Intramural Gastric Abscess Caused by a Toothpick Presenting as a Subepithelial Tumor
Article information
Abstract
In the present report, we describe an unusual case of an intramural gastric abscess caused by a foreign body, detected in the form of a subepithelial tumor. A 64-year-old woman was referred to our gastroenterology clinic for further evaluation of a gastric subepithelial tumor. The patient presented with a 1-month history of sustained dull epigastric pain. Esophagogastroduodenoscopy revealed an ill-demarcated, round, smooth, protruding lesion with a small central erosion on the great curvature of the proximal antrum. Endoscopic ultrasonography indicated the presence of an ovoid, heterogeneous, hypoechoic lesion with small echogenic foci located in the submucosa and muscularis propria layers. An abdominal computed tomography scan showed focal gastric wall thickening and regional lymph node enlargement. Endoscopic submucosal dissection was performed for definite diagnosis and management. Thus, we detected a toothpick and removed it using grasping forceps. The final diagnosis was an intramural gastric abscess caused by a toothpick.
INTRODUCTION
Most ingested blunt foreign bodies that reach the stomach pass safely through the intestinal tract without any complications. However, long, hard, and pointed objects such as toothpicks may cause gastrointestinal bleeding, bowel perforation, obstruction, and sepsis.1 If foreign body ingestion is suspected and the patient presents with symptoms such as fever and severe abdominal pain with tenderness, physicians should consider the possibility of acute peritonitis combined with perforation. Furthermore, abdominal radiography or abdominal computed tomography (CT) should be performed prior to the endoscopic examination to evaluate the presence of complications. In the present report, we describe a case of an intramural gastric abscess caused by a foreign body detected in the form of a subepithelial tumor.
CASE REPORT
A 64-year-old woman was referred to our gastroenterology clinic for further evaluation of a gastric subepithelial tumor. The patient presented with a 1-month history of dull, continuous, and intermittent fulgurating epigastric pain with no specific aggravating or relieving factors. The patient was in good health, and her medical and drug histories were unremarkable. She had a blood pressure of 120/70 mm Hg, pulse rate of 76 beats per minute, and body temperature of 36.8℃. She did not have anemia or jaundice. Routine laboratory test results showed a white blood cell count of 4,600/µL and a platelet count of 253,000/µL. Her hemoglobin concentration and C-reactive protein level were 11.8 g/dL and 0.17 mg/dL, respectively. Serum amylase, lipase, and liver function test results were all within normal limits. The patient's abdomen was soft, with mild right-upper quadrant abdominal tenderness. No abnormal findings were detected on chest and abdominal radiography. Esophagogastroduodenoscopy (EGD) revealed an ill-demarcated, round, smooth, protruding lesion with a small central erosion on the great curvature of the proximal antrum (Fig. 1). The lesion was suspected to be a subepithelial tumor or extrinsic mass and was further evaluated by endoscopic ultrasonography (EUS) and abdominal CT. EUS indicated the presence of an ovoid, heterogeneous, hypoechoic mass with small echogenic foci located in the submucosa and muscularis propria layers, and a hyperechoic wall of the muscularis propria layer (Fig. 2). Abdominal CT showed focal gastric wall thickening with heterogeneous enhancement and regional lymph node enlargement (Fig. 3). The mass was assumed to be an inflammatory lesion caused by an eosinophilic abscess, a foreign body, or an infection. Therefore, endoscopic submucosal dissection (ESD) was performed for definite diagnosis and management. ESD revealed the presence of a toothpick that had penetrated the antral wall of the stomach (Fig. 4A). The toothpick (3 cm long) was removed using grasping forceps (Fig. 4B). The removal site was closed by metallic clips. EGD was performed on the following day to check for complications such as bleeding or perforation; however, no complications were detected. A pathological analysis of the resected specimen revealed chronic gastritis along with lymphocyte aggregation caused by chronic inflammation. The patient was discharged on the fourth hospital day after her symptoms had disappeared. In retrospect, the patient did not remember having eaten food containing a toothpick, nor had she experienced any problems with eating or swallowing.

