INTRODUCTION
The best potentially curative therapy for malignant biliary obstruction is complete surgical resection.1,2 Unfortunately, a majority of these patients with advanced cases are not good candidates for such curative therapy and may benefit from palliative therapy biliary drainage with stent placement is the treatment of choice for malignant biliary obstruction caused by unresectable neoplasms. Median survival of such patients is lower without biliary than with the biliary drainage,3-5 and bacterial cholangitis or liver failure often contributes to death.
The aims of palliation in these patients are to relieve the obstructive cholestasis and its associated morbidities like pruritus, cholangitis and pain; to avoid liver failure due to progressive biliary obstruction; and to improve quality of life, cost-effectiveness, procedure-related complications and hospital stays through minimal invasive therapy.6 Palliation of obstructive cholestasis can be achieved successfully through two major non-surgical routes; one is a percutaneous route via percutaneous transhepatic cholangiography (PTC) and the other is an endoscopic route via endoscopic retrograde cholangio-pancreatography (ERCP).
Biliary drainage via the endoscopic route offers the advantages of physiologic bile drainage and has been proved to be more non-invasive and comfortable for patients than that via the percutaneous route.7,8 A major disadvantage of percutaneous drainage is the presence of a percutaneous tube, which could be uncomfortable for patients and cause tube related-complications, such as hemorrhage, infection, bile leakage, pleural complications, catheter blockage and migration. Therefore, in the palliation of malignant biliary obstruction, the endoscopic approach can be initially used with percutaneous radiological intervention reserved for any unexpected failures. The strategy of palliative treatment differs according to the location (i.e., hilar or distal bile duct) of the malignant biliary stricture.
PALLIATION FOR MALIGNANT DISTAL BILE DUCT OBSTRUCTION
The majority of distal bile duct obstructions are inoperable, and therefore restoring biliary flow with relief of jaundice and pruritus is the primary aim in the palliation of obstructive cholestasis due to distal lesions. Endoscopic biliary drainage with biliary stent placement has now become the main and least invasive palliative modality for achieving adequate symptom relief, which has been proven to be more effective in >80% of cases with lower morbidity than surgery, and perhaps may provide a survival benefit in patients with obstructive cholestasis due to unresectable malignant distal bile duct obstructions.9 When it fails or is unable to be performed, percutaneous biliary drainage with or without percutaneous stenting may be a better choice as an alternative palliation of malignant distal bile duct obstructions. Endoscopic route via ERCP in these patients has several advantages over percutaneous route via PTC. The duodenum and the papilla can be directly inspected to check for tumor infiltration under endoscopic view of ERCP, cytological or biopsy samples can be easily obtained via endoscopic channel and subsequent placement of a biliary stent can be performed to relieve the obstructive cholestasis. Therefore, most stents used on these patients are inserted endoscopically, although many non-comparative studies, assessing the outcomes, between percutaneous and endoscopic palliation for treatment of distal bile duct obstruction, stated that there were no significant differences in technical success, complication and mortality rates.10-12
The two main types of commercially available biliary stents are plastic stents and self-expandable metal stents (SEMS). Biliary stents are inserted successfully in approximately 90% to 95% of patients with malignant distal bile duct obstructions and the procedure is more often successful in patients with distal rather than hilar lesions.9 When contemplating endoscopic palliation of obstructive jaundice, important variables that need to be considered include location and extent of the biliary obstruction, potential need for repeated interventions, choice between plastic versus metal stents, and the life expectancy of the patient.13
Technique of endoscopic biliary stenting
Palliative drainage of malignant distal bile duct obstruction should be first attempted endoscopically. After cannulating the bile duct and injecting contrast medium under ERCP, careful consideration of biliary imaging allows detailed planning and successful execution of the palliative procedure. If endoscopic palliation of obstructive jaundice is considered, a decision should be made regarding the size and type of biliary stent. Relief of jaundice due to malignant distal bile duct obstructions requires introduction of large 10 to 11.5 Fr plastic stents or SEMSs inserted with a duodenoscope using a 3.8 mm or 4.2 mm working channel. Initial insertion of a 10 Fr plastic stent is recommended if the diagnosis of malignancy is not established or if expected survival is <4 months. Whatever stent is to be used, a standard 0.035-inch guidewire through the catheter is inserted across the stricture to be stented into the bile duct and its tip passed into an intrahepatic duct. Biliary sphincterotomy is not necessary for placement of a single plastic biliary stent or a SEMS in transpapillary position. It is nevertheless routinely performed before stenting by some endoscopists possibly in order to facilitate stent exchange during follow-up, or for cases requiring more than one biliary stent placement.14 While plastic stents are inserted using a three layer coaxial system, consisting of guidewire, inner guiding catheter and pusher tube/stent, SEMSs are placed over the standard guidewire. The stents must be positioned and released accurately through the tumor under fluoroscopic and endoscopic guidance. The distal part of the SEMS should protrude about 1 cm into the duodenum to allow easy endoscopic access, in case it is needed for the restoration of patency of occluded stents.8 If conventional endoscopic stenting fails despite best efforts, PTC can then be performed for percutaneous biliary drainage with/without stenting or a percutaneous endoscopic biliary stenting for conversion into the endoscopic biliary drainage.
