A Needle Penetrating the Stomach Cavity after Acupuncture
Article information
Abstract
Although acupuncture is known as a safe procedure that is widely used in many countries, complications including infection, hemorrhage, hematoma, pneumothorax, nerve damage, and cardiac tamponade have been reported. A needle penetrating the stomach after acupuncture, however, is very rare. Here, we report the case of 47-year-old woman who experienced abdominal pain 2 days after receiving acupuncture. Upper gastrointestinal endoscopy identified an approximately 2.5-cm long needle in the posterior wall of the antrum. The needle was removed endoscopically using rat tooth forceps with no complications.
INTRODUCTION
Acupuncture is a form of alternative medicine that is practiced in many countries. It is used to treat a variety of conditions, from a simple cold to gastroenteritis, neuralgia, and musculoskeletal diseases. Acupuncture involves inserting several fine needles (usually 32 to 36 gauge) into selected sites on the body. Classic literature describe 365 points located in a systematic pattern along meridians or channels of energy flow, which are mapped onto the surface of the body.1 Although acupuncture is very safe, complications including infection or hemorrhage, hematoma, pneumothorax, nerve damage, and cardiac tamponade have been known to occur.2,3 To date, however, there have been no reports of acupuncture-associated needle penetration of the stomach cavity. Here, we report the case of a 47-year-old female patient who experienced abdominal pain 2 days after undergoing acupuncture. An endoscopic examination revealed an acupuncture needle penetrating the stomach cavity.
CASE REPORT
The patient was a 47-year-old woman who presented with a 2-day history of abdominal pain. She had no significant medical history, but had recently received acupuncture treatment at a local oriental medical clinic for abdominal discomfort. Her symptoms did not improve after the treatment; instead, she developed a throbbing pain in the mid-abdominal region. The following day, her abdominal pain worsened after she ate porridge, which did not improve with fluid therapy administered at her local hospital. Finally, she was referred to Asan Medical Center for further evaluation and management.
On arrival at the emergency department, her vital signs were stable: blood pressure, 138/79 mm Hg; heart rate, 76 beats per minute; respiratory rate, 18 breathes per minute; and body temperature, 36.1℃. She was alert, but appeared to have an acute condition. She had received acupuncture treatment at five mid-abdominal sites. Bowel sounds were normal, and there was no abdominal tenderness.
Laboratory results did not identify any significant abnormalities. Routine blood chemistry results were as follows: white blood cell count, 5,500/mm3; hemoglobin, 13.2 g/dL; hematocrit, 39.5%; and platelet count, 224,000/mm3. A coagulation battery showed a prothrombin time (international normalized ratio) of 1.04, and an activated partial thromboplastin time of 30.6 seconds. A chemical battery showed the following: Na+, 140 mmol/L; K+, 4.1 mmol/L; and Cl-, 101 mmol/L. The admission battery showed the following: blood urea nitrogen, 8 mg/dL; creatinine, 0.67 mg/dL; total protein, 7.7 g/dL; albumin, 4.4 g/dL; aspartate aminotransferase, 16 IU/L; alanine aminotransferase, 10 IU/L; total bilirubin, 0.7 mg/dL; and C-reactive protein, 0.13 mg/dL.
Chest radiography showed no significant findings; however, abdominal radiography showed a 25-mm-long radio-opaque linear image (Fig. 1). Abdominal computed tomography revealed a high-attenuated linear image (25 mm) embedded in the posterior wall of the antrum (Fig. 2).

Abdominal radiography findings. A radio-opaque, 25-mm-long needle is seen in the stomach (white arrowhead).

Abdominal computed tomography findings. A 25-mm-long acupuncture needle with high attenuation is seen embedded in the posterior wall of the gastric antrum (white arrowhead).
Esophagogastroduodenoscopy using a single-channel endoscope (GIF-H260; Olympus Optical Co., Ltd., Tokyo, Japan) was performed that revealed a needle penetrating the stomach. There was evidence of mucosal inflammation and edema surrounding the penetration site. In addition, mucosal erosion and inflammation were noted on the anterior wall of the antrum, which may have been caused by the penetrating needle (Fig. 3).

