Interventional Endoscopic Ultrasonography: Present and Future
Article information
Abstract
The technical advances in endoscopic ultrasonograpy (EUS) and accessories have enabled performing EUS-guided intervention in the pancreas and biliary tract. Many research centers have been performing or investigating EUS-guided drainage, EUS-guided celiac plexus neurolysis and block, EUS-guided anastomosis that includes choledocho-enterostomy and choledocho-gastrostomy, EUS-guided ablation and injection therapy mainly for pancreatic neoplasm, EUS-guided photodynamic therapy and EUS-guided brachytherapy. Some of these are currently clinical applications and others are under investigations in clinical studies or animal models. Further detailed randomized controlled clinical trials and the development of materials will bring us into a new era of therapeutic EUS.
INTRODUCTION
Endoscopic ultrasonography (EUS) was developed to observe abdominal organs with a sonic probe located in the nearby gastrointestinal tract. With improvements of sonographic resolution, application of Doppler imaging and the technical progress of endosonograhic accessories, EUS-guided tissue samplings have been conducted more frequently in various clinical situations.
Linear-array therapeutic probes with large working channels have recently been developed. These technical advances enable us to perform EUS-guided intervention in the pancreas and for biliary tract disease in various clinical situations and to investigate new procedures mainly regarding the local control of pancreatic tumors. Moreover, new innovative techniques are under investigation in animal models. In this review, we focus on interventional EUS mainly for diseases of the pancreas and biliary tract.
EUS-GUIDED PSEUDOCYST DRAINAGE
Symptomatic and complicated pancreatic pseudocyst can be drained radiologically, surgically or endoscopically by way of gastrocystostomy or duodenocystostomy. In the appropriate setting, EUS-guided drainage of a pancreatic fluid collection can be considered as the treatment of choice to treat pancreatic pseudocysts. A large-channel echoendoscope allows this to be accomplished as a single stage procedure, and so this avoids the need for other therapeutic procedures. It was reported to have a higher success rate and lower morbidity in several comparative studies.1-5
Compared to conventional endoscopic drainage, EUS scanning determines the optimal puncture site by identifying the intervening blood vessels and the shortest needle path. This merit allows us to perform drainage even in cases without bulging in the gut lumen. After puncture of this site, the technique is almost the same as conventional endoscopic drainage (Fig. 1). Contrast medium may be injected into the cyst and then a guide wire is positioned. A needle knife, a bougie and a dilatation balloon are introduced through the working channel and they are used to carry out dilatation of the EUS-guided transgastric or transduodenal puncture of the cyst.

Endoscopic ultrasonograpy (EUS)-guided pseudocyst drainage. After EUS-guided puncture of pseudocyst (A) and dilatation of puncture site, pus was coming out from infected pseudocyst (B). Endoscopic nasobiliary drainage tube would be inserted over guide wire to irrigate the cyst after a pigtail plastic stent was inserted (C).
Below the guidewire, a nasocystic drain or stent is placed within the cyst to establish complete drainage of the pancreatic pseudocyst or abscess. A 7 Fr plastic stent is commonly inserted due to the size of the working channel of the echoendoscope. For efficient drainage, multiple stentings combined with nasocystic drainage are used. Full-covered self-expandable metal stent insertion is currently under study to obtain a larger drainage route.
EUS-GUIDED CELIAC PLEXUS NEUROLYSIS AND BLOCK
Celiac plexus neurolysis (CPN) is the injection of absolute alcohol for destroying the sympathetic plexus near the celiac axis to relieve abdominal pain, and this is mainly done in pancreatic cancer patients. Celiac plexus block (CPB) is the injection of steroids to inhibit the pain pathway mainly in patients with chronic pancreatitis. In both procedures, bupivacaine is usually added to relieve initial pain.
EUS-guided CPN can be done via the anterior approach, so it can avoid serious complications brought about by the posterior approach such as parasthesia, paraplegia and pneumothorax.6 Another advantage of this technique is to visualize the intervening blood vessels and sometimes the ganglia itself. Real time visualization by EUS enables the injection into the celiac space and sometimes the ganglion itself.
CPN showed alleviation of pain in 70-90% of the patients with pancreatic cancer.7-9 On the other hand, CPB seemed to yield a marginal benefit (a 30-60% response rate) in chronic pancreatitis patients. A few studies showed EUS-guided CPN provided superior pain relief compared to CT and fluoroscopy guided celiac plexus ablation therapy.7-9 Further studies are needed for assessing the long-term efficacy of CPN and improving pain relief in patients with chronic pancreatitis.
EUS-GUIDED ANASTOMOSIS: BILIARY AND PANCREATIC DUCT
Endoscopic retrograde cholangiography (ERCP) is a palliative option for relief of malignant biliary obstruction. It is sometimes impossible due to anatomic and technical difficulties. Surgical or percutaneous biliary drainage are alternative methods, but they have higher morbidity and more discomfort than an endoscopic approach. EUS-guided drainage of the bile duct has recently been studied.10-19 Hepaticogastrostomy, choledochoduodenostomy and the rendezvous transpapillary approach are commonly performed according to the anatomic feasibility.
