INTRODUCTION
Immunoglobulin G4 (IgG4)-associated cholangiopathy (IAC) is an inflammatory systemic disease characterized by IgG4-positive lymphoplasmocytic infiltration of the biliary tract.1,2,3,4 IAC is part of a systemic process in which IgG4 infiltration in the biliary tract is accompanied by infiltration in other organs, such as the pancreas (autoimmune pancreatitis [AIP]), salivary glands (chronic sclerosing sialadenitis), lacrimal glands (Mikulicz's disease), retroperitoneum (retroperitoneal fibrosis), kidneys, and many others.5
IAC is associated with pancreas involvement in approximately 90% of patients.6 However, biliary involvement may also be seen without pancreatic involvement.6 Although the most commonly involved part of the biliary tree in IAC is the intrapancreatic segment of the common bile duct, multifocal intrahepatic biliary strictures similar to those seen in primary sclerosing cholangitis (PSC) may occur.6,7 IAC can also present as a hilar pseudotumor or mass resembling cholangiocarcinoma (CCA).6,7 In a study conducted to determine whether cholangiography could be used to differentiate IAC from PSC and CCA, the sensitivity of diagnosing IAC based on cholangiography alone was found to be poor, and many patients with IAC were misdiagnosed with either PSC or CCA.8
The gold standard for diagnosing IAC is histology.6 However, biopsies of the bile duct do not usually provide sufficient amounts of tissue for a definitive diagnosis. Although IgG4 immunostaining may be suggestive of IAC, the specificity of this finding is low.6 In addition, elevated serum IgG4 levels are also found in other conditions such as PSC and CCA.9,10,11 Diagnosis of IAC in the absence of AIP is particularly difficult, and strategies such as ampullary biopsy, particularly in patients with ampullary swelling, and liver biopsy in patients with predominantly intrahepatic abnormalities have been suggested as additional diagnostic methods.12,13,14
Given the lack of a reliable marker for distinguishing IAC from PSC and CCA, strategies to improve the diagnosis of IAC are needed. A small pilot study suggested that IgG4 levels measured in bile may be useful in distinguishing IAC from PSC and CCA.15 In clinical practice, cholangiography is a required test for the evaluation of IAC. Bile aspiration during endoscopic retrograde cholangiopancreatography (ERCP) is not only easy and safe, but also associated with minimal additional costs. Because inflammation occurs in the biliary epithelium, IgG4 levels in the bile should theoretically be higher. We sought to use our prospectively established database of bile fluid in patients with biliary disorders to study the utility of measuring IgG4 levels in bile for differentiating IAC from PSC, CCA, and other benign biliary conditions in a small pilot study.
MATERIALS AND METHODS
Patients
The Cleveland Clinic biliary fluid database is a prospectively maintained database of bile obtained via direct aspiration from the common bile duct during ERCP in patients with biliary disorders. The database was established in 2012 and in addition to bile, contains demographic, clinical, cholangiographic, and follow-up information for all patients. Bile fluid from patients in the database was used for this study. The study was approved by the Cleveland Clinic Institutional Review Board and registered with the National Institutes of Health clinical trial registry (NCT01565460).
Inclusion and exclusion criteria
The inclusion criteria were the presence of a biliary condition and the ability to give informed consent. Exclusion criteria included age <18 years, unsuccessful cannulation of the bile duct, and abnormal postsurgical anatomy including biliary stricture in PSC patients after liver transplantation. The diagnosis of IAC was made through cholangiography, histology, IgG4 serum levels, and/or response to steroid therapy.
Biliary fluid sampling procedure
During ERCP, after cannulation of the common bile duct and prior to contrast injection, approximately 1 to 5 mL of bile was aspirated through the sphincterotome into a sterile syringe. Bile samples were immediately transported to the laboratory on ice and frozen at -80ā until use. The samples were thawed twice for IgG4 measurements.
IgG4 measurement in bile
Bile samples were centrifuged for 8 minutes at 150 g and 4ā. Measurements were performed in the hybridoma core of the Lerner Research Institute of the Cleveland Clinic by a single investigator (EP) who was blinded to the final diagnosis. Bile samples were identified by a numeric code, which was deciphered only at the end of the study when all measurements had been performed. The codes were prepared as two digit numbers which were designated by one of the investigators immediately after sample collection.