Plastic versus metal stents
Both plastic stents and SEMSs can be used for the palliation of malignant distal bile duct obstructions. Plastic stents are relatively less expensive compared to SEMSs, and can be removed and replaced easily if they become occluded. However, the diameter of plastic stents is limited up to 12 Fr by the working channel size of the duodenoscope. Plastic stents have limited stent patency because they have relatively narrow lumen and easily become occluded with biliary sludge and/or bacterial biofilm comprising of protein, bilirubin, bacteria and amorphous debris.15 Stent occlusion usually leads to recurrent biliary obstruction accompanying jaundice and/or ascending cholangitis. In case of cholangitis or decrease in total bilirubin level by <20% from baseline at 7 days post stent insertion, biliary imaging or endoscopic revision should be considered.14
Plastic stents of 10 to 11.5 Fr have patency rates of approximately 3 months but smaller diameter stents have significantly lower patency rates and should not be routinely placed for palliative drainage.16 Plastic stents measuring no smaller than 10 Fr in diameter and possibly certain stent designs, such as the DoubleLayer stent and stents with an anti-reflux valve, provide the longest biliary patency, but using a 11.5 Fr model or drug administration has not shown a more prolonged stent patency.14 Two strategies have been employed against to plastic stent occlusion, including management of management of expectant episodes of stent occlusion and prophylactic scheduled exchange at 3-month intervals in order to prevent the risk of subsequent cholangitis. Prophylactic plastic stent changes improve symptom-free survival compared to stent change at signs of stent occlusion. However, with prophylactic plastic stent changes, patients who live more than 6 months are likely to be affected by the expenses and patient compliance for repeated stent changes is needed.17
SEMSs were developed to overcome the diameter limitation of plastic stents as they deliver stents with as larger diameter as up to 30 Fr or 10 mm, when deployed, using a relatively smaller delivery system of 7 to 8 Fr, facilitating easier passage across the biliary strictures. This larger diameter facilitates biliary flow and improves patency rates.18 The comparison studies between plastic and SEMSs at ERCP concluded that the patency rates of SEMSs were superior to those of plastic stents for distal biliary obstruction, with 10 to 12 months vs. 3 to 4 months.17-20 Because unresectable malignant biliary obstruction is typically associated with survival of less than one year, SEMSs are intended to yield palliation of obstructive symptoms throughout the remaining lifespan of these patients.18,21,22 Although SEMSs are more expensive and there is no significant difference in the survival time between plastic and SEMSs, recent European Society of Gastrointestinal Endoscopy guidelines recommend insertion of SEMS, 10 mm in-diameter, in patients with an established diagnosis of malignancy as the prime stent, whether expected survival time is >4 months or if the cost of the SEMS itself is <50% than that of ERCP procedure.14 This is due to superior stent patency, decreased need for repeated ERCP to manage recurrent jaundice, shorter hospital stays, reduced duration of antibiotic treatment, and fewer complications.17,23
