayTM buys time to arrange for definitive control measures for tumor bleeding, which in this case was radiotherapy. In a case series of patients with upper gastrointestinal tumors, using HemosprayTM as the primary modality of hemostasis reported no further bleeding in 80% at 30 days and 50% cases at 6 months.