Is Submucosal Injection Helpful in Cold Snare Polypectomy for Small Colorectal Polyps?
Article information

Abstract
Background/Aims
Cold snare polypectomy (CSP) is an effective method of polyp removal for small colorectal polyps. However, the effect of submucosal injection in cold snare endoscopic mucosal resection (CS-EMR) for small polyps is unclear. Therefore, this study aimed to evaluate the effect of submucosal injection in CS-EMR for small polyps.
Methods
Between 2018 and 2019, 100 consecutive small colorectal polyps (5–10 mm) were identified in 58 patients. The first 50 consecutive polyps were removed by CS-EMR, and the remaining 50 were removed by CSP. Demographic data, clinical data, endoscopic findings, procedure times, complication rates, and pathology data were collected.
Results
No difference in the complete resection rate was observed between the CS-EMR and CSP groups. A total of 9 polyps showed post-polypectomy bleeding (7 had immediate bleeding, 1 had delayed bleeding, and 1 had both immediate and delayed bleeding). No difference in the bleeding rate was observed between the two groups. In multivariate analysis, warfarin (odds ratio [OR], 42.334; 95% confidence interval [CI], 1.006–1,781.758) and direct-acting oral anticoagulants (OR, 35.244; 95% CI, 3.853–322.397) showed a significantly increased risk of bleeding.
Conclusions
The effect of submucosal injection in CSP was not significant for small colorectal polyps.
INTRODUCTION
Cold snare polypectomy (CSP) is a safe and effective method to remove small colorectal polyps (5–9 mm) due to the lack of diathermy-related complications, including postpolypectomy syndrome, delayed bleeding, and perforation [1]. Several studies have reported that complete resection rate for CSP is significantly higher than that for cold forceps polypectomy in diminutive and small colorectal polyps [2,3]. A randomized controlled trial reported that complete resection rate for CSP was not lower than that for hot snare polypectomy (HSP) in 4–9 mm colorectal polyps [4]. Another meta-analysis showed that CSP had a shorter procedure time and tended to result in less delayed bleeding than HSP [5].
Recent studies have reported that cold snare polypectomy with submucosal injection (cold snare endoscopic mucosal resection [CS-EMR]) can be used to remove even larger polyps (≥10 mm) [6,7]. A prospective, randomized controlled study in China showed that CS-EMR was safe and effective for the treatment of 6–20 mm colorectal polyps [8]. Another study reported that the efficacy of CS-EMR was comparable to that of EMR for small colon polyps [9]. Polyp pre-lifting with submucosal chromoendoscopy—injection of a colored fluid—can sharply delineate lesion margins and help remove abnormal tissues using a cold snare [9].
However, data on the effect of submucosal injection in CS-EMR have been limited for small polyps by comparing CS-EMR and CSP. Therefore, this study aimed to compare the efficacy and safety of CS-EMR and CSP and to evaluate risk factors for immediate bleeding during the small polyp resection.
PATIENTS AND METHODS
Patients
Patients who underwent CSP or CS-EMR by a single endoscopist (SF) at Palo Alto Veterans Administration Hospital between September 2018 and April 2019 were included in this study. All patients consented to undergo the procedure, and data collection was performed with institutional review board approval (Stanford #15766). In accordance with guidelines, patients continued to take aspirin for cardiovascular problems throughout the perioperative period; clopidogrel and warfarin were discontinued for 5 days and resumed immediately after the procedure, whereas direct-acting oral anticoagulants (DOACs) (dabigatran, apixaban, rivaroxaban) were discontinued for 24–48 hr before the procedure and resumed immediately after [10]. During the first half of the study period, the routine practice of endoscopists was to perform submucosal injection with saline-containing indigo carmine for all cold snare polypectomies. In an attempt to decrease procedure time and reduce costs, an endoscopist changed the routine practice and stopped performing submucosal injection prior to cold snare polypectomy at the midpoint of the study period. Between September 2018 and April 2019, 100 consecutive small colorectal polyps (5–10 mm) were identified in 58 patients. The first 50 consecutive polyps were removed by CS-EMR (CS-EMR group), and the remaining 50 polyps were removed by CSP (CSP group). Demographic data, clinical data, endoscopic findings, procedure times were collected.