Early complications develop in approximately 5% of patients after endoscopic biliary stenting is attempted, including infection, pancreatitis and bleeding, regardless of the stent type used. Complications were distributed as follows: biliary infection (35%), pancreatitis (29%), bleeding (23%), perforation (6%), early stent migration (3%), and renal failure (3%). Of the commercially available plastic biliary stents, Teflon-made stents of the Tannenbaum or Amsterdam type result in a significantly lower short-term success rate, defined by decreasen levels of jaundice, serum bilirubin or pruritus, but similar morbidity and 30 day mortality rate, as compared with polyethylene-made stents.14 Late complications of biliary stenting mostly consist of stent dysfunction, which is approximately twice more frequent with plastic stents compared to SEMS, followed by much less frequent cholecystitis, duodenal perforation and bleeding ulcer. Approximately 5% of plastic stents and partially covered SEMS migrate while 1% of uncovered SEMS and 20% of fully covered SEMS migrate.14 SEMSs may still eventually become occluded with tumor ingrowth, tumor overgrowth, epithelial hyperplasia or biliary sludge. Insertion of a second SEMS within the occluded SEMS yields a longer biliary patency than inserting a plastic stent, particularly if one of the two SEMSs (initially placed or placed for treating stent dysfunction) is a covered stent. However, in cases where the life expectancy is Ōēż3 months, insertion of a plastic stent would suffice.14 Another major limiting factor of uncovered SEMSs is that they cannot be removed any other way than by operation. So tissue confirmation of cancer should always be obtained before placement of the SEMSs.24
Covered versus uncovered metal stents
Uncovered stents are made from stainless steel, cobalt based alloy, or nickel-titanium (nitinol) alloy and are designed with a wire mesh. Covered stents were developed to overcome tumor ingrowth through the wire mesh and have non-porous covering membranes, such as polyurethane, silicone, or expanded polytetrafluoroethylene. The covering may extend over the entire length of the stent (fully covered SEMS), or small areas at the ends may be left uncovered (partly covered SEMS). Although they prevent tumor ingrowth, overgrowth still remains a problem. The long-term durability of the covering membrane is sometimes problematic, because the covering membranes can be damaged during deployment or degradation due to reflux of the duodenal and gastric juices.25 Tumor ingrowth in patients using covered SEMSs has the possibility of occurring through the tear of the covered membranes. Other potential problems of the covered SEMSs include encrustation of bile, stent migration, or occlusion of the cystic duct, pancreatic duct, or lateral branches of the bile ducts. There was no significant difference in the incidence of cholecystitis between covered and uncovered SEMSs.26-28 Neoplastic involvement of the cystic duct and gallbladder stones are the key risk factor for SEMS-related cholecystitis.14 While several studies of covered SEMSs reported relatively high incidence of acute pancreatitis (5.6-6.1%),26,29-31 recent analysis of prospective randomized trials comparing covered and uncovered SEMSs showed no difference in the rate of pancreatitis.32 Each 5-mm length bare meshed end of covered SEMSs allows embedding into the tissue to reduce the risk of migration. They were originally introduced in an attempt to improve patency rates of covered SEMS compared to the uncovered SEMSs. However, non-randomized comparison studies comparing covered and uncovered Wallstents in unresectable distal malignant biliary obstruction did not show differences in stent patencies or complication rates.26,33 Two recent prospective randomized trials also failed to show a difference in stent patency between covered and uncovered SEMSs when they were placed endoscopically,34,35 with an exception of one study of uncovered vs. non-commercially available covered diamond stents.36 Further well-designed large scale randomized prospective studies are needed to identify the benefits and indications of covered stents.
