Endoscopic Resection of Giant Colonic Lipoma: Case Series with Partial Resection
Article information
Abstract
Colonic lipoma, a very rare form of benign tumor, is typically detected incidentally in asymptomatic patients. The size of lipoma is reported variously from 2 mm to 30 cm, with higher likelihood of symptoms as the size is bigger. Cases with symptom or bigger lesion are surgically resected in principle; endoscopic resection, which has developed recently with groundbreaking advance of endoscopic excision technology, is being used more often but with rare report of success due to high chance of complications such as bowel perforation or bleeding. The authors report here, together with a literature review, our experiences of three cases of giant colonic lipomas showing complete remission after aggressive unroofing technique, at certain intervals, using snare catheter at the origin of the lipoma so that the remaining lipoma could be drained out of the exposed surface spontaneously, in order to reduce complications.
INTRODUCTION
Colonic lipoma is the second most common, but very rare, tumor after colon polyps.1 Although most cases are found incidentally in asymptomatic patients, some cases may present with symptoms such as abdominal pain, diarrhea, intestinal obstruction and bleeding. The reported size of lipoma varies from 2 mm to 30 cm, with increased likelihood of having symptoms as the size is bigger.1-3 Patients with a larger lesion or symptomatic patients require treatments. Surgical resection has been considered better suited for giant (≥2 cm) lesions than endoscopic management, which is highly likely to cause complications such as perforation or bleeding in a giant lesion. With recent breakthrough in endoscopic excision technology, however, reports of successful endoscopic management is increasing even for giant lesions.4-6 Two endoscopic methods to manage lipoma, complete resection and partial resection (including unroofing technique), have been reported.7-9 The difference of effectiveness between these two methods is not proven,9 but partial resection is thought to be much safer than complete resection due to lower chances of complication. Now, we report our experiences of three cases of giant colon lipoma that were cleared up after partial resection, together with a literature review.
CASE REPORTS
Case 1
A 65-year-old female was referred to our center due to a giant colon lipoma detected on a colonoscopy. The patient had intermittent abdominal discomfort in the right lower quadrant. A wide-based 3×3-cm size yellowish protruding mass without mucosal change was detected at the ileocecal valve during colonoscopy (Fig. 1A). We planned to perform an unroofing technique with a snare catheter (ASM-1-S; Wilson-Cook Medical Inc., Winston-Salem, NC, USA) at the center of the lesion so that the remaining lipoma could flow out of the exposed surface. It was deemed as appropriate to remove the roof of the center because the wide base of the lipoma could impede the conduction of electric current. ERBE ICC 200 (Elektromedizin, Tubingen, Germany) was used as the electrosurgical unit; at the Endo-cut mode (120 W, effect 3), partial resection was performed twice, each time lasting for less than 5 seconds, to resect about half of the mass (Fig. 1B, C). Typical yellow tissue indicating lipoma could be seen on the exposed surface (Fig. 1D). The patient was relieved of the abdominal discomfort afterwards. At 3-year follow-up colonoscopy, a surgical scar was observed but not any remaining lipoma (Fig. 1E).
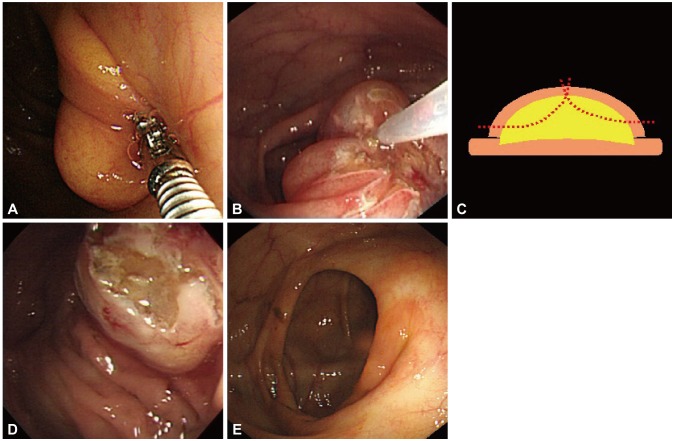
Endoscopic resection of a giant colon lipoma, case 1. (A) A wide-based 3×3-cm yellowish protruding mass without mucosal change detected at the ileocecal valve during colonoscopy. (B) Partial resection with unroofing technique performed twice at the center of the lesion using snare catheter (ASM-1-S; Wilson-Cook Medical Inc.). (C) A simplified illustration of the procedure. (D) Half the mass is resected, and yellow tissue can be observed on the exposed surface of the remaining lesion, indicating typical lipoma. (E) Three-year follow-up colonoscopy. There's no remaining evidence of the lipoma, except for the surgical scar.