The bulb of the duodenum can be recommended as a puncture site for choledochoduodenostomy in the case of distal common bile duct obstruction because it has some merits (Fig. 2): a close location to the bile duct, it is away from obstructing tumor, there are no intervening major vessels and good stabilization of the echoendoscope. After a convex linear-array echoendoscope guided puncture, a needle knife, bougies and a balloon dilator are used to make and dilate a route. A plastic stent or metal stent is bridged between the dilated bile duct and the duodenal bulb. Hepaticogastrostomy is performed when the left intrahepatic duct is dilated due to perihilar biliary obstruction (Fig. 3). The usual puncture site is the high body of the stomach. The method after a puncture is almost same as choledochoduodenostomy. In the transpapillary approach, EUS-guided placement of a guide-wire through the papilla is performed. After withdrawing the EUS, an endoscopist inserts an ERCP endoscope, grasps the transpapillary wire with a snare or a biopsy forceps and withdraws it through the operating channel for retrograde introduction of a sphincterotome over the wire.
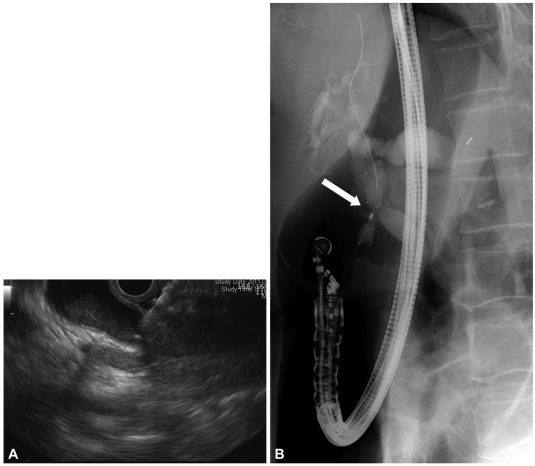
Choledochoduodenostomy. Due to duodenal partial obstruction, a transpapillary metal stent insertion was impossible. After endoscopic ultrasonograpy-guided puncture of dilated common bile duct (CBD) (A), fully covered metal stent was inserted from duodenal bulb to distal CBD (B).
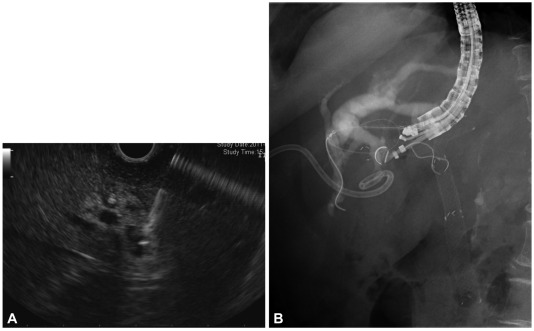
Hepaticogastrostomy. Jaundice hadn't resolved after percutaneous and endoscopic drainage. Endoscopic ultrasonograpy-guided puncture of a dilated left intrahepatic duct (A) and placement of metal stent (B) was performed.
Around 90% technical success rates were reported. Several complications such as bile peritonitis, cholangitis, cholecystitis, and pneumoperitoneum were observed and most cases were resolved without significant morbidity. Larger studies and more experience are necessary to define the true risk-benefit profile of this intervention relative to other methods such as percutaneous access.
EUS-guided drainage techniques are also applied to the pancreatic duct with almost same technical approach.16,17,19 These have been reported in much more limited numbers of patients. The success rate was a little lower and the complication rate was higher than EUS-guided biliary drainage. It remains technically challenging for the aspect of the difficult puncture of the pancreatic duct and stabilization of the endoscope.
To increase the success rate and decrease the complication rate, the development of EUS-specific accessories is needed, and particularly dedicated stent systems that reduce the potential for bile leak. The forward-viewing linear echoendoscope, which is currently only available as a prototype, may also help to improve the technical feasibility.20
EUS-GUIDED CYST ABLATION
Cyst ablation with ethanol and with or without chemotherapeutic agents showed promising results in some studies.21-25 They showed effective decrease or disappearance of cysts after ablation therapy on the radiological evaluation. After 3 months or 12 months, the complete radiological eradication rates were 33% to 79% with minimal complications. Multiple endoscopic sessions might increase the rate of image-defined cyst resolution.23 However, the long-term outcomes and the effect of preventing malignancy in mucinous cystic lesions have not yet been answered. Moreover, the patients who received ablation therapies and who showed complete eradiation seemed to have no need of any interventions.23 Only observation of cysts could be enough for them. It is prudent that the generalized clinical application of ethanol ablation is deferred until well-organized clinical trials show real benefits to alter the natural history of pancreatic cysts.26
EUS-GUIDED ABLATION THERAPY FOR SOLID PANCREATIC TUMOR
Some recent studies have shown the feasibility of radiofrequency (RF) ablation in pancreatic cancer in an open, percutaneous or laparoscopic setting.27,28 However, RF ablation in the pancreas could be dangerous without cooling the adjacent tissue and real-time visualization of the ablation.28-32 On comparing techniques, EUS-guided ablation has some theoretical advantages such as it is less invasive than the surgical approach and more selective than the percutaneous approach. However it is still under experimentation in animal models.33-35 In animal models, the desirable ablation effect can be achieved by adjusting the time and energy delivered into porcine pancreas, but the complications such as pancreatitis or adhesion of the surrounding viscera have not been adequately evaluated to apply this technique to clinical fields. A more exact delineation of a lesion in 3D configuration and delicate adjustment of the ablation area may be helpful to improve the safety.