IgG4 in bile was measured by using a commercial enzyme-linked immunosorbent assay (ELISA) kit (eBioscience Human IgG4 Ready-Set-Go Kit, Cat. #: 88-50590; eBioscience, San Diego, CA, USA). Measurements of IgG4 in all bile samples were repeated twice, occurring at different times but within 2 months of one another and under the same conditions. Because there is no established normal range for IgG4 in bile, this experiment was designed to serve as a pilot study.
Statistical analysis
Descriptive statistics were computed for all factors. These include medians, 25th and 75th percentiles, range, or meanĀ±standard deviation (SD) for quantitative variables and frequencies as well as percentages for categorical factors. Continuous data are summarized as mean and SD and categorical data are summarized as frequency and group percentage. Normally distributed continuous variables were analyzed by using t-tests, and continuous variables that were not normally distributed were analyzed by using the nonparametric (Wilcoxon) rank sum test. IgG4 levels below the level of detection were included in the analysis and set to 0 mg/dL. Specifically, linear models of bile IgG4 were created with IAC, PSC, CCA, pancreatic cancer, and benign biliary conditions serving as independent variables. Diagnoses were assessed using pairwise comparisons. All analyses were performed using R 2.10.1 software (The R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
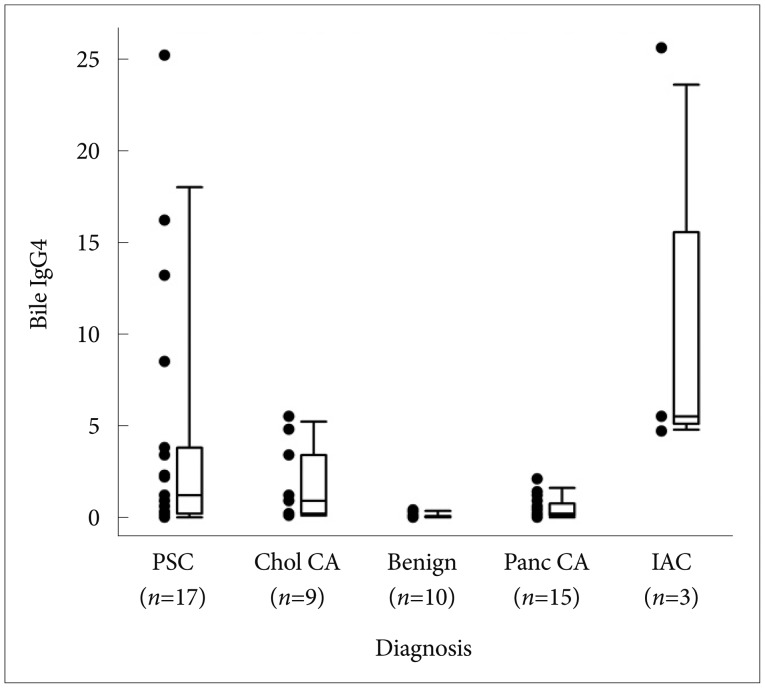
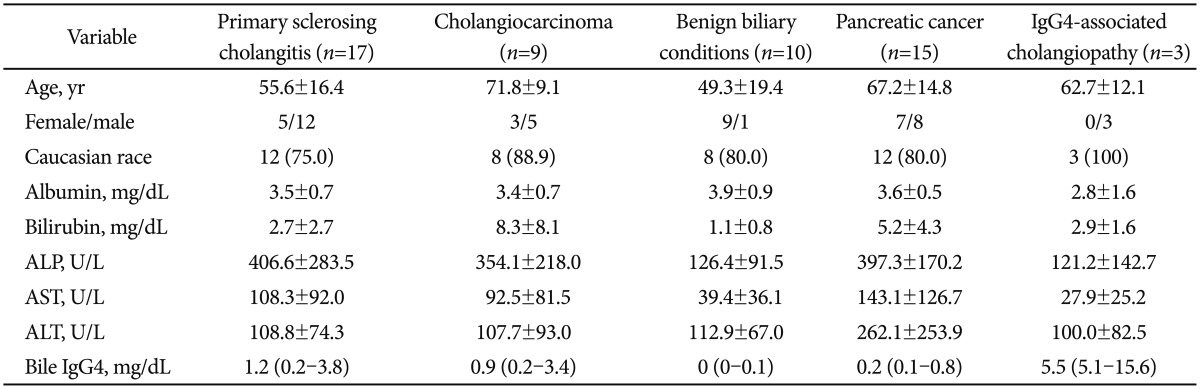
Bile fluid from 54 consecutive patients in the database (3 with IAC, 17 with PSC, 9 with CCA, 15 with pancreatic cancer, and 10 with benign biliary disorders such as sphincter of oddi dysfunction [n=4] and choledocholithiasis [n=6]) was used for this study. Table 1 highlights the characteristics of the entire study cohort with comparative laboratory features at the time of ERCP. IgG4 was detected in bile in all patients with IAC, CCA, and PSC; however, seven of nine patients with benign biliary disorders and two patients with pancreatic cancer had undetectable IgG4 levels in bile.
