Usefulness of Endoscopic Ultrasound in Esophagogastric Varices
Article information
Abstract
Endoscopic ultrasound (EUS) is a useful diagnostic tool for evaluation of esophagogastric varices and guidance of endoscopic therapy. EUS can visualize not only collateral veins around the esophagus but also perforating veins that connect esophageal varices with collateral veins. They are associated with high risk of bleeding and early recurrence after initial variceal eradication. Isolated gastric varices can be easily diagnosed using EUS that mimic thickened gastric folds or subepithelial tumors. EUS-guided endoscopic therapy is a challenging field of variceal bleeding. It has a potential role for assistance of interventions and evaluation of treatment outcome.
INTRODUCTION
Endoscopy has a critical role in acute esophageal variceal bleeding.1 Endoscopic injection sclerotherapy and band ligation has been proven to be effective in prevention and control of acute variceal bleeding. Recently, endoscopic ultrasound (EUS) has shown its potential for evaluation of gastroesophageal varices.2 During endoscopy, EUS with a miniaturized ultrasonography can be performed. EUS with conventional echoendoscope equipped with doppler can also be performed before endoscopic therapy. EUS shows a cross-section of esophageal varices and the changes in collateral veins around the esophagus. Perforating veins connect the varices with collateral veins through the esophageal wall. These veins are associated with early recurrence or bleeding of esophageal varices.3,4 Prediction of variceal recurrence or aggravation after variceal eradication would be improved, if EUS might be used for evaluation of the perforating veins.
VISUALIZATION AND EVALUATION OF GASTROESOPHAGEAL VARICES
Increased portal pressure can develop collateral veins around the distal esophagus and stomach. EUS can detect vascular changes of these areas in an early stage. A high-frequency (20 MHz) endoluminal miniature probe facilitated greater resolution of submucosal vessels and esophageal varices.5 During conventional endoscopy, EUS can be performed easily by introduction of the miniature probe through a biopsy channel. Endoscopic view of esophageal varices is well correlated with EUS finding (Fig. 1). Miller et al.6 showed EUS can measure the severity of esophageal varices by summing the cut-surface area with digitized image. The measured area was well correlated with risk of bleeding. EUS allows detection of early changes in submucosal veins in the cardia and fundus of the stomach (Fig. 2). Small gastric varices that mimic thickened gastric folds can be easily differentiated. The thickness of the variceal wall and hematocystic spots can be evaluated with EUS.7 Duodenal varices or isolated gastric varices other than the fundus are rare. The diagnosis of rare gastrointestinal varices can be difficult but EUS can make it easy revealing hypoechoic tortuous tubular structures in the submucosal layer.8

Esophageal varices. (A) Endoscopic image shows large esophageal varices. (B) Endoscopic ultrasound image shows esophageal varices (arrowheads) using a miniature probe (20 MHz) in the same patient.
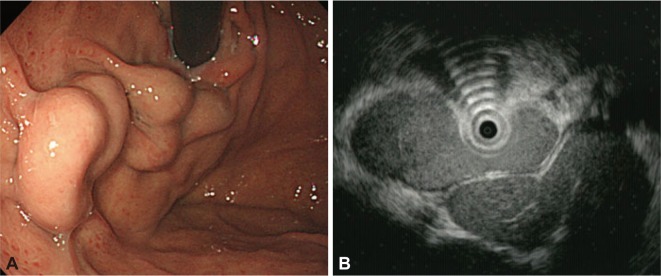
Gastric varices. (A) Endoscopic image shows large varices in the stomach. (B) Endoscopic ultrasound image shows same gastric varices. A tortuous hypoechoic tubular structure is seen in the submucosal layer.
