INTRODUCTION
Achalasia is an esophageal motility disorder caused by the inability of the lower esophageal sphincter (LES) to relax due to the degeneration of inhibitory neurons in the myenteric plexus.1 Achalasia has an incidence of 1 in 100,000 individuals annually and a prevalence of 10 in 100,000.2 Achalasia has no epidemiologic predilection for any demographic group, affects men and women equally, and can occur at any age.3 Symptoms are characterized by dysphagia to solid and liquids, regurgitation of food or saliva, substernal chest pain during meals, weight loss, aspiration pneumonia, and heartburn.4,5 Esophageal manometry reveals incomplete or absent relaxation of the LES and aperistalsis of the esophageal body.6
Treatments for achalasia primarily focus on dysphagia relief by decreasing the resting pressure in the LES. Treatments currently available include botulinum toxin (Botox) injections, oral pharmacologic therapies with nitrates and calcium channel blockers, pneumatic dilation (PD), and surgical myotomy.7,8 Only PD and surgical myotomy provide sustained response. Multiple studies have demonstrated the efficacy of PD exceeds 90% but usually requires serial dilations.7,9,10,11 The most severe complication of PD is esophageal perforation with a rate of ~2%.12 A review of 39 studies on laparoscopic myotomy found symptomatic improvement in a mean of 89% of patients. 7 A randomized controlled trial found that after 2 years of follow-up, laparoscopic Heller myotomy (LHM), as compared with pneumatic dilatation, was not associated with superior rates of therapeutic success.13
Peroral endoscopic myotomy (POEM), is an endoscopic procedure that achieves division of the esophageal circular muscle fibers across the esophagogastric junction (EGJ) and into the stomach. It is derived from natural orifice transluminal endoscopic surgery (NOTES) and advances in endoscopic submucosal dissection (ESD).14 Pasricha et al.15 initially described the feasibility of an endoscopic submucosal esophageal myotomy in a pig model in 2007 and the technique was subsequently developed and translated into clinical care by Inoue et al.16 in Japan. This paper will focus on the steps require to set up a POEM program in a modern endoscopy program as well as the training required to achieve skills and credentialing in this procedure.
PREPROCEDURE EVALUATION
The evaluation of any patient with suspected achalasia involves a thorough history with focus on frequency, severity, and timing of onset of symptoms.17 The Eckardt score has become the standard metric to assess symptomatic outcomes for achalasia and incorporates a scale for dysphagia, regurgitation, chest pain, and amount of weight loss with higher scores representing more severe disease.18 Physiological evaluation should be performed with esophageal manometry. The introduction of high resolution manometry has increased the sensitivity of detecting impaired EGJ relaxation and esophageal aperistalsis in classic achalasia and also allows for division into subtypes.2 The diagnosis of achalasia is supported by barium esophagram findings including dilation of the esophagus, a narrow EGJ with "bird-beak" appearance, aperistalsis, and poor emptying of barium.4 Esophagogastroduodenoscopy is a complementary test to rule out pseudoachalasia, mechanical obstruction from stricture or tumor, determine the degree of esophageal dilation, and evaluate for coexistent esophagitis.1
Botox and PD can cause tissue injury at the LES and resultant submucosal fibrosis, which to varying degrees obliterates the dissection plane, making POEM more challenging but still feasible.19 Sharata et al.20 found no statistically significant difference in the length of procedure, incidence of intraoperative or postoperative complications, or 6 months postoperative median Eckardt scores in patients undergoing POEM previously treated with Botox or PD. Contraindications to POEM include severe pulmonary disease, cirrhosis with portal hypertension, severe coagulopathy, prior interventions resulting in submucosal fibrosis including ablation therapy and endoscopic mucosal resection, and esophageal or chest irradiation.21,22
PREPARATION
Full liquid diet should be instituted for 2 days prior to the procedure and nothing by mouth for at least 8 hours. The procedure room is organized with the patient on a centrally located procedure table with the endoscopist working at the head of the bed (Fig. 1). The patient is positioned supine and the procedure is performed under general anesthesia with positive pressure ventilation. Broad spectrum antibiotics are administered intravenously and continued during the hospital stay.