Endoscopic findings. A needle is embedded in the posterior wall of the antrum with edematous mucosal change around the needle (white arrowhead). Mucosal erosion and inflammation are seen on the opposite side of the needle (black arrowhead).
The needle was removed using rat tooth forceps (Olympus Co., Tokyo, Japan) and retrieved from the stomach using an endoscopic hood (MTW, Wesel, Germany) to prevent further mucosal injury. The needle was 25 mm long (Fig. 4). After treatment with antibiotics for 2 days (nil-by-mouth), the patient's abdominal pain subsided and there were no signs of infection (such as fever). She resumed a regular diet 2 days after the needle was removed and discharged without further medication.
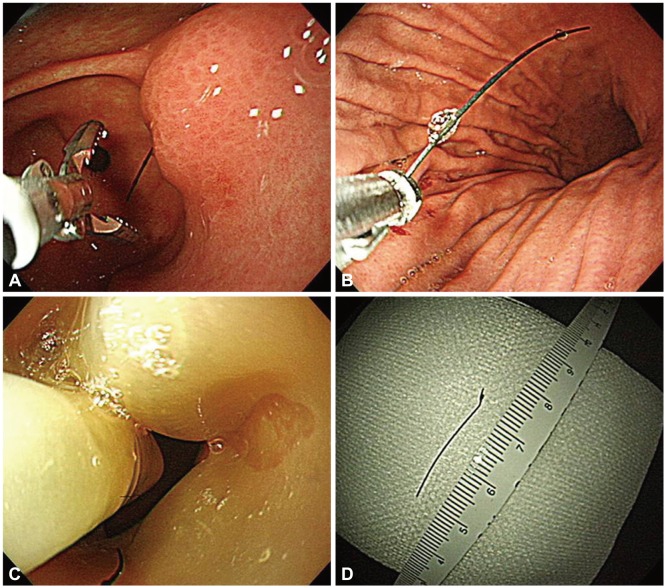
Endoscopic removal of the needle. (A, B) Rat tooth forceps were used to grasp and remove the needle. (C) An endoscopic hood was used to retract the needle for the prevention of other mucosal injury. (D) A 25-mm needle was removed without complications.
No specific findings were noted at the 3-month follow-up examination at the outpatient clinic. A follow-up esophagogastroduodenoscopy performed 3 months after the endoscopic removal showed complete resolution of the mucosal inflammation with no complications.
DISCUSSION
Acupuncture is an alternative therapy used to treat various diseases and is safe when performed by qualified practitioners.4,5 However, unsterile techniques (reusing needles or treating needles with bare hands) are associated with infections including hepatitis, human immunodeficiency virus, staphylococcal septicemia, osteomyelitis, and bacterial endocarditis. There have been reports, although rare, of life-threatening complications such as pneumothorax and cardiac tamponade.6 Here, we report a very unusual case in which the needle used for acupuncture was found inside the stomach. After endoscopic removal of the needle, the lesion healed completely with no complications.
Although acupuncture is associated with few complications, some have been reported. Indeed, two cases of thoracic empyema after acupuncture have been reported in Korea. In these cases, the metallic foreign bodies that were found in the lung were successfully treated by removal of the abscess and needle tip by thoracotomy.7 Another study reported a case of acute pancreatitis after acupuncture with a long needle that was managed conservatively.8 In another study, acupuncture treatment applied to the abdomen resulted in a hepatic injury with hemoperitoneum; in this case, the sequelae were fatal.9 The patient in the present study made a full recovery without any complications after the acupuncture needle, which penetrated the abdominal and gastric walls, was removed endoscopically.
Studies show that 10% to 20% of patients who ingest a foreign body will not require surgical intervention, whereas ≥1% will require surgery.10,11 In one study, the majority of patients with suspected foreign body ingestion (96.1%) were successfully treated using a flexible endoscope (with suitable devices attached) without any serious procedure-related complications.12 Various equipment are available for removing such foreign bodies, including polypectomy snares, foreign body forceps (rat tooth or alligator), roth retrieval nets, friction fit adapters (endoscopic mucosal resection, variceal band ligator), dormia baskets, and grasping forceps (Magill, Kelly).13 In this case, we used rat tooth forceps to remove the needle (which had penetrated the peritoneum and gastric wall) and an endoscopic hood to allow safe retraction.
Although acupuncture is a relatively safe procedure, this type of complication can be encountered in clinical practice; however, endoscopic removal using an appropriate device can remedy the problem without complications.
Notes
The authors have no financial conflicts of interest.