Endoscopic procedure
All patients underwent the standard bowel preparation before colonoscopy examination. Colonoscopies were performed under moderate sedation with intravenous midazolam and fentanyl. One expert endoscopist (SF) with an experience of >10,000 colonoscopies performed all procedures using a high-definition video colonoscope (Olympus PCF-H190AL or CF-H190AL; Olympus, Center Valley, PA, USA) with a high-definition processor (Evis Exera II CV-190; Olympus).
The polyp size was estimated through visual comparison with the size of the snare catheter or diameter (9 mm). Polyp morphology was described according to the Paris classification [11]. Pedunculated (Ip), semi-pedunculated (Isp), and sessile (Is) polyps were classified as the protruded type, and slightly elevated (IIa) polyps were classified as the flat elevated type.
Polyps from the cecum to the splenic flexure were classified as right colon polyps, and those from the descending colon to the rectum were classified as left colon polyps.
Bowel preparation was assessed using the Boston bowel preparation scale (BBPS) [12], and the value of the segment where the polyp was located was recorded.
Polyps were resected using an Exacto® cold snare (US endoscopy, Mentor, OH, USA). In the CS-EMR group, saline solution mixed with a few drops of indigo carmine for staining was used for submucosal injection.
After the polyp removal, the polypectomy site was rinsed with water and carefully inspected for residual polyps. If a residual polyp was observed at the polypectomy site, it was resected again using a cold snare. Complete resection was determined by carefully observing the polypectomy site. If the margin was not clearly observed, complete resection cannot be considered. Immediate bleeding was defined as intraprocedural bleeding requiring endoscopic hemostasis due to spurting or oozing for >2 min. Delayed bleeding was defined as postprocedural bleeding (within 14 days) that required hospital admission, repeat colonoscopy, or blood transfusion [13].
Statistical analysis
Continuous data are presented as means with standard deviations, and categorical data are presented as rates and proportions. Statistical differences were established according to the Pearson chi square test or Fisher’s exact test for qualitative variables and the Mann–Whitney U test for quantitative variables.
Associations among risk factors for bleeding were evaluated using logistic regression analysis in terms of odds ratio (OR) and its corresponding 95% confidence interval (95% CI). Factors with a p-value of <0.1 in univariate analyses were included in multivariate analyses. Results were considered significant if the two-sided p-value was <0.05, or if 95% CI did not include unity. All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) version 25.0 software (IBM Co., Armonk, NY, USA).
RESULTS
A total of 100 small colorectal polyps were identified in 58 patients. Table 1 shows the patient characteristics. The average age of patients was 67.5 years, predominantly comprised of men, as expected based on the majority-male demographics of the Veterans Administration Hospital. Nearly half of patients (46.6%) were taking antiplatelet agents, mostly aspirin. Two patients received dual antiplatelet therapy (aspirin and clopidogrel). Ten patients (17.2%) were taking anticoagulants: three with warfarin, six with DOACs, and one with low-molecular-weight heparin. One patient was taking both antiplatelets and anticoagulants (ticagrelor and apixaban). A total of 36 patients (62%) had one or more comorbidities, 20 (35%) had diabetes, 14 (24%) had coronary artery disease, 7 (12%) had atrial fibrillation, and 4 (7%) had chronic obstructive pulmonary disease.