EQUIPMENT/ACCESSORIES
A forward-viewing high definition gastroscope with a 2.8 mm working channel (GIF-H180; Olympus, Tokyo, Japan) is fitted with a 4 mm transparent distal cap attachment (Model No. D-201-11804; Olympus). Carbon dioxide (CO2) gas is used for insufflation during the procedure with a CO2 insufflator (UCR; Olympus). A triangle-tip knife (KD-640L; Olympus), hybrid knife T type (ERBE, Erbe Elektromedizin GmbH, T├╝bingen, Germany), or hook knife (KD-620LR; Olympus) is used to create an esophageal mucosal incision, dissect the submucosal layer, and divide the circular muscle bundles. Coagulating forceps (Coagrasper, FD-411QR; Olympus) are used to close larger vessels prior to dissection and for hemostasis. For electrocautery, an electrogenerator (ERBE) is used. Final closure of the mucosal entry site is accomplished with hemostatic clips (Resolution clip; Boston Scientific, Natick, MA, USA) or endoscopic suturing (Overstitch Endoscopic Suturing System; Apollo Endosurgery, Austin, TX, USA).
ENDOSCOPIC TECHNIQUE
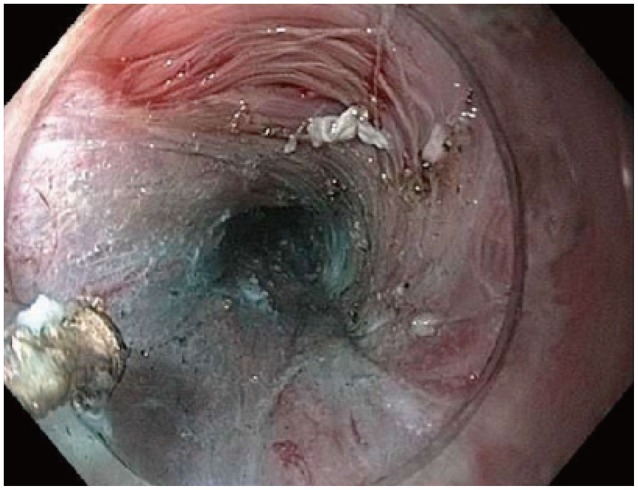
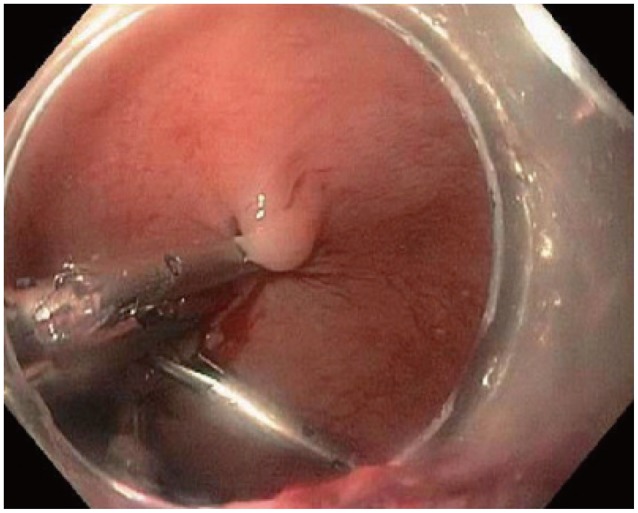
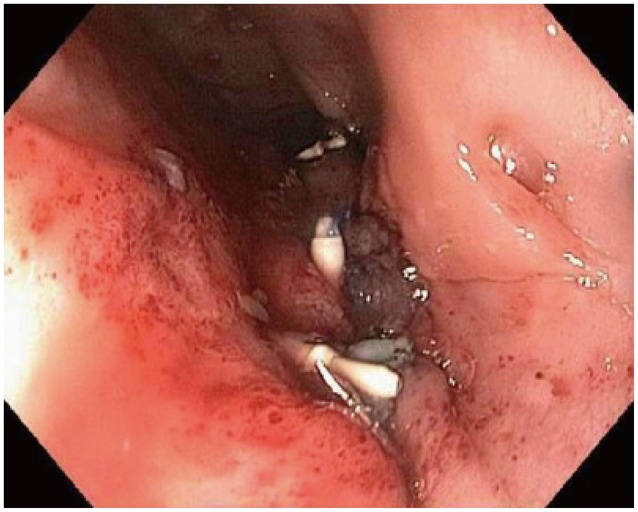
The esophagus is irrigated significantly until clean. Lavage of the esophageal mucosa is performed with gentamicin 80 mg in 20 cc normal saline. The initial mucosal incision is done along the right anterolateral esophagus at the 2 o'clock position, approximately 10 cm proximal to the EGJ. This maintains distance from high risk structures and leads to a straight tunnel ending at the lesser curvature at the cardia (Figs. 2, 3).23 A submucosal injection is performed using 0.9% NaCl and indigo carmine to create separation between mucosa and submucosa. An ESD knife (Endocut Q, Effect 3) is used to create a 2 cm longitudinal mucosal incision to allow entry to the submucosal space. The width of the submucosal tunnel should extend to half the circumference of the tubular esophagus. Larger vessels are coagulated with Coagrasper forceps in soft coagulation mode (Effect 5, 80 W). Dissection of the circular muscle fibers begins 3 cm distal to the mucosal entry site over a minimum length of 6 cm in the esophagus, and extending 2 cm into the cardia. Confirming extension of the submucosal tunnel beyond the LES into the cardia via a retroflexed view with visualization of blue discoloration of the cardiac mucosa from the blue dye used in the submucosal injection is important to prevent inadequate myotomy. Lavage of the submucosal tunnel with gentamicin 80 mg in 20 cc normal saline is recommended by Inoue et al.24 The mucosal entry site is then closed with hemostatic clips or endoscopic suturing (Figs. 4, 5). At the end of the procedure, the endoscope is inserted into the natural lumen down to the stomach to confirm smooth passage through the EGJ.