PALLIATION FOR MALIGNANT HILAR OBSTRUCTION
Resectability of malignant hilar obstructions should be evaluated by imaging techniques in the absence of biliary stents. Palliative treatment in patients with unresectable malignant hilar obstruction clearly has an important role, because 80% of these are unresectable and a risk of recurrence is high even in those undergoing resection.37,38 Being more difficult, requiring higher degree of expertise, and carrying considerably higher morbidity and mortality rate, unresectable malignant hilar obstruction represents a significantly greater challenge both technically and in decision making, than in malignant distal bile duct obstruction.39 More than 90% of unresectable malignant hilar obstructions have obstructive cholestasis and therefore restoration of bile flow is one of the main objectives of palliative treatment.40 A median survival of 6 to 9 months for unresectable hilar tumors implies that durable palliation should be one of the major objectives of treatment plan.40 An ideal palliative procedure should be simple and effective in relieving obstructive cholestasis, have low procedure-related morbidity and mortality, and offer durable palliation.24 In general, when appropriate expertise is available, endoscopic palliation has been considered as the treatment of choice for palliation of unresectable malignant hilar obstruction, because it allows definitive internal drainage in single procedure. Combined percutaneous and endoscopic procedures or percutaneous drainage alone are used in hilar tumors either after the failure of the endoscopic procedure or for further non-surgical intervention where obstructive cholestasis fails to be resolved after the endoscopic procedure. Endoscopic biliary drainage can be achieved with either plastic or metal stents, but patency rates of biliary stents are generally lower with malignant hilar obstructions, compared with malignant distal bile duct obstructions.41 The still remaining questions are whether to use one or multiple stents, and plastic or metal stents for endoscopic palliation.
Technique of endoscopic biliary stenting
One of the important technical considerations during biliary stent insertion in malignant hilar obstruction, is that initially it is imperative not to inadvertently inject contrast medium above the level of the hilar stricture into unintended multiple hepatic segments, because it frequently leads to postprocedure cholangitis. Therefore, the hepatic segment(s) requiring drainage should be carefully pre-selected before beginning ERCP with the aim of draining more than 50% of the liver volume in malignant hilar obstructions, based on an adequate cholangiogram obtained through either magnetic resonance (MR) or computed tomography (CT) scan.42 Every effort is done to carefully inject contrast medium only into the obstructed ducts that are intended to be drained, for example by injecting contrast medium after deep catheter insertion into the stricture of interest or by using contrast-free