Biliary IgG4 levels in patients with IAC and benign biliary conditions
Biliary IgG4 levels were significantly higher in patients with IAC compared to those with benign biliary conditions (5.5; interquartile range [IQR], 5.1 to 15.6 vs. 0; IQR, 0 to 0.1; p=0.003). All three patients with IAC had evidence of associated pancreatic involvement. The first of these patients had a mid common bile duct stricture raising suspicion for possible CCA. However, further evaluation including IgG4 elevation in the serum to 553 mg/dL (normal <112 mg/dL) confirmed the diagnosis of IAC and the cholangiogram normalized with steroid treatment. The second patient had a mild elevation of serum IgG4 to 118 mg/dL and a pancreatic mass which was diagnosed as AIP based on pancreatic biopsy. This pancreatic mass resolved completely with steroid treatment. Subsequently, this patient developed multifocal biliary strictures resembling PSC. Further treatment with steroids resulted in complete normalization of the cholangiogram. The third patient had a distal bile duct stricture with elevation of serum IgG4 to 315 mg/dL. This patient also had a pancreatic mass which was diagnosed as AIP based on pancreatic biopsy on endoscopic ultrasound-guided fine needle aspiration. The pancreatic mass resolved completely with steroid treatment. All of these patients had ampullary biopsies, and only one had a positive result. Endoscopic ultrasound was performed in all three patients, two of whom had evidence of AIP from core biopsies of the pancreas, and 1 who did not have any pancreatic mass or features of AIP. Fig. 1 shows the median bile IgG4 levels in all patient groups.
Biliary IgG4 levels in patients with PSC
IgG4 levels in bile were elevated in patients with IAC as compared to patients with PSC (5.5; IQR, 5.1 to 15.6 vs. 1.2; IQR, 0.2 to 3.8) and this difference was statistically significant (p=0.001). Three PSC patients had higher biliary IgG4 levels than those seen in IAC patients. Two of these patients had a dominant stricture and both intrahepatic and extrahepatic biliary involvement at the time of ERCP and one also had concomitant inflammatory bowel disease (IBD). The other patient had evidence of severe intrahepatic PSC with no dominant strictures. Among the 17 patients with PSC, concomitant IBD was present in 14 patients. There was no difference in the IgG4 biliary levels in PSC patients with and without concomitant IBD. All patients with IBD had ulcerative colitis, while none had Crohn disease.
Biliary IgG4 levels in patients with CCA
IgG4 levels in bile were elevated in patients with IAC as compared to patients with CCA (5.5; IQR, 5.1 to 15.6 vs. 0.9; IQR, 0.2 to 3.4) and this difference was statistically significant (p=0.005). Two patients with CCA had higher biliary IgG4 levels than those seen in patients with IAC. Both of these patients had a tight hilar stricture at the time of bile aspiration, which was treated with metal stent placement. Both patients had normal serum IgG4 levels.
Biliary IgG4 levels in patients with pancreatic cancer
The median biliary IgG4 levels in patients with pancreatic cancer was significantly lower than those seen in patients with IAC (0.2; IQR, 0.1 to 0.8 vs. 5.5; IQR, 5.1 to 15.6; p=0.001). Table 2 shows pairwise comparisons resulting from a linear model with bile IgG4 as an outcome variable. A cutoff value of 3.8 mg/dL distinguished patients with IAC from those with PSC and CCA with a 100% and 76.5% sensitivity and specificity, respectively.
