INTRODUCTION
Endoscopic mucosal resection (EMR) is an endoscopic alternative to surgical resection of mucosal and submucosal neoplastic lesions and intramucosal cancers. EMR offers both diagnostic and therapeutic capability. Lesions limited to the mucosa and the superficial layers of the submucosa appear to be the most amenable to endoscopic cure. The techniques for EMR can be broadly divided into two groups: suction and non-suction techniques.
This topic will provide an overview of useful accessories for colorectal EMR such as cap and band.
CAP-ASSISTED COLONOSCOPY
This technique is most commonly performed with a transparent cap (disposable distal attachment; Olympus, Tokyo, Japan) attached to the tip of the endoscope. Cap-assisted colonoscopy (CAC) uses a transparent plastic hood attached to the tip of the colonoscope to flatten the semilunar folds and improve mucosal exposure. Several studies have examined that CAC facilitated shortening of the cecal intubation time in difficult cases, and was more sensitive for detecting adenomas than was conventional colonoscopy.1,2 A meta-analysis and systemic review suggests that a transparent cap on the end of the colonoscope may give a marginally faster cecal intubation time compared with standard colonoscopy. It also suggests that there is a better polyp detection rate and less pain with the cap.3,4
CAC may reduce the time required for colonoscopic EMR of each polyp and may also improve the polyp detection rate.5
COLORECTAL EMR USING A CAP
This technique is most commonly performed using a distal attachment fitted to the distal end of the endoscope, with saline solution with a low concentration of epinephrine injected underneath the lesion. The lesion was snared and drawn into the cap using the suction function of the endoscope, and then ligated and resected using electrocautery. The most serious complication of this technique may be perforation due to the lack of submucosal saline injection and too much suction. Therefore, large volume injection, which creates a large bleb and potentially reduces the risk of perforation, is recommended.6
Moreover, EMR using a cap (EMR-C) is effective at removal of carcinoid tumor which is diagnosed increasingly each year. It is widely accepted that rectal carcinoid tumors with a diameter of 10 mm or less can be treated with local excision, including endoscopic resection.7 Complete resection of rectal carcinoid tumors, however, is difficult to achieve with conventional endoscopic resection techniques because these tumors often extend into the submucosa.
Resection via polypectomy or conventional EMR is often associated with resection margin involvement, which necessitates further intervention.8,9 The rate of positive resection margin for tumor is lower in the group of EMR-C than conventional polypectomy group.10-12
And secondary endoscopic treatment for remnant lesions of rectal carcinoid tumors after primary EMR or polypectomy is technically difficult because of fibrosis of the residual tissues. EMR-C, a method to resect the submucosal layer by suction by using a transparent cap, may be feasible as a salvage treatment. 13
COLORECTAL EMR WITH A LIGATION DEVICE (OR ENDOSCOPIC SUBMUCOSAL RESECTION WITH A LIGATION DEVICE)
A variation of the suction technique is the band and snare procedure. During the band (endoscopic ligator; Conmed, New York, NY, USA) and snare procedure, tissue is banded using an esophageal variceal banding device and then snared off in the standard fashion.14
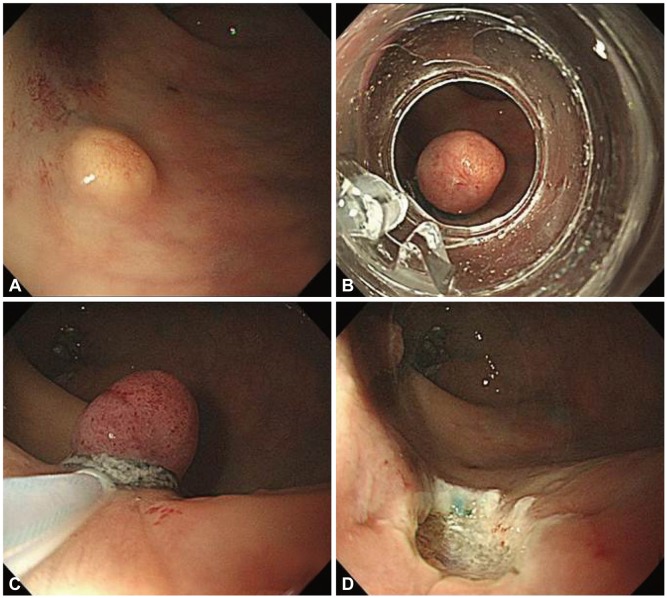
After submucosal injection beneath the lesion to elevate it away from the muscularis propria, the lesion was aspired into the ligator device and the elastic band was then deployed. Next, snare resection was performed below the band with a blended electrosurgical current (Fig. 1). The resection specimen was then removed by aspiration into the cap or by retrieving it with a grasping forceps. After resection of the specimen, the ulcer floor was endoscopically closed with clips to prevent postoperative bleeding and perforation. As with EMR-C, complete resection of rectal carcinoid tumor is important but is difficult to achieve with conventional endoscopic resection techniques because these tumors often extend into the submucosa. Resection via polypectomy or conventional EMR is often associated with resection margin involvement. Among various endoscopic resection techniques, endoscopic submucosal resection with a ligation device (ESMR-L) is known to be a useful and safe procedure.15-19