POSTOPERATIVE CARE
Following completion of the POEM procedure, all patients should be admitted to the hospital for observation. Routine labs and a barium esophagram should be performed on postoperative day 1. Patients should have nothing by mouth until the results of the esophagram are reviewed. If there is no evidence of contrast extravasation, patients can begin a clear liquid diet for 3 days. Broad spectrum antibiotics should be continued postoperatively for a total of 7 days, and can be transitioned from intravenous administration to oral route once patients are tolerating a liquid diet. Hospital discharge can be anticipated 48 hours postprocedure, with outpatient follow-up in 2 to 4 weeks. There are no consensus guidelines for postoperative follow-up after POEM. Repeat Eckardt scores, manometry, timed barium esophagram, endoscopy, and pH monitoring have all been used.17 An Eckardt score Ōēż3 is considered a clinical success.13,19,25 Despite treatment, patients with achalasia have up to a 50-fold increased risk of developing esophageal carcinoma compared with the general population, though presently no endoscopic surveillance guidelines exist.26
OUTCOMES
Even with the limitations of small numbers, early experience, and short term follow-up, POEM has a short term success rate of 90%, similar to initial treatment success of LHM.7,27 Verlaan et al.6 evaluated the effect of POEM on esophagogastric function by comparing Eckardt score, LES pressure, centimeters of barium stasis, EGJ distensibility and reflux esophagitis before and 3 months after POEM on 10 consecutive patients. They found that POEM had a statistically significant improvement in all outcome measurements of esophagogastric function except reflux esophagitis (6/10 endoscopically seen, only 3/10 reported reflux symptoms). Swanstrom and colleagues28 recently published their findings on long term outcomes for POEM. They followed 18 POEM patients for a mean follow-up of 11.4 months and found all 18 patients had dysphagia relief with postoperative manometry and timed barium swallows demonstrating significant improvements at 6 months. There was significant objective evidence of gastroesophageal reflux disease (GERD) postoperatively in 46% of patients. Stavropoulos et al.22 surveyed 16 expert centers with cumulative experience of 841 POEMs and found the prevalence of GERD in patients post-POEM to be 12%.