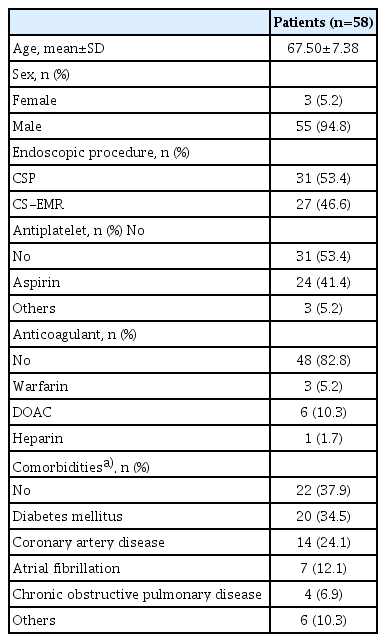
Clinical Characteristics of the Patients
Table 2 shows the characteristics of colon polyps along with the comparison of CSP and CS-EMR groups. The mean size of all polyps was 6.39 mm. A total of 60 polyps were classified as the protruded type (Is, Isp, and Ip), and 40 polyps were classified as the flat elevated type (IIa). Two patients had pedunculated polyps, all removed by CS-EMR. Fifty-four polyps were located in the right colon. In majority of patients, bowel preparation was good (segmental BBPS was 2 or 3). The complete resection rate was 92% and 96% in the CSP and CS-EMR groups, respectively, but without statistically significant difference. The total procedure time was significantly longer in the CS-EMR than that in the CSP group (78.76 sec vs. 23.14 sec, p<0.001). Resection and bleeding times were not significantly different between the two groups. According to the histological diagnosis, 79 polyps were adenomas, 9 were hyperplastic polyps, and 4 were serrated adenomas. The proportion of patients taking antiplatelet agents was higher in the CS-EMR group (54% vs. 30%, p=0.025). After polypectomy, 8 patients showed immediate bleeding and 2 showed delayed bleeding. One of them showed both immediate and delayed bleeding, and a total of 9patients had post-polypectomy bleeding (PPB). No differences in the PPB rate were observed between the CSP and CS-EMR groups. No patients had perforation.
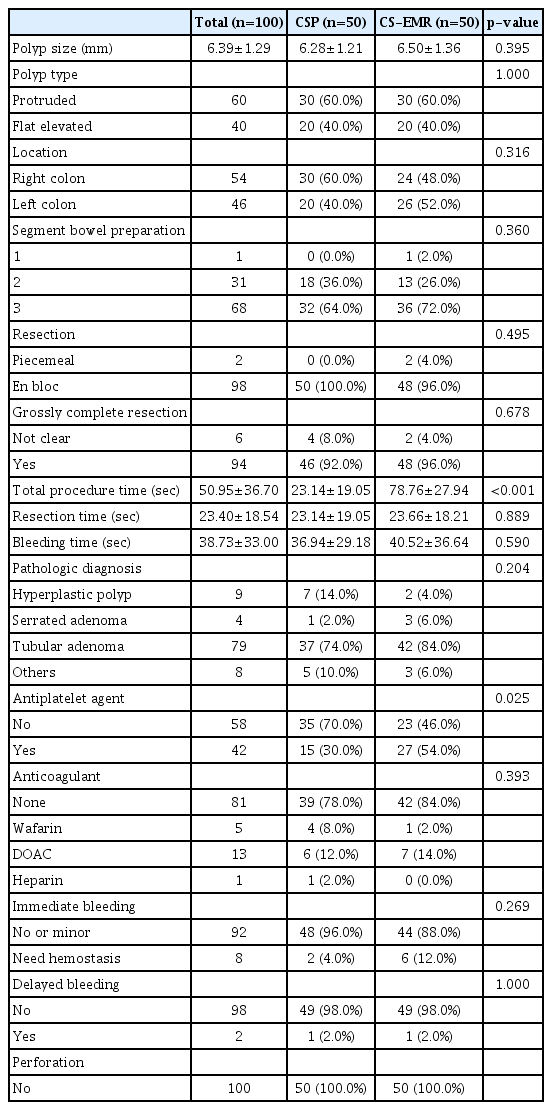
Comparison between Cold Snare Polypectomy and Cold Snare Endoscopic Mucosal Resection Group
Results of univariate analyses on risk factors for PPB are summarized in Table 3. DOAC (OR, 24.688; 95% CI, 4.106–148.432) and polyp size (OR, 1.740; 95% CI, 1.060–2.858) were associated with an increased risk of PPB.
