INTRODUCTION
Duodenal ulcer is one of the most commonly encountered gastrointestinal diseases. The prevalence of duodenal ulcer is about 8% in Korea.1 Peptic ulcer disease is associated with the following two major factors: Helicobacter pylori infection and the consumption of nonsteroidal anti-inflammatory drugs. About 95% of duodenal ulcers occur in the duodenal bulb or within 5 cm of the pyloric ring. The remainder is formed between these areas and the ampulla. Ulcers around the ampulla are rare.2,3 The yearly incidence of acute pancreatitis in South Korea is about 20 new cases per 100,000.4 The most common causes of acute pancreatitis are excessive alcohol consumption and gallstones, which together account for nearly 80% of the cases.5,6 Other causes of pancreatitis include autoimmunity, trauma, anatomical abnormalities, and hereditary factors including genetic mutations.7,8,9 Metabolic disorders such as hypercalcemia and hypertriglyceridemia are also risk factors for acute pancreatitis.10 Although there are numerous causes of acute pancreatitis, an etiology cannot always be found. Acute pancreatitis caused by duodenal ulcer-induced ampullar damage is very rarely reported worldwide.11 A case of duodenal ulcer-induced pancreatitis is reported herein.
Case Report
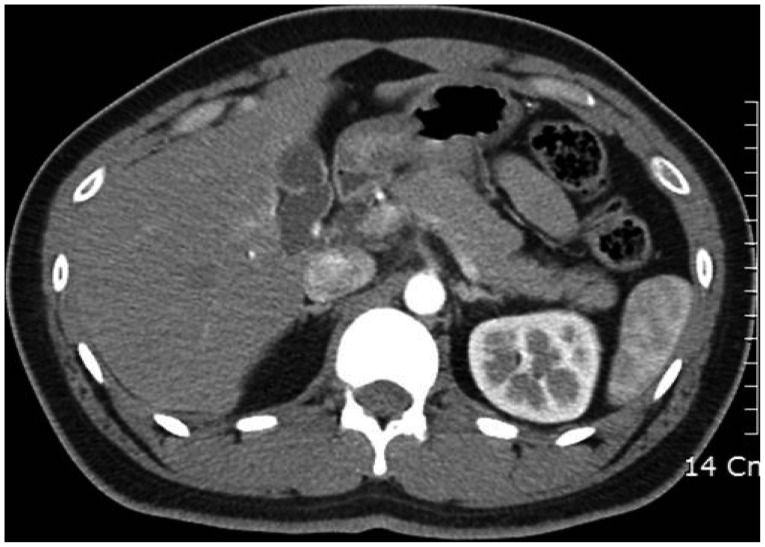
A 28-year-old man, with no notable clinical history, had been hospitalized for acute pancreatitis. His social history was insignificant except for light alcohol consumption (two cans of beer twice a week). On the next day, abdominal computed tomography (CT) showed mild pancreatitis with subtle peripancreatic fluid collection (Fig. 1). Initial laboratory findings were as follows: amylase, 345 U/L; lipase, 301 U/L; hemoglobin, 14.6 g/dL; white blood cells (WBC), 11,220/ТЕL; platelets, 222,000/ТЕL; C-reactive protein (CRP), 8.77 mg/L; aspartate transaminase (AST), 339 IU/L; alanine transaminase (ALT), 245 IU/L; alkaline phosphatase (ALP), 179 IU/L; blood urea nitrogen, 6 mg/dL; creatinine, 1.09 mg/dL; cholesterol, 120 mg/dL; prothrombin time/international normalized ratio, 13.1 seconds (1.27); gamma-glutamyl transferase, 315 IU/L; total bilirubin, 3.92 mg/dL; direct bilirubin, 2.75 mg/dL; hepatitis B surface antigen (-); anti-hepatitis C virus antibody (-); and anti-hepatitis A virus antibody immunoglobulin M (-). After 2 days of supportive care, he was discharged with alleviated abdominal pain and improved laboratory findings (hemoglobin, 12.4 g/dL; WBC, 7,240/ТЕL; platelets, 208,000/ТЕL; AST, 30 IU/L; ALT, 98 IU/L; ALP, 140 IU/L; amylase, 165 U/L; lipase, 203 U/L; total bilirubin, 0.67 mg/dL).
Three weeks later, he experienced a similar type of epigastric pain and radiating back pain. A close examination of his habits and lifestyle during this period revealed that there was no distinctive behavior excluding an occasional consumption of alcohol, which induced pancreatitis. Laboratory findings at the time of the revisit were as follows: total bilirubin, 0.64 mg/dL; gamma-glutamyl transferase, 149 IU/L; ALP, 97 IU/L; AST, 43 IU/L; ALT, 45 IU/L; blood urea nitrogen, 16 mg/dL; creatinine, 1.42 mg/dL; CRP, 0.26 mg/dL; hemoglobin, 15.8 g/dL; WBC, 6,830/ТЕL; platelets, 238,000/ТЕL; triglycerides, 81 mg/dL; low density lipoprotein, 128 mg/dL; amylase, 1,145 U/L; lipase, 1,103 U/L; immunoglobulin G, 1,096 mg/dL (range, 800 to 1,800); immunoglobulin A, 226 mg/dL (range, 126 to 517); anti-nuclear antibody, 1:160; rheumatoid factor, 2.5 IU/mL (0 to 10); complement C3, 135 mL/dL (range, 84 to 151), complement, C4 26 mg/dL (range, 17 to 40 mg/dL), venereal disease research laboratory test, 0; free thyroxine, 1.03 ng/dL; thyroid stimulating hormone, 0.708 ТЕlU/mL; cancer antigen 19-9, 13.42 U/mL.