DISCUSSION
The sensitivity and specificity of cholangiography for diagnosing IAC is low and may lead to misdiagnosis as PSC or CCA.8 For example, in a study of 185 patients who underwent liver resections for presumed hilar CCA, 17% did not have any evidence of malignancy, and approximately 50% of these patients had histologic features consistent with IAC.16 In another study involving 53 patients with IAC, proximal extrahepatic biliary strictures mimicking CCA were seen in 34% and intrahepatic strictures similar to PSC were found in 36%.6
Elevated serum IgG4 levels have been suggested as a diagnostic tool for the detection of IAC. Elevations in serum IgG4 levels, however, have also been observed in patients with PSC and CCA.9,10,11 The sensitivity of serum IgG4 levels for diagnosing IAC has been reported to be approximately 74%.6 The specificity of the test is also suboptimal, as it has been associated with high false positive results. For example, elevated serum IgG4 has been reported in 9% to 20% of patients with PSC.9,10
The current pilot study was conducted to identify a new possible diagnostic marker for the diagnosis of IAC, as the diagnosis remains notoriously difficult, and differentiating IAC from PSC, CCA, and pancreatic cancer is clinically important. Analysis of bile collected during cholangiography could be a potentially useful marker for distinguishing IAC from other biliary disorders. Bile aspiration during ERCP is not only easy and safe, but also associated with a minimal increase in costs. We observed that patients with IAC had increased levels of IgG4 in bile compared to patients with pancreatic cancer, PSC, CCA, or those with benign biliary conditions. However, a small proportion of patients with PSC and CCA also had significant elevation of biliary IgG4, which therefore limited the specificity of biliary IgG4.
Our study results are similar to those of a previous study in which bile IgG4 levels were found to be significantly higher in patients with IAC as compared to those with PSC or CCA.15 However, it is important to understand that a small proportion of patients with PSC and CCA may have elevated IgG4 levels. The method of IgG4 measurement differed between the current study and the previously reported study.15 More specifically, we used an ELISA technique to measure IgG4 in bile, while the previously reported study used nephelometry, which is based on measuring the intensity of scattered light, to assess protein concentrations.
Prior studies have reported elevated serum levels of IgG4 in patients with CCA and PSC. In a study of 126 patients with CCA from the Mayo Clinic cohort, 13.5% were found to have elevated IgG4 (>140 mg/dL) and 3.2% had a >2-fold (>280 mg/dL) increase.9 Elevated IgG4 was found in 9% of patients with PSC in additional study.10 Therefore, it is not surprising that elevated biliary IgG4 was seen in a subgroup of patients with PSC and CCA in our cohort. It should be noted that the level of disease activity among patients with IAC may not be the same, and that patients with less active IAC may have IgG4 levels which could overlap with those of PSC and CCA patients. In addition, treatment with steroids may affect IgG4 levels in bile. As in the aforementioned, previously reported study,15 patients with IAC in our study were not on steroids or any immunosuppressive agents at the time of bile aspiration.
Our pilot study had one major limitation; only three patients in our cohort had IAC, which could have led to potential type II errors. However IAC is rare in North America, and we could accrue only three patients with IAC who did not have any previous treatment with prednisone or intervention/stenting in the bile duct over a period of 1 year at a tertiary referral center such as the Cleveland Clinic. Serum IgG4 levels were assessed in all our patients with IAC; however, we did not assess serum IgG4 levels in patients with CCA or PSC, or in patients with choledocholithiasis, as it is not part of the standard of clinical care. Therefore, we could not study the utility of serum IgG4 and its comparison to biliary IgG4 measurement in our cohort. Despite this limitation, we have identified a potential role for the assessment of IgG4 levels in bile as a diagnostic tool in patients with IAC. The results of this hypothesis-generating pilot study suggest a potential role for bile IgG4 measurements. We are planning to conduct a lager, multi-center study to recruit more patients in order to further elucidate the potential role of bile IgG4 level measurement in distinguishing IAC from various other biliary disorders.