Case 2
A 46-year-old female was referred to the center with a colonoscopic finding of 3×3 cm giant lipoma at the sigmoid colon during a health examination performed 3 years ago. Being asymptomatic, the patient had been followed on an outpatient basis but was referred to our center due to continued abdominal discomfort in the left lower quadrant. A wide-based 3×3-cm yellowish globular mass without mucosal change was detected 30 cm above the anal verge during colonoscopy (Fig. 2A). Partial resection technique was performed with a snare catheter at the center of the lesion so that the remaining lipoma could flow out of the exposed surface (Fig. 2B, C). Since the mass was attached in a globular form, snare catheter was placed slightly apart from the base for optimal constriction. At the Endo-cut mode (120 W, effect 3), partial resection was performed for less than 10 seconds to resect most of the mass. Typical yellow tissue indicating lipoma could be observed on the exposed surface (Fig. 2D). The colonoscopic finding at the next day confirmed flowing out of the remaining lipoma tissue at the exposed lesion (Fig. 2E). The patient was relieved of the abdominal discomfort afterwards. At 1-year follow-up colonoscopy, a surgical scar was observed but not any remaining lipoma (Fig. 2F).
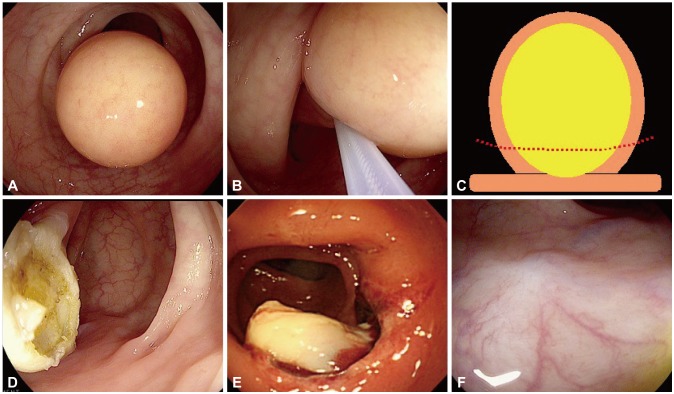
Endoscopic resection of a giant colon lipoma, case 2. (A) A 3×3-cm yellowish protruding mass without mucosal change detected at the sigmoid colon during colonoscopy. (B) Partial resection performed on the center of the lesion using snare. (C) A simplified illustration of the procedure. (D) Most of the mass is resected, and yellow tissue can be observed on the exposed surface of the remaining lesion, indicating typical lipoma. (E) Colonoscopy on the next day. The remaining lipoma tissues are flowing out of the exposed lesion. (F) One-year follow-up colonoscopy. There's no remaining evidence of the lipoma, except for the surgical scar.
Case 3
A 48-year-old male was referred to the center with diagnosis of a benign lesion in the ascending colon detected by abdominal-pelvic computed tomography and abdominal discomfort in the right lower quadrant. At colonoscopy, a 4×7-cm cylindrical protruding mass without mucosal change was detected originating from the proximal ascending colon (Fig. 3A). As the size of the mass was much bigger than the other cases, we first tried partial resection with a snare catheter at the apical end of the mass unlike the other cases. At the Endo-cut mode (120 W, effect 3), partial resection was performed for 20 seconds unsuccessfully due to the impeded conduction of the electric current by the submucosal lipoma tissue (Fig. 3B). It was found that the diameter of the mass became decreased toward the base of the cylindrical mass, which was why we retried partial resection slightly apart from the origin. Simulations were performed several times near the base of the mass, before performing the resection, in order to find the proper placement of the snare catheter with optimal constriction while avoiding possible thermal injury (Fig. 3C, D). Partial resection was performed for less than 5 seconds to reset most of the mass. Typical yellow tissue indicating lipoma could be observed on the exposed surface (Fig. 3E). As observed from the resected specimen of the mass, the apical end of the mass was too thick to apply electric current without inflicting severe thermal injury on the adjacent tissues, while the actual resected part was relatively thinner and the electric current was well-applied with rare thermal injury on the adjacent tissues (Fig. 3F). The patient was relieved of the abdominal discomfort afterwards. At 1-year follow-up colonoscopy, a surgical scar was observed but not any remaining lipoma.