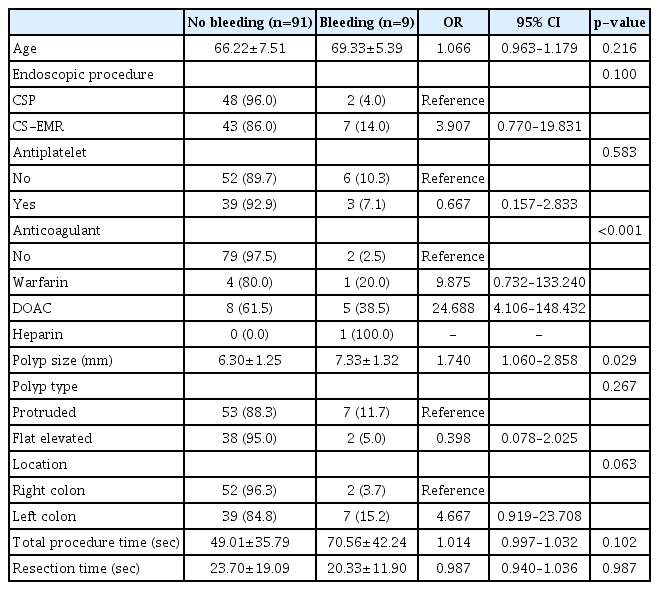
Univariate Analysis of Risk Factors for Postpolypectomy Bleeding (n=100)
In multivariate analysis (Table 4), warfarin (OR, 42.334; 95% CI, 1.006–1,781.758) and DOACs (OR=35.244; 95% CI, 3.853–322.397) showed a higher risk of PPB.

Multivariate Analysis of Risk Factors for Postpolypectomy Bleeding
DISCUSSION
Colonoscopic polypectomy can decrease the incidence of and mortality from colorectal cancer [14,15]. Conventional polypectomy uses an electrosurgical current that increases the risk of complications, including bleeding, perforation, and postpolypectomy syndrome [16,17]. Recently, the introduction of CSP, the mechanical resection of colorectal polyps without electrocautery, has attracted attention as a possible alternative [18]. In a recent prospective cohort study, CSP was performed on 1,198 small colorectal polyps, and no patients had delayed bleeding or perforation [19]. Another retrospective cohort study reported that the incidence of delayed PPB was significantly lower in the CSP than that in the HSP group [20]. According to a histological study comparing CSP and HSP specimens, HSP damaged the deep layers of the colon wall involving larger vessels, whereas CSP was limited to the shallow submucosa, which would be the reason for decreased incidence of delayed bleeding after CSP [21]. The European Society of Gastrointestinal Endoscopy (ESGE) clinical guidelines also recommend CSP as a resection technique for sessile or flat small colorectal polyps [22].
Submucosal injection before HSP provides a thermal safety cushion and makes defining the lesion margin easy [16]. Although injection for thermal safety is not required with CSP, submucosal injection may be helpful to resect polyps by sharply delineating the polyp margin and “loosening up” the submucosa [6]. Submucosal injection before CSP, also known as CS-EMR, has been reported in several studies. Recent studies reported that large colon polyps with an average size of 2 cm were successfully resected using CS-EMR without major adverse events [6,7,23]. The rate of residual or recurrent adenoma was reported as 0.6%–9.7% on follow-up colonoscopy within 1 year after CS-EMR, which is comparable to results of HSP [7,24]. However, most of these reports were studies on CS-EMR for large colorectal polyps measuring >1 cm. To the best of our knowledge, this is the first study to evaluate the effectiveness of submucosal injection in CSP for small polyps by comparing CSP and CS-EMR. In this study, no difference in the complete resection rate or the incidence of complications was observed between the CSP and CS-EMR groups, and the total procedure time was significantly increased with CS-EMR. These results suggest that submucosal injection is not helpful in CSP for small colorectal polyps.