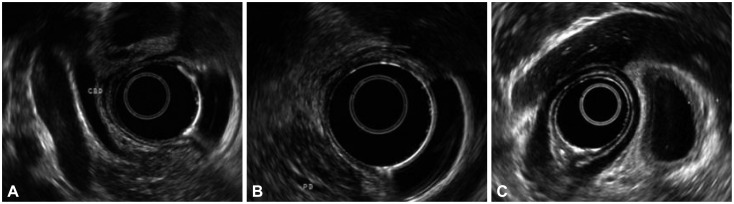
From the follow-up abdominal CT scan taken on the next day, mild diffuse enlargement of the pancreas and subtle peripancreatic strand-like infiltration were observed. Abdominal ultrasonography on the same day showed mild diffuse edematous enlargement of the pancreas, probably due to acute pancreatitis. Any stones or sludge within the gallbladder and bile duct were not observed. Diffuse gallbladder wall thickening, which could be considered secondary change, was noted. Endoscopic ultrasonography findings contained neither dilatation of the common bile duct and pancreatic duct nor pancreatic parenchymal masses (Fig. 2).
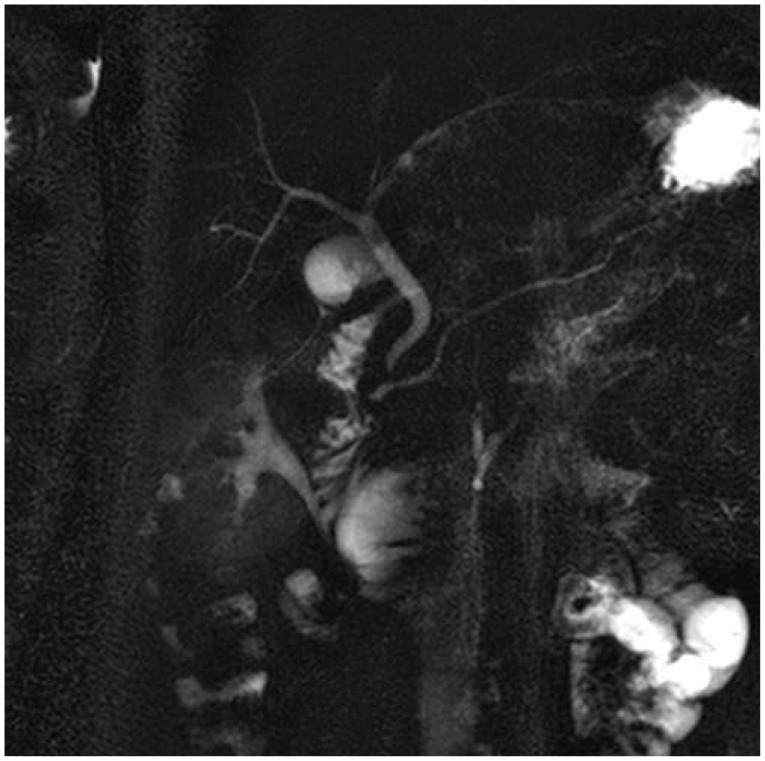
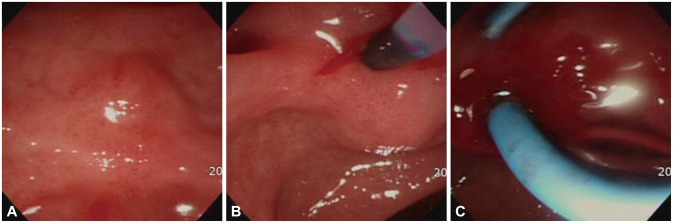
On the sixth day, a linear ulcer scar on the second part of the duodenum, which was accompanied by fibrotic changes around the lesion, was circumferentially observed by endoscopic retrograde cholangiopancreatoscopy (ERCP). However, any specific ampullar shapes were not detected even after scrutinizing the proximal and distal parts of the linear ulcer scar (Fig. 3). Close analysis of the ampulla conducted by another endoscopist also did not yield any meaningful results. On the 10th day, the patient's lab findings were as follows: amylase, 230 U/L; lipase, 71 U/L; hemoglobin, 14.5 g/dL; WBC, 4,950/ТЕL; platelets, 227,000/ТЕL; CRP, 1.08 mg/dL; AST, 20 IU/L; ALT, 14 IU/L; and total bilirubin, 0.6 mg/dL. Additionally, in magnetic resonance cholangiopancreatography (MRCP), no lesions such as anomalous pancreaticobiliary duct union (or anomalous union of the pancreaticobiliary duct [AUPBD]) were found. Only mild pancreatitis was observed (Fig. 4).