cannulation.43,44 The upstream bile duct(s) unintentionally opacified with contrast medium should be drained during the same procedure and antibiotics should be administered in case of suspected incomplete biliary drainage. Although no difference in efficacy has been shown between single stent placement in the left or right hepatic lobe,45 the left hepatic segments are drained preferentially if a single stent is to be placed. This is due to the longer length of the left main hepatic duct before branching, which leads to larger volumes of the liver being able to be drained, resulting in a more effective drainage than the right. Since the right system is more variable with earlier branching and multiple segment obstructions are more common, a right sided stent is more likely to drain only a limited portion. After a biliary stent is inserted, biliary balloon dilatation may be helpful for hilar strictures particularly when bilateral stenting is being attempted.
Bilateral stenting is technically challenging. The first stent is endoscopically placed in either the left or right hepatic duct whichever is more difficult to access first. The left stent is usually placed first as it is more difficult to access compared to the right stent. There are two techniques for endoscopic placement of bilateral SEMSs; one is the 'side-by-side' (SBS) stenting technique and the other is the 'through-the-mesh' (TTM) stenting or 'stent-in-stent' technique (Table 1). The SBS technique is an endoscopic procedure for bilateral plastic or metal stenting with sequential delivery of two or more parallel plastic stents or SEMSs, to drain both intrahepatic bile ducts after multiple guidewire placements. It can be extremely difficult or unavailable despite best efforts in patients with unresectable hilar tumors. Once a SEMS is deployed endoscopically within the biliary tree, passaging a second SEMS alongside the initial stent is not technically easy because the first stent expands to completely occupy the bile duct lumen. So this technique usually demands prior dilatation. Strategies to overcome this difficulty for bilateral metal stenting include the following: SBS insertion of two delivery catheters (Ōēż6 Fr) followed by simultaneous deployment of both SEMSs;46 a rapid SEMS insertion sequence, inserting the second SEMS assembly while the first SEMS is being deployed; having the first SEMS traverse the papilla; or inserting a temporary plastic stent.14,47 On the other hand, the TTM technique is an alternative endoscopic procedure that allows bilateral metal stenting placed in a Y-configuration, in which a second stent traverses through the open-mesh wall of the initial stent to enter the opposite hepatic lobe. During this procedure, attempts to pass a second metal stent through the mesh of the indwelling initial conventional metal stent can be technically problematic, due to the tightly woven structure of the stent wire mesh. Even if a taper-tipped catheter, hydrostatic balloon, or a 7 Fr Soehendra stent extractor is used