COMPLICATIONS
Since Inoue et al.16 described his experience on the first series of 17 patients with achalasia treated by POEM without any major complications, a number of investigators have begun to perform POEM and publish their preliminary experiences. The complications of POEM for which to monitor include delayed bleeding, pneumoperitoneum, pneumothorax, mucosal flap perforation, pneumomediastinum, cervical emphysema, and displacement of transparent cap. Bleeding usually occurs at the cut muscular edges because of an abundance of small blood vessels and collateral circulation in the muscle layers of the esophagus.29 Preventative coagulation of suspected bleeding areas by using hemostatic forceps significantly reduces the risk of delayed bleeding. Li and colleagues30 recently published a study reporting delayed bleeding in the submucosal tunnel after POEM in 3/428 patients (0.7%). All three cases of delayed bleeding were controlled by endoscopic hemostasis involving Sengstaken-Blakemore tube insertion and/or electrocoagulation without the need for surgical intervention or blood transfusions. Pneumoperitoneum and pneumothorax can occur due to gas permeation through the longitudinal muscle fibers of the esophagus or due to full-thickness dissection into the peritoneal cavity at the cardia.19 Pneumoperitoneum is usually asymptomatic and managed conservatively, although use of a Veress needle (Model No. ETH- UV120; Ethicon, Bridgewater, NJ, USA) to decompress capnoperitoneum has been described.19,23,27 Treatments of cardiac mucosal penetration vary from observation to closure by hemostatic clips. Li et al.31 described two cases of cardiac mucosal penetration treated with fibrin sealant when hemostatic clips failed to seal the defect. Saxena et al.32 reported the successful use of over-the-scope clips to close large esophageal mucosal flaps in two patients after inability to initially close the mucosal defect with standard clips. Ling and colleagues33 describe a 2 cm mucosal flap rupture at the lower esophagus. Due to the risk of restenosis, the rupture was sealed with a retrievable nickel-titanium stent instead of endoscopic clips. The stent was removed after 3 weeks when the rupture healed without any further complications. Closure of full thickness esophagotomy has been reported using an endoscopic suturing device in both muscular and mucosal layers after completion of endoscopic myotomy.34 Pneumomediastinum and cervical emphysema are caused by the insufflation of CO2 into the mediastinum during the submucosal tunnel dissection and the myotomy. The muscle fibers and adventitia are not a resistant barrier to CO2, which diffuses into the mediastinum and up to the neck.35 Pneumomediastinum and cervical emphysema are usually self-limiting and not clinically relevant. The range of pneumomediastinum and cervical emphysema in select published series ranged from 0% to 55.5%.16,19,25,36,37 CO2 insufflation has been stressed by the vast majority of studies to reduce complications. Baldaque-Silva et al.38 reported cap retention in the submucosal tunnel when the endoscope was withdrawn from the submucosal tunnel for mucosal surface assessment. The cap was retrieved with an alligator jaw forceps and afterwards the POEM was completed successfully. Despite the theoretical risk of infections, no cases of mediastinitis have been described perhaps due to the prophylactic administration of antibiotics before POEM. No mortality associated with POEM has been reported in published series.35
EXPANDED INDICATIONS
POEM has been performed for esophageal disorders aside from classic achalasia. Responses have been described for spastic achalasia, nutcracker esophagus, hypertensive LES, sigmoid esophagus, and diffuse esophageal spasm.3,16,20,27,39,40 The procedure has been performed in children as young as 3 years, though there is very limited data available.37,41,42,43 Rescue POEM has been described for failed surgical myotomy. Onimaru and colleagues44 successfully performed POEM primarily using a posterior myotomy axis in 10 patients with failed surgical myotomies (eight Heller, two thoracoscopic) who did not respond to PD with excellent short term results. Zhou et al.29 performed successful rescue POEM in 12 patients after a mean of 11.9 years from failed Heller myotomy. During a mean follow-up of 10.4 months, treatment success was achieved in 11/12 patients (91.7%).
POEM VS. LHM
There is scant data comparing POEM to LHM. Hungness and colleagues25 compared perioperative outcomes between POEM and LHM in a nonrandomized retrospective study. They found similar outcomes between both groups pertaining to myotomy lengths, complication rates, length of stay, and pain in postanesthesia care unit. The POEM group had shorter operation times and less estimated blood loss. Treatment success at median 6 months follow-up was 89% in POEM patients.
FUTURE DIRECTIONS
POEM is a technically challenging and time consuming procedure. Dissection of the submucosal fibers within the esophageal submucosal tunnel is a lengthy and time consuming task. Khashab et al.45 recently described the use of a new endoscopic gel composed of a proprietary material with tissue dissecting properties to help facilitate submucosal "auto-tunneling" in an animal experiment. The gel was injected into the submucosal layer and upon entry into the submucosal space, a submucosal tunnel had already formed and no esophageal submucosal dissection was required. Further tunneling into the gastric cardia was needed in all pigs with a triangle-tip knife. The average procedure time, including myotomy, was 28 minutes.