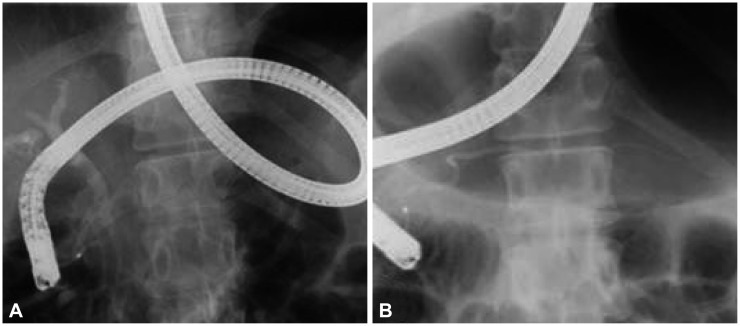
After the patient was transferred to a tertiary medical center, ERCP was repeated 7 days after the first ERCP. It was inferred that a pin-shaped ampulla was likely situated on the fibrotic band caused by the duodenal ulcer scar. Since it was difficult to distinguish the orifice of the ampulla by the naked eye, cannulation using an ERCP catheter tip was performed. Cannulation was successful only after several attempts (Fig. 5A, B). After an upstream injection of contrast media, the main pancreatic duct was observed, followed by the common bile duct, after delicate manipulation of the guide wire in several directions (Fig. 6). After stricture and distortion of the ampulla caused by the duodenal ulcer were diagnosed, dilatation with a 4-mm diameter endoscopic pancreatic balloon was conducted, followed by insertion of seven French plastic stents into the pancreatic duct (Fig. 5C). As there was considerable risk of cholangitis because of the narrow entrance of the distal common bile duct, endoscopic sphincterotomy was scheduled in case of fever and jaundice. Fortunately, the patient's status was stable after the procedure. After plastic stent insertion, H. pylori eradication was carried out in order to prevent duodenal ulcers in the patient who tested positive in the rapid urease test (also known as the CLOtest); proton pump inhibitor-based triple therapy comprising one proton pump inhibitor and two antibiotics, amoxicillin and clarithromycin, was used. Even though the follow-up period has not been very long, the patient has not shown any recurrence of symptoms since the removal of the plastic stent 1 month after insertion.
DISCUSSION
Through a series of initial evaluations such as history taking, physical exam, routine laboratory tests, and abdominal ultrasound or CT, 75% to 90% of the causes of acute pancreatitis can be found. The common causes are generally gallstones and alcohol intake. However, the remaining cases (10% to 25%), whose origins are unidentifiable, are referred to as idiopathic acute pancreatitis,6,12,13 and show a high recurrence and mortality rate. In this sense, it can be clinically very important to identify the causes.13,14,15 Potential etiologies of idiopathic acute pancreatitis could be microlithiasis, sphincter of Oddi dysfunction, hereditary pancreatitis, cystic fibrosis, a congenital abnormality such as pancreas divisum, choledochocele, annular pancreas, an anomalous pancreaticobiliary junction, and pancreaticobiliary tumors. In order to unveil the underlying causes, various means such as specialized laboratory tests, ERCP, endoscopic ultrasonography, and MRCP can be applied.16 The opening of the common bile duct is rarely located at the duodenal bulb due to a certain type of AUPBD.17 In our case, AUPBD could be excluded because both the main pancreatic duct and common bile duct were observed by ERCP during the injection of contrast media through the ampullar orifice, which was very difficult to find. AUPBD was not observed except for mild pancreatitis in the MRCP. In our case, the appearance of the duodenal ulcer as a form of a healing scar was combined with the ulcer scar surrounding the periampullar site. In addition, except for mild pancreatitis, pancreatic duct dilatation was not observed through ultrasonography and CT. For these reasons, the duodenal ulcer scar can be considered the main cause of pancreatitis in this case.
It is advisable to investigate the existence of duodenal ulcer through upper gastrointestinal endoscopy when it is difficult to find a distinctive cause of acute pancreatitis, considering the possibility of acute pancreatitis being accompanied by strictures and distortion of the ampulla following ulcer healing, like in this case.
When it is not easy to locate the orifice of the ampulla due to structural distortion, applying indigo carmine solution can be an alternative for tracing the drainage of bile juice, if the orifice is not completely blocked.
As in our case, the first-line treatment of such stricture-related cases can be a balloon dilatation, if an ERCP catheter is used to cannulate the upward biliary tract.18 Close follow-up for 1 to 2 months is recommended to check for any possible complications after inserting the plastic pancreatic catheter, and to monitor the recurrence of pancreatitis after removing it.