Neuroendocrine tumor behaves more indolently than pancreatic cancer. Even in the case of metastasis, local debulking surgery and/or metastasectomy increases the survival of patients. Local ablation therapy with EUS-guided probe can theoretically be done. However, until now there were only a few anecdotal cases of EUS-guided ablation of neuroendocrine tumor. EUS-guided alcohol ablation of an insulinoma36 and the hepatic metastasis of insulinoma treated with percutaneous radio-frequency ablation37 were reported. EUS-guided ablation might be applied to high-risk patients.
EUS-GUIDED INJECTION THERAPY
Advanced pancreatic cancer has a dismal prognosis with the median survival being 3-4 months. Until now, no therapy has been proven to increase survival of these patients. Therefore, the main aim of therapy is to improve the quality of life.
Several investigational studies were conducted using EUS-guided injection of various therapeutic agents, including various onco-viruses,38 chemotherapeutics and immune cells. After animal studies with swine pancreas, some of them were applied to patients. Unfortunately, no agent has currently shown an efficient tumor killing effect (Table 1).

Endoscopic Ultrasonograpy-guided Injection Therapy
The EUS-guided approach to pancreatic cancer from the stomach and duodenum is a potentially minimal invasive option for locally advanced cases, but the injected agents have not been so effective in patients with advanced pancreatic cancer.
EUS-GUIDED PHOTODYNAMIC THERAPY
Following the infusion of photosensitizing drug, target tissue necrosis can be induced by exposure to light of a proper wavelength. EUS-guided fine-needle aspiration technique can be used for delivery of a light source to pancreatic cancer. The feasibility of this therapy was tested in a healthy swine model.39,40 There were no serious complications and there was proper tissue necrosis. Further studies that will consider the cost-effectiveness and biology of pancreatic cancer are needed for this therapy.
EUS-GUIDED FIDUCIAL PLACEMENT
A fiduciary marker or fiducial is an object used as a point of reference in external beam radiation therapy. Only gold fiducials are available to facilitate stereotactic body radiotherapy (SBRT) for the treatment of locally advanced pancreatic cancer. Placement of gold fiducials in the lesions is performed with EUS-guided delivery through a 19-guage needle,41-44 which enables a high-dose therapeutic beam of radiation to reach the tumor. The technique to push fiducials to go through the curved pathway is a technical challenge. The stylet-push method or the sterile water-push method is used.44 The successful placement and SBRT were done in around 90% of patients.43,44 The fiducials migrated in less than 5% without complication. To define their clinical usefulness, fiducial placement should be compared with conventional radiation therapy in prospective randomized blinded trials.
EUS-GUIDED BRACHYTHERAPY
Intraoperative interstitial brachytherapy has showed some beneficial effects for the local control of malignant pancreatic tumors. During operation, radioactive seeds placed in the pancreatic tumors emit steady gamma rays that lead to local ablation. EUS is used to place radioactive materials into the pancreas without laparotomy. Iodine-125 radioactive seeds were inserted through a 19-guage needle.45,46 In a pilot study, a partial response of unresectable pancreatic cancer was observed in 26.7% (4/15 patients) with limited improvement of pain. Only minor complications were reported in this study and in some porcine models.47 Complications such as fistula formation, gastrointestinal bleeding, ascending cholangitis and intrahepatic cyst formation were reported in operative settings.48 Considering the nature of pancreatic cancer and risk/benefits of brachytherapy, the precise role of this modality should be carefully investigated.
CONCLUSIONS
EUS-guided therapy is a new frontier for endoscopists. EUS-guided pseudocyst drainage and celiac plexus neurolysis and block can be recommended as a standard treatment if they are indicated. The others are under investigation and some of them showed promising results. Further progress of technology will make interventional EUS more useful for treating pancreatico-biliary diseases and well-designed clinical trials will clarify the role of investigational EUS-guided therapies.
Notes
The authors have no financial conflicts of interest.