to widen the smaller-mesh wall of the initial stent, it is still proved difficult to permit passage of the second stent during an ERCP.48 Strategies to facilitate this procedure include the following: balloon dilation of the contralateral hepatic duct immediately before inserting the first stent to ease TTM cannulation of the contralateral duct; dilation of the cannulated first stent mesh by means of a balloon before inserting the second stent; or use of a specific SEMS with a wider mesh opening.17
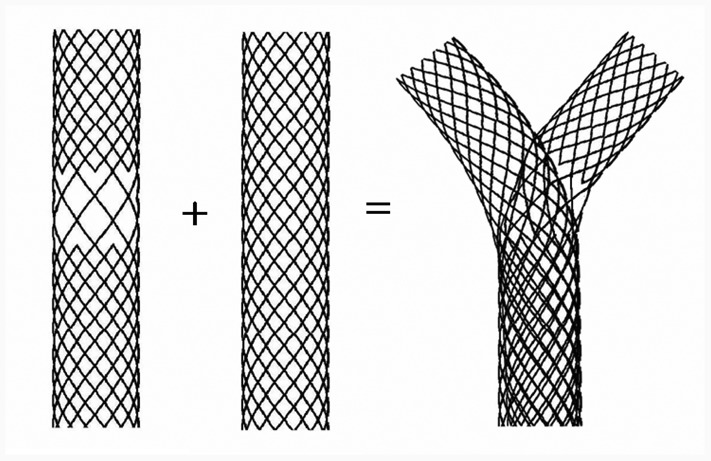
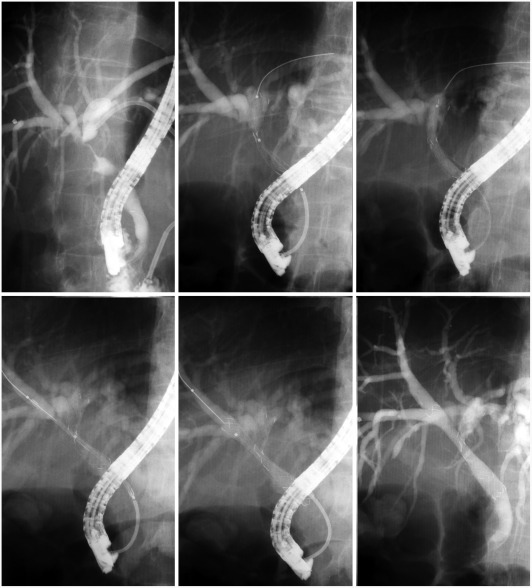
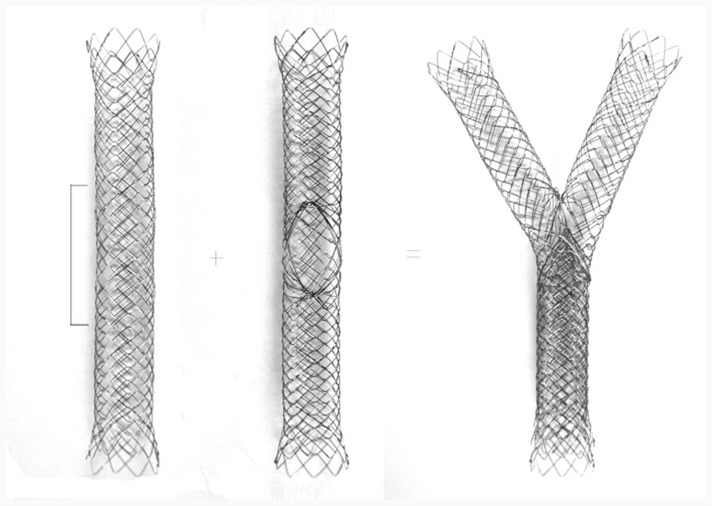
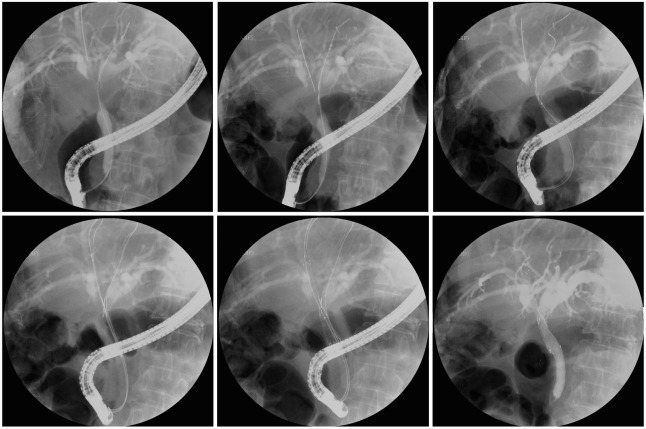
For overcoming such technical difficulty in the TTM technique using conventional metal stents, several kinds of newly designed SEMSs have been recently introduced to facilitate passage of the second metal stent during bilateral stenting. One of them is a Y-stent (Y type biliary Niti-S stent; Taewoong Inc., Seoul, Korea) with a wider-mesh portion in the center and smaller-mesh portions on both ends.49,50 The joining of the Y-stent and conventional metal stent through the wider-mesh portion of the Y-stent produces a Y-shaped arrangement (Fig. 1). First Y-stent is endoscopically placed through the hilar stricture into the intrahepatic bile duct, and then the second conventional biliary metal stent is advanced over the guidewire from the inside of the Y-stent through the central wider-mesh portion into the contralateral intrahepatic duct, and released to form a Y-shape. The large opening in the wider-mesh wall of the first Y-stent permits easy passage of the delivery catheter for the second stent and its wide expansion (Fig. 2). More than two metal stents, including multiple Y-stents, can be inserted in sequence using the TTM technique in order to drain multiple hepatic segments. The two main drawbacks of this Y-stent are; first, later endoscopic access to both stents is often impossible after stent occlusion; secondly, the wider-mesh structure in the center causes an increasing tendency of tumor ingrowth and poor stent expansion due to the weak radical force.
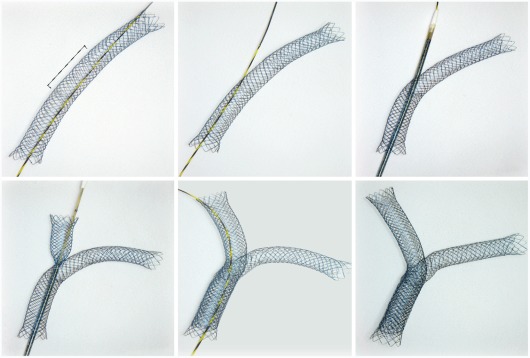
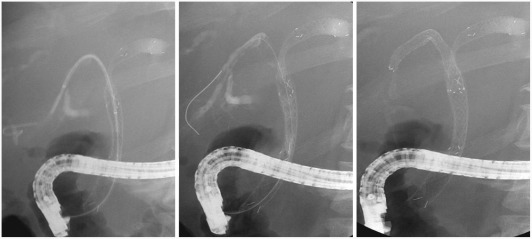
Other types of metal stents (M-Hilar stent and K-Hilar stent; Standard Sci-Tech Inc., Seoul, Korea) for bilateral stenting have been developed to overcome the drawbacks of the Y-stent as described above.51 The M-Hilar stent has been designed with a differently woven structure in the center, which permits easy passage of the delivery catheter of the second stent, even though it has no wider-mesh portion (Figs. 3, 4). The K-Hilar stent is another special stent with a large hole in the center of the stent (Figs. 5, 6). When this particular stent is used as the second stent during bilateral stenting, lumens of both stents are absolutely patent without blockage of the wire mesh. Therefore, endoscopic re-intervention with plastic stents can be easily performed in cases where these new Y-stents were used.