CHANGES IN COLLATERAL VEINS AROUND THE ESOPHAGUS
Peri-esophageal collateral veins (peri-ECVs) are small veins adjacent to esophageal wall. Para-ECVs are larger veins located on the outer side of esophageal wall, which are connected to the superior vena cava through the azygos vein (Fig. 3).2 Large collateral veins were associated with higher risk of variceal bleeding and recurrence of varices following endoscopic treatment.3,9,10 EUS can visualize and evaluate these collateral veins around the esophagus in patients with portal hypertension. EUS also allows visualization of the left gastric vein. The diameter of the left gastric vein is associated with variceal size.11 The azygos vein drains blood from the esophagus to the superior vena cava and may become enlarged due to aggravated portal hypertension.12 With EUS, azygos vein diameter and valuable quantitative and qualitative data including blood flow volume index can be obtained.13
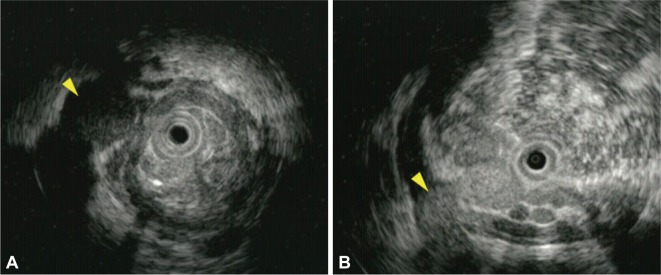
Endoscopic ultrasound images of collateral and perforating veins. (A) A collateral vein outside of the esophageal wall is seen (arrow head). (B) A perforating vein (arrowhead) that connects a collateral vein with an esophageal varix is seen.
PERFORATING VEINS
Perforating veins connect esophageal varices to collateral veins outside of the esophageal wall (Fig. 3). Although ECVs could be visualized by computed tomography or magnetic resonance imaging, small perforating veins can be detected only by EUS. Large esophageal varices with high risk of bleeding have correlation with the number and size of perforating veins.14 Large perforating veins were more frequent in large varices. When blood flow in a perforating vein was studied using color doppler, 45% to 88% of perforating veins exhibited inflow from the collateral veins into the varices.4,15 Most perforating veins, particularly in large esophageal varices, seem to be associated with aggravation or recurrence of the varices.
EVALUATION OF TREATMENT RESPONSE AND PREDICTION OF REBLEEDING
Before endoscopic therapy, knowledge of the inflow pattern of the varices might be useful to make a treatment plan. Esophageal varices drain portal blood flow from the cardiac submucosal veins or perforating veins. If the varices receive blood from only the cardiac veins, endoscopic treatment should be focused in the cardia and esophagogastric junction. This cardiac inflow pattern of esophageal varices was seen in 60% of cirrhotic patients.16 Large collateral veins and perforating veins might be connected to the esophageal varices. Previous studies showed large para-ECVs (>5 mm) were associated with high rates of variceal recurrence and rebleeding.17,18 The increased risk of bleeding seems to be associated with large perforating veins. Therefore, the high-risk patients need more intensive treatment and close follow-up.3,19 The anterior branch of left gastric vein was associated with poor response to endoscopic treatments.20 The morphology and blood flow of the vein can be evaluated with color Doppler EUS.
ASSISTANCE IN ENDOSCOPIC THERAPY
Under EUS guidance, injection of sclerosant can be done confidently into esophageal varices. This procedure might decrease the recurrence rate of esophageal varices after the endoscopic therapy.21 A randomized controlled study showed EUS-guided injection sclerotherapy is safe and effective as compared with injection therapy alone in the treatment of esophageal varices.2,22
Endoscopic therapy is not easy to perform in patients with bleeding gastric varices. EUS can guide injection of cyanoacrylate into gastric varices and evaluate the success of the treatment. Transesophageal EUS-guided coil and cyanoacrylate glue treatment of gastric fundal varices was successful in a report.23 Remnant varices are easily visualized by EUS. Recently, successful EUS-guided glue injection was reported.24,25
CONCLUSIONS
EUS can be used for evaluation of not only gastroesophageal varices but also perforating and collateral veins outside of the esophagus. Perforating veins might be associated with large varices, early recurrence, or rebleeding. Evaluation of perforating veins and detailed imaging of collateral veins increased our understanding of esophageal varices. EUS is useful for early diagnosis of varices, assessment of the risk of bleeding, and prediction of early recurrence in patients with portal hypertension. EUS guided variceal treatment deserves further study to determine if it can improve safety and efficacy over conventional endoscopic injection therapy.
Further studies are also required to demonstrate conclusively the role of EUS in improving the survival of patients with esophageal varices.
Notes
The author has no financial conflicts of interest.