INTERNATIONAL EXPERIENCE
Over the past few years, the number of centers performing POEM has expanded. A recently published International POEM Survey (IPOEMS) reported data from 25 POEM operators at 16 expert centers with a combined volume of 841 POEM procedures. The mean POEM procedure time varied from 45 to 174 min. The mean myotomy length ranged from 6 to 15 cm. The centers surveyed perform 8 to 10 cm length myotomies with extension of the myotomy approximately 2 cm into the gastric cardia.22
POEM PROGRAM
Establishing a POEM program allows a tertiary center to build a comprehensive motility program and broaden the variety of treatments available for esophageal disorders. Initial clinical data has demonstrated the effectiveness and safety of endoscopic myotomy when performed by experienced operators. The increasing positive international experience has made the need for a training system in POEM more urgent. POEM requires skills including good endoscope manipulation, recognition of luminal structures, and knowledge of extraluminal structures, particularly vessels, nerves, and mediastinal anatomy.46 Starting a POEM program can be a difficult task with numerous institutional and administrative processes to clear in order to be successful. The prior establishment of a NOTES program allows for a much simpler segue into developing a POEM program. There are five essential prerequisites to start a POEM program: recruiting multidisciplinary collaborators, institutional support, credentialing board approval, proper training, and technical/engineering/nursing support.47
Before starting a POEM program, institutional support should be obtained for an animal laboratory, protected time to train, grant funding, purchase of equipment, and approval of credentialing and privileges. Procedures should only be performed in hospitals with available surgical expertise in managing potential complications. A standardized preprocedural checklist is advised to ensure all properly needed equipment is available. The procedure can be conducted in an endoscopic suite or operating room. Prior to beginning, the endoscopist should ensure all necessary equipment is available. Following the procedure, a standardized postprocedure protocol should be followed. Outcomes data should be prospectively recorded and maintained in a database to enable analysis.
At present, with few experienced POEM practitioners worldwide, there is no standardized training or credentialing guidelines. Initially, it is recommended that the endoscopist observe POEM performed by an experienced operator.48 Familiarization with all necessary equipment for the procedure is of utmost importance. The endoscopist should then practice the procedure rigorously. Training should encompass set up of equipment, followed by training using nonsurvival porcine models, then training using survival porcine models prior to undertaking the procedure in humans.46 Training on models helps free the cognitive capacity during procedures by allowing individuals to automate certain components of a procedure by removing the high stakes clinical environment.49 The porcine organ model is an easy, inexpensive and reproducible animal model for training. Due to a long esophagus and its close resemblance to a human esophagus, the porcine model allows for realistic exposure to the procedure. The disadvantages of the porcine model include thinner esophageal layers, different anatomy of the gastric cardia, and a softer and less vascular submucosal space which allows for easier submucosal dissection with less bleeding risk than in a human esophagus.48,49 Cadaver models can be used to confirm the results achieved in the animal laboratory prior to clinical implementation. The IPOEMS survey reported that 10 of 16 centers performing POEM received preclinical training before human cases.22 However, the centers had very different training, protocols, and training times, and some used ex vivo and others live animal models. The median number of proctored cases was 2. An experienced proctor should be present for the first initial human cases. Kurian and colleagues39 collected data from the first consecutive 40 POEM procedures on humans at their institution and determined the learning curve plateaus at about 20 cases for experienced endoscopists evidenced by decrease in length of procedure, variability in minutes per centimeter of myotomy, and incidence of inadvertent mucosotomies. With the growing number of centers performing POEM, many institutions have started offering this procedure after strict credentials have been set in place. At our institution, credentialing for POEM requires: 1) board certification in general thoracic surgery and upper endoscopic experience plus performing four POEM cases in a porcine model or 1 proctored human case, or 2) board certification in gastroenterology with endoscopic privileges in ESD and endoscopic retrograde cholangiopancreatography with sphincterotomy plus performing four POEM cases in a porcine model or 1 proctored human case.
The clinical team should also get exposure to the training in order to understand the technical aspects behind the procedure and ensure optimal results. Team members should be familiar with endoscopic equipment and instruments, which can reduce stress and mental workload during the procedure and potentially reduce complications and risks. Obtaining support from device or endoscopy representatives can be helpful in assisting with technical and engineering questions.