In this study, the rate of immediate bleeding was 8% (8 cases), which is similar to that of previous studies [19]. Two patients (2.0%) had delayed bleeding; one of whom developed both immediate and delayed bleeding. He had been taking aspirin and warfarin for coronary artery disease and switched to heparin bridge therapy after the warfarin discontinuation because surgery was scheduled a week later. After the procedure, hemostasis was performed with clips for immediate bleeding. Delayed bleeding occurred at 3 days post-procedure. Colonoscopy showed an ulcer at the clip site with an adherent clot; therefore, additional clips were placed. Another patient with delayed bleeding was also safely treated with a hemoclip without transfusion. No patient had massive bleeding requiring surgery or transfusion, and all patients with bleeding were treatable with endoscopic procedures. No patients had colonic perforation.
This study analyzed the risk factors for PPB, including both immediate and delayed bleeding because only a small number (2) of patients developed delayed bleeding. Results showed that the risk of PPB increased with both warfarin (OR, 42.334; 95% CI, 1.006–1,781.758) and DOACs (OR, 35.244; 95% CI, 3.853–322.397). Warfarin is well known for increasing risk of procedure-related bleeding [25,26]. DOACs have been reported to be relatively safe compared to warfarin in terms of postpolypectomy bleeding [27,28]. Conversely, based on our results, a recent study reported that PPB risk was similar between patients taking warfarin and those taking DOACs [29]. Longer duration of anticoagulant use interruption prior to colonoscopy would possibly reduce bleeding risks associated with residual anticoagulant activity; however, this may expose patients to a higher risk of cardiovascular complications. Large-scale prospective studies will be needed to definitively answer remaining questions on the effects of DOACs on colonoscopy outcomes.
Polyp size was suspected to be a risk factor for PPB in univariate analysis (OR, 1.740; 95% CI, 1.060–2.858) but did not show statistically significant results in multivariate analysis. In previous studies, larger polyps (>1 cm) have been reported as risk factors for immediate and delayed PPB [30,31].
This study has several limitations. First because of the small number of study patients, the incidence of complications was insufficient to show a statistically significant difference. In addition, only two patients had delayed bleeding; therefore, risk factors for immediate and delayed bleeding could not be analyzed separately. If a study is conducted with a larger number of polyps in the future, whether submucosal injection will be clinically helpful in CSP for small colorectal polyps may be clarified.
Second, the evaluation of complete resection was confirmed only based on endoscopic gross findings. The muscularis mucosae (MM) is known to be only partially removed in cold snare polypectomy. If prior injection (CS-EMR) enables removal of the entire MM beneath the lesion and enables a negative vertical margin, the remnant/recurrence would be less frequent. If a histological examination was performed, more accurate results could be achieved. We washed the resection site after polypectomy with water and observed resection margins in detail. Only patients with clearly evident resection margin without remnant lesions were judged as complete resection, and the complete resection rate was 94%. A recent study reported a pathologic complete resection rate of 93.2% after CSP, which is similar to the results of our study [3].
Third, in patients taking antithrombotic agents, whether to discontinue or maintain the drugs was determined by evaluating the cardiovascular risk of each patient according to higher-risk endoscopic procedures. Patients who discontinued antithrombotics for several days before the procedure were also classified as taking antithrombotics. Therefore, the risk of bleeding from antithrombotic agents might have been evaluated as lower than the actual risk.
Patients were not randomized and those receiving submucosal injection had their procedures performed earlier than those who did not receive submucosal injection. Although no obvious statistical differences in the demographics were observed in the two groups and no other known technical changes in procedures occurred during the study period, we cannot exclude the effect of unknown biases.
Finally, the study was conducted at a Veteran’s hospital; therefore, majority of patients were men, and only 5% were women.
In conclusion, the effect of submucosal injection in cold snare polypectomy was not significant for small colorectal polyps. Anticoagulants such as warfarin and DOACs are risk factors for postpolypectomy bleeding, and patients taking these medications should be treated carefully to prevent postpolypectomy bleeding.
Notes
Conflicts of Interest: The authors have no potential conflicts of interest.
Funding
None.
Author Contributions
Conceptualization: Ji Hyun Song, Shai Friedland
Data curation: JHS, SF
Writing-original draft: JHS
Writing-review&editing: SF