Endoscopic findings. An ill-demarcated, round, smooth, protruding lesion with a small central erosion in the great curvature of the proximal antrum.

Endoscopic ultrasonography findings. An ovoid, heterogeneous, hypoechoic mass with small echogenic foci located in the submucosa and muscularis propria layers (arrow).

Abdominal computed tomography scan images. (A) Horizontal view image and (B) sagittal view image show focal gastric wall thickening with heterogeneous enhancement (arrow) and regional lymph node enlargement. Abdominal perforation or major vessel injury was not evident.
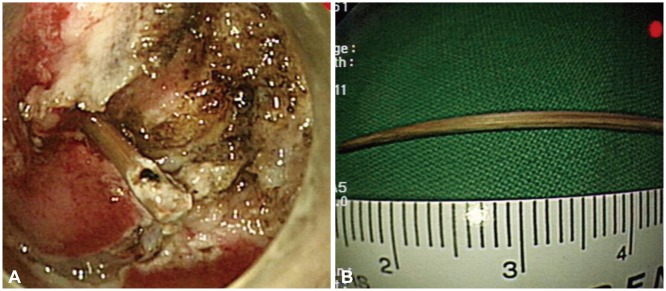
Endoscopic submucosal dissection findings. (A) A toothpick that penetrated the antral wall of the stomach. (B) The 3-cm long toothpick, after removal.
DISCUSSION
Of all the ingested foreign bodies that pass through the gastrointestinal tract, 80% to 90% cause no intraluminal injury.2 A foreign body that remains in the stomach can be asymptomatic, whereas an object remaining in the esophagus or small intestine may cause symptoms of dysphagia or intestinal colic.
The incidence of toothpick-related injuries to intestinal organs is estimated at 0.2/100,000.3 Toothpicks are more likely to cause intestinal perforations than other objects because they are long, slender, and sharp. Toothpick ingestion may lead to gastrointestinal hemorrhage, small or large bowel perforation, fistula formation, intestinal obstruction, sepsis, or other diseases.3 A patient complaining of abdominal symptoms should be assessed for complications such as obstruction and perforation by abdominal radiography or CT before an endoscopic examination is performed.
Unfortunately, as in the present case, many patients with foreign bodies in the gastrointestinal tract have no memory of their ingestion.4 Gastrointestinal injuries caused by foreign bodies can be asymptomatic, and may lead to potential complications in adjacent organs.5 For instance, appendiceal obstruction, asymptomatic gastric perforation, and constrictive pericarditis have been reported as complications of toothpick ingestion.1,5,6
In certain cases, foreign bodies that remain undetected may cause inflammatory, allergic, and infectious complications. Plain abdominal radiography is ineffective for detecting a radiolucent foreign body such as a toothpick. However, a CT scan can detect radiolucent foreign bodies, including ingested toothpicks, which are observed as hyperdense, long, and slender lesions. CT scanning is useful for acquiring clinical information, including the depth of penetration, the location of foreign bodies, and the presence of bleeding and inflammation in the abdomen.7,8,9 Rioux and Langis9 reported cases of gastrointestinal perforation by a toothpick that were detected by ultrasonography. EUS is a useful tool for differential diagnosis and can provide the information necessary for determining whether a mass originates from the wall or is caused by extrinsic compression.10
Gastric abscess associated with gastritis cystica profunda has been reported.11 In that case, EGD showed an edematous, protruding lesion with central ulceration on the antral wall. A yellowish purulent discharge was detected on the lesion. In our case, EGD revealed a round, protruding lesion with a small central erosion on the great curvature of the proximal antrum. We did not, however, detect any signs of gastric abscess. We performed CT, EUS, and ESD for the definite diagnosis and management of a suspected gastric subepithelial tumor and detected a toothpick that had penetrated the gastric wall. We then concluded that the lesion was an intramural gastric abscess caused by an ingested toothpick.
Our results suggest that foreign body ingestion should be considered during the evaluation of gastric subepithelial tumors in patients with recent onset abdominal pain. In patients who present with abdominal symptoms and who are suspected of having ingested a foreign body, CT and EUS are effective diagnostic tools.
Notes
The authors have no financial conflicts of interest.