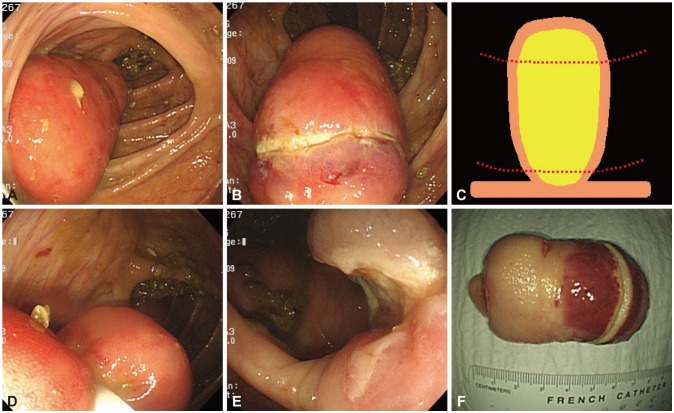
Endoscopic resection of a giant colon lipoma, case 3. (A) A 4×7-cm cylindrical protruding mass without mucosal change originating from the proximal ascending colon detected during colonoscopy. (B) Partial resection at the apical end of the mass resulted in serious thermal injury on the adjacent tissues without proper conduction of the electric current. (C) A simplified illustration of the procedure. (D) Since the diameter of the mass became decreased toward the base of the cylindrical mass, partial resection was retried slightly apart from the origin. (E) Yellow tissue can be observed on the exposed surface of the remaining lesion, indicating typical lipoma. Thermal injury of the adjacent tissues is not observed. (F) The resected specimen of the mass. The apical end of the mass was too thick to apply electric current without inflicting severe thermal injury on the adjacent tissues, while the actual resected part was relatively thinner and the electric current was well-applied with rare thermal injury on the adjacent tissues.
DISCUSSION
Generally, simple follow-up is sufficient for asymptomatic colon lipomas since they are highly unlikely to develop to malignancy.10 Excision becomes a necessity, however, when the size of the lipoma gets as big as to require histologic examinations for differential diagnosis from other malignancies and the patient accompanies symptoms such as abdominal pain, constipation, bleeding, or intestinal obstruction.4,10,11 Furthermore, ileocecal valve hypertrophy or lipomas occurring at the ileocecal valve, as presented in the case 1, is believed to cause small bowel obstruction.12
Recent development of endoscopic instruments and their accessories has enabled endoscopic excision of huge lipomas, but the complication rate is still higher than polypectomy.6 Pfeil et al.11 performed endoscopic removal of colon lipoma in seven patients and reported perforation in three of them. Adipose tissue contains not enough water to facilitate conduction of electric current, which is why endoscopists apply higher electrical output for snare during procedure, causing thermal injury on the colon wall adjacent to the mass and increasing the likelihood of perforation.6,13 It seems that, in case of a pedunculatd type with a long stalk, it is relatively safe to perform a procedure, as if performing polypectomy, bearing the low conduction in mind. However, in case of a wide-based lipoma, surgical resection is inevitable since forced endoscopic resection of such cases may not only cause acute complications such as bleeding or perforation, it may also lead to a severe stricture due to a large iatrogenic ulcer occurring after the resection.6
Two endoscopic methods to manage lipoma, complete resection and partial resection (including unroofing technique), have been reported.7-9 The unroofing technique, first reported by Mimura et al.,7 is a new method of endoscopic resection for colorectal lymphangioma, a benign tumor composed of several interconnected cavities. The unroofing technique only cuts off the upper half of the submucosal tumor, thus reducing the risk of complications. The difference of effectiveness between the two methods is not proven,9 but partial resection is thought to be much safer than complete resection due to lower chances of complication. However, in case of lipoma of big size (like case 3), remnant lipoma after cutting of the upper half could be possible. Therefore, in order to complete removal, more resection is more effective.
In this report, we performed endoscopic partial resection for wide-based giant lipomas to facilitate spontaneous flowing out of the remaining tissues with time. Practical methods to apply this strategy in three patients with distinct shapes of giant lipomas were described in detail. In the case 1, the patient had a wide-based lipoma. In order to expose the lesion by opening the cover, the partial resection of the central tissues was safely performed twice, and the remaining tissues were left to flow out spontaneously (unroofing technique). In the case 2, the lipoma was globular but wide-based, suggesting high risk of deep thermal injury on the adjacent tissues when resected in the form of polypectomy. Snare catheter was placed slightly apart from the base ensuring optimal constriction and the resection was performed for less than 10 seconds. The examination on the next day revealed the lipoma tissues flowing out of the exposed surface. In the case 3, we could personally witness the fact that snare resection of a giant lipoma could only lead to serious thermal injury on the adjacent tissues, suggesting high chance of complication after lipoma resection close to the base. We prefer and recommend using higher power cutting mode with shorter coagulation time, which can minimize cutting time and reduce heat-induced damage of adjacent tissues.
There are no reports demonstrating risk factor for complications of endoscopic lipoma resection. But, in cases of polypectomy, polyps larger than 1 cm in the right colon or larger than 2 cm in the left colon and multiple polyps carried an increased risk of bleeding and perforation.14 Therefore, we think that lipoma with a broad base or a large diameter has the risk for complication after endoscopic resection. Although surgery is not necessarily the first-line treatment option any more, the following circumstances are good candidates for operation; in case with wide-base sessile lipoma, unclear diagnosis, intussusception or obstruction, involvement of muscular and serosal layers.15
In conclusion, endoscopic resection could be preferentially recommended for giant lipomas, provided that the lipoma was well-characterized and the procedure was applied safely. The lesions could be cleared up spontaneously by unroofing technique and more aggressive resection will be needed in case of big size.
Notes
The authors have no financial conflicts of interest.