Unilateral versus bilateral biliary stents
Single stents are adequate for Bismuth type I hilar tumors, which have strictures of the main bile duct below the confluence. However, there is significant controversy as to whether single or multiple stents should be inserted for Bismuth type II, III, and IV hilar tumors. The decision of whether to place single or multiple bilary stents depends on the location and extent of the stricture in the biliary tract as well as the degree of biliary contamination.6 It is well known that only 25% of the liver volume needs to be drained for adequate palliation of obstructive cholestasis showing improvement in biochemical parameters11,53 and draining >50% of the liver volume is associated with a higher drainage effectiveness and longer survival than draining <50%.17 A single biliary stent into one functional liver lobe for unilateral drainage can provide adequate palliation in a major portion of patients with hilar tumors, and many studies have reported good results using a single stent in about 80% of patients with Bismuth type II and III hilar tumors.54,55
Sometimes, however, bilateral biliary stents may be needed for palliative drainage of both hepatic lobes when both sides are contaminated, when a non-dominant or atrophic lobe was inadvertently stented without efficacy, or if bilateral brachytherapy is scheduled.56 Especially the vigorous opacification of multiple bile ducts of both hepatic lobes, to obtain detailed cholangiograms with contrast during ERCP, increases the necessity for bilateral stent insertion in hilar tumors, because cholangitis mainly arises from contaminated and undrained bile ducts. Drainage of both systems during ERCP is actually to prevent postprocedure cholangitis rather than to have effective palliation. If both lobes are imaged with contrast during ERCP, bilateral stent insertion reduces the potential sequelae of cholangitis in undrained bile ducts. However, even in the most experienced hands, endoscopic placement of bilateral stents may be difficult or impossible, and failure of bilateral stenting after extensive contaminated contrast filling of multiple bile ducts may frequently lead to subsequent cholangitis. If contrast medium does not contaminate both sides or is sufficiently drained from unilateral bile duct after imaging both sides, then unilateral stenting should be enough and is substantially easier to perform endoscopic re-intervention.
Several studies have attempted to address whether unilateral or bilateral drainage is preferred for palliation of obstructive jaundice in patients with hilar tumors.5,55,57,58 Early studies have shown high rates of cholangitis following ERCP in large parts attributed to the contamination of the undrained segments which was caused by contrast injection without any planned limitations.5,57 These studies showed that bilateral stent insertion was associated with an increased survival rate and reduced risk of cholangitis, compared to unilateral drainage for Bismuth type II and III hilar tumors.57 The highest survival rate was noted in patients with hilar tumors who had bilateral drainage, while the lowest survival rate in those who showed cholangiographic opacification of both lobes but only unilateral drainage was available.5 These results are believed to have been caused by inadvertent contrast injections into the undrained bile ducts and quite clearly show that failure to drain an opacified lobe leads to a significantly negative outcome, thus bilateral drainage being mandatory if both hepatic lobes are opacified. However, an unsuccessful attempt at bilateral drainage can lead to increased incidence of postprocedure cholangitis and lower survival rates.44,54 Therefore, ERCP in hilar tumors should only be undertaken in highly regarded institutions with high success rates for drainage of hilar obstruction.