CONCLUSIONS
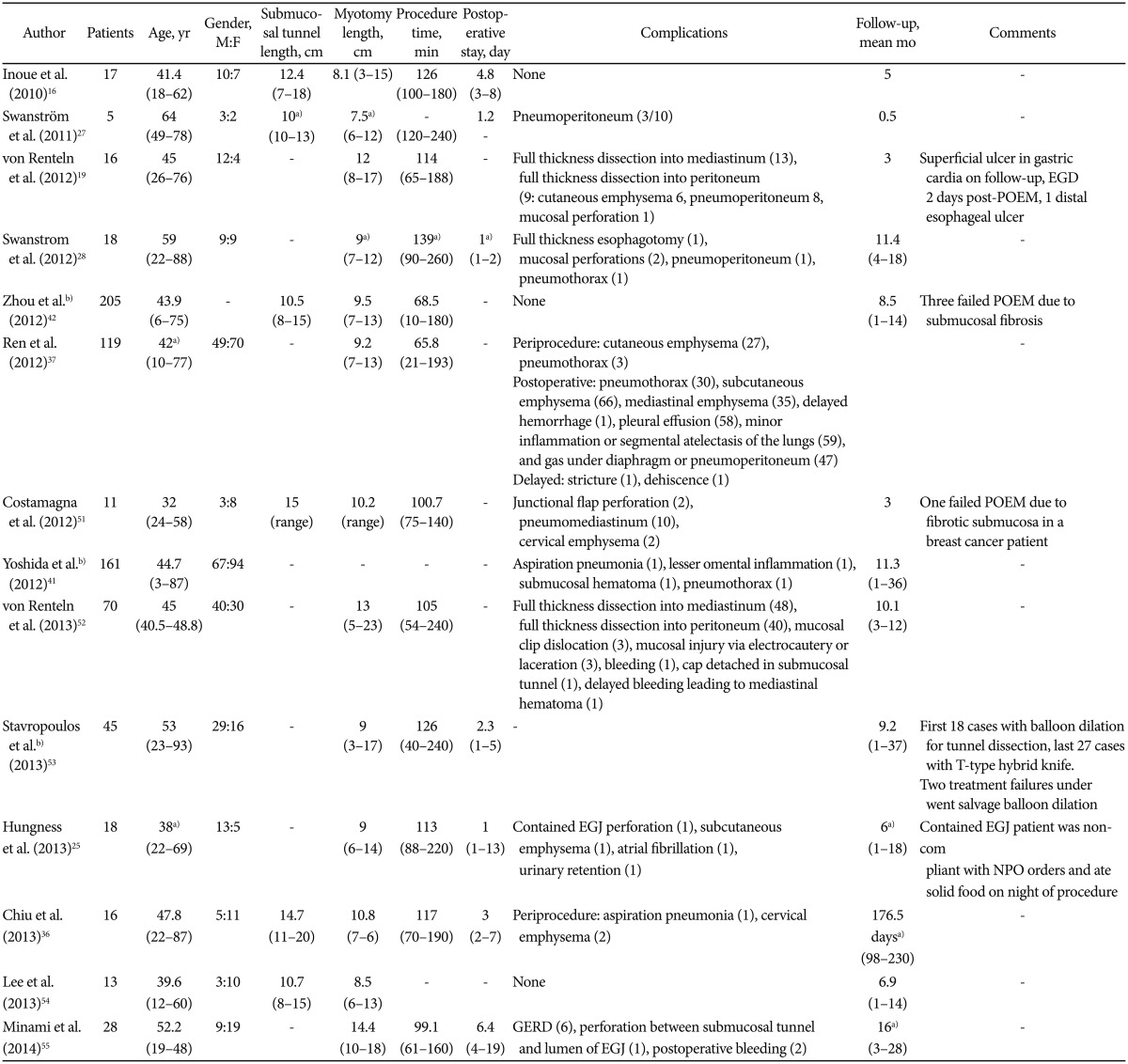
POEM is an exciting and novel technique in the realm of NOTES and ESD using submucosal tunneling to perform an endoscopic myotomy for achalasia and other esophageal disorders. The POEM procedure requires a certain degree of skill and competency, and should only be carried out by experienced endoscopists. Emerging technologies that objectively measure EGJ distensibility such as endoscopic functional luminal imaging probe (EndoFLIP) add parameters to determine efficacy of treatment for patients.50 The published literature to date has established the efficacy of the procedure and the few clinically significant complications have been usually treated conservatively. Table 1 presents data from select published case series of successful POEM procedures in humans so far.16,19,25,27,28,36,37,41,42,51,52,53,54,55 Further data is anticipated as more programs are established at tertiary care centers and long term follow-up is collected from pre-existing studies. Additional refinements in POEM technique are expected to yield a paradigm shift in the treatment of esophageal disorders in the coming years.