Selectively targeted and planned endoscopic drainage guided by MR cholangiography or CT imaging has recently been introduced to reduce inadvertent contrast injections into atrophied and/or unintended multiple hepatic segments, resulting in a lower incidence of postprocedure cholangitis.15,44,55,58,59 MR findings seem to be slightly more accurate than CT findings in assessing the level of obstruction in malignant hilar obstructions and measuring the volume of functional liver lobes. MR cholangiography is widely known as a reliable and noninvasive diagnostic tool and shows equivalent imaging to that of ERCP in demonstrating the detailed anatomy of the biliary tree. Several advantages of MR cholangiography over ERCP include noninvasive diagnostic tool, no use of contrast medium and the delineation of missing ducts which are not visible on the endoscopic cholangiogram due to complete obstruction of the bile ducts. Cholangiograms obtained from MR provide a road map for the biliary endoscopist to define the biliary anatomy prior to ERCP, and allow them to choose the optimal hepatic lobe and bile ducts for effective drainage.15,44,55,58 Nowadays MR cholangiography has led to the unnecessary need for a diagnostic ERCP and is rapidly replacing its role for the delineation of the biliary tree, therefore ERCP is becoming an unnecessary procedure for such diagnostic purposes in hilar tumors. ERCP for hilar obstruction can be undertaken mainly for the therapeutic purpose of endoscopic intervention such as stenting into the targeted bile duct with the help of MR cholangiography. Several studies have evaluated the role of MR-guided selective unilateral biliary stent placement for endoscopic palliation of hilar tumors, and showed that the use of MR cholangiography to plan a layout of the intended endoscopic placement of the stent, reduced the need to inject contrast medium into multiple segments during ERCP, and thus diminished the risk of postprocedure cholangitis.44,58-60
Plastic versus metal biliary stents
A plastic stent has been commonly used to achieve biliary drainage in patients with a malignant hilar obstruction. However, the use of plastic stents for the palliation of hilar tumors revealed poor results in some series.56,61 Plastic stents in the hilar stricture have limited stent patency due to their narrow lumen and a higher chance of stent clogging due to the longer length of the stent used. Stent occlusion frequently results in cholangitis with rates as high as 20% to 40% reported for unilateral or bilateral plastic stents due to bacterial contamination of undrained bile ducts.56,61 Other disadvantages of plastic stents include that it is technically difficult to place more than one 10 Fr stent at the initial setting and plastic stents in hilum are prone to distal migration.6
SEMSs are increasingly favored, although individually more expensive. A larger diameter of SEMSs may potentially result in improved stent patency as compared with that of plastic stents, thus requiring fewer repeated procedures.20,60,62 In addition, there are some theoretical advantages of metal stents in hilar tumors, including the open-mesh design, which allows drainage of secondary branches through the side of the stent and less likelihood of obstructive segmental cholangitis.63 When single lobe drainage is planned, insertion of an uncovered metal stent is preferred to prolong patency, and to avoid occlusion of branch ducts which is more likely with a plastic stent. Although little data is available on hilar tumors, the current evidence favors the placement of SEMSs as they provide a superior palliation in comparison to plastic stents in terms of early and late complications.5,64 Insertion of SEMS is especially recommended in patients with a life expectancy of >3 months or with biliary infection. The initial higher cost is offset by lower incidence of re-intervention and hospitalization for complications.61 However, a major limiting factor of SEMSs is that they cannot be removed other than surgically.24 So plastic stent placement for the palliative therapy can be recommended if diagnosis is clinically ambiguous or SEMS placement is impossible. Covered metal stents are not appropriate for hilar strictures as intrahepatic side branches can be inadvertently obstructed.65
CONCLUSIONS
Palliative management of patients with unresectable malignant biliary obstructions is challenging for all biliary specialists, because there is no single correct approach for it and there are several controversies in choice of therapies according to the location and extension of tumors. For palliation of malignant distal bile duct obstructions, an endoscopic approach should be initially used with percutaneous radiological intervention reserved for its failures. For palliation of malignant hilar obstructions, the endoscopic approach has also been considered as the treatment of choice when performed by an appropriate expertise, although percutaneous approaches may vary depending on the institution. There is still a lack of clear consensus on the use of covered versus uncovered metal stents in malignant distal bile duct obstructions and plastic versus metal stents and unilateral versus bilateral drainage in malignant hilar obstructions. This decision should be made on an individual basis, till acceptable results are found in randomized, controlled trials further evaluating these therapies. For future advanced biliary stents, drug-eluting SEMSs would particularly be appealing for the treatment of malignant biliary obstruction although they are not commercially available for biliary use yet, and currently radioactive SEMS and bioabsorbable self-expanding stents are being tested in animal models.