Mohammad and Kahaleh: Comparing palliative treatment options for cholangiocarcinoma: photodynamic therapy vs. radiofrequency ablation
Abstract
Referral to an endoscopist is often done once curative resection is no longer an option for cholangiocarcinoma management. In such cases, palliation has become the main objective of the treatment. Photodynamic therapy and radiofrequency ablation can be performed to achieve palliation, with both procedures associated with improved stent patency and survival. Despite the greatly increased cost and association with photosensitivity, photodynamic therapy allows transmission to the entire biliary tree. In contrast, radiofrequency ablation is cheaper and faster to apply, but requires intraductal contact. This paper reviews both modalities and compares their efficacy and safety for bile duct cancer palliation.
Keywords: Ablation treatment; Bile duct neoplasms; Cholangiocarcinoma; Photodynamic therapy
INTRODUCTION
Cholangiocarcinoma is a rare cancer of the biliary tree. Cholangiocarcinoma may involve intrahepatic or extrahepatic bile ducts, excluding the ampulla of Vater or the gallbladder. Risk factors for the development of cholangiocarcinoma include biliary pathology, malformations, cholelithiasis, choledocholithiasis, cholecystitis, cholecystectomy, cirrhosis, alcoholic liver disease, hepatitis B or C infection, type II diabetes, chronic pancreatitis, and smoking, among others. 1 This disease carries a poor prognosis, with a median survival of less than 24 months. 2
Classification of tumor locations help in the determination of appropriate treatment modalities. The Bismuth-Corlette classification is used to define the longitudinal tumor extension of perihilar cholangiocarcinoma. 3 Extrahepatic cholangiocarcinoma can be classified by its location in the upper, middle, and lower third of the bile duct or simply by perihilar vs. distal cancer. 4 Conversely, lateral tumor extension is defined by using the TNM staging of the American Joint Committee on Cancer (AJCC) cancer staging system. Tumor resectability can be determined by the Blumgart T-staging system as well as the AJCC cancer staging system. 4 Bismuth type I tumors are defined as lesions located below the confluence of the right and left hepatic ducts, and can be treated through extrahepatic bile duct resection. In contrast, Bismuth type II tumors extend to the hepatic ducts and can be treated with bile duct resection, hepaticojejunostomy, and lymph node dissection. Bismuth type IIIa extends to the bifurcation of the right hepatic duct, while IIIb extends to the bifurcation of the left hepatic duct. General management for type III tumors involves hilar resection and hemihepatectomy with lymph node dissection. 3 Bismuth type IV tumors extend to the bifurcation of both right and left hepatic ducts, or are multicentric. Often, they are inoperable, with the exception of liver transplantation. 4
Surgery and/or hepatic transplantation is the curative treatment for cholangiocarcinoma. However, these modalities are rarely pursued in cases of advanced disease. In more widespread and unresectable cholangiocarcinoma, options range between a combination of biliary stenting, chemotherapy, immunotherapy, and other locoregional therapies. These include external beam radiation therapy (EBRT), radiofrequency ablation (RFA), trans-arterial chemoembolization, and photodynamic therapy (PDT). 5 This review focuses on the use of PDT and RFA in the palliation of cholangiocarcinoma.
PALLIATIVE TREATMENT OPTIONS
Biliary stenting
Biliary stenting is the most commonly used palliation technique for patients with nonresectable cholangiocarcinoma. This is performed to relieve jaundice and symptoms of biliary obstruction. The two types of biliary stents commonly used are plastic stents (PS) and self-expandable metal stents (SEMSs). Primarily, PS is used to serve as a temporary bridge to surgery in cases of hilar or extrahepatic resectable tumors, while SEMS is preferred in cases with nonresectable tumors such as malignant hilar obstruction. 6 In terms of clinical success, morbidity, and mortality, the short-term results of SEMS and PS are comparable. 6 However, results differ with respect to long-term outcomes. In a retrospective analysis of 480 patients with cholangiocarcinoma, SEMS was observed to have higher technical and clinical success rates and fewer complications compared to PS placement. 7 In the same study, the patency of bilateral SEMS and PS was significantly higher than that of unilateral SEMS or PS, with lower occlusion rates. Another randomized controlled trial comparing endoscopic retrograde cholangiopancreatography with SEMS vs. PS placement in patients with unresectable hilar cholangiocarcinoma reported that SEMS provided better drainage and longer survival compared to PS. 8 The decision to offer unilateral or bilateral stenting is often made after imaging with magnetic resonance imaging, allowing selective drainage when specific segments of the biliary tree are non-dilated or atrophic.
Radiofrequency ablation
RFA is a common palliative treatment modality for patients with unresectable cholangiocarcinoma. This has been utilized for tumor ablation in various types of gastrointestinal malignancies, including esophageal, rectal, and hepatic cancer. RFA works through the delivery of thermal energy within the tissue, leading to coagulative necrosis and cell death. 9 Cholangioscopy can be used to assess necrosis ( Fig. 1). For years, RFA procedures have been performed surgically and percutaneously. However, intrabiliary RFA through endoscopy has been observed to be safe and effective. The most commonly used devices for intrabiliary RFA are the Habib HPB-RF probe (Boston Scientific, Natick, MA, USA) and ELRA RF catheter (Taewoong, Medical USA, Los Angeles, CA, USA). 9
The use of RFA in cholangiocarcinoma improves stent patency by decreasing tumor ingrowth and benign epithelial hyperplasia. 10 The first study demonstrated its safety and efficacy, and reported improved stricture after RFA treatment with minimal complications. 10 Another early study of 20 patients with malignant biliary obstruction, 11 of which were due to cholangiocarcinoma, revealed the safety and efficacy of RFA in conjunction with stenting in improving biliary stricture. 11 In a later retrospective analysis examining the efficacy of RFA compared to stenting alone, RFA was shown to be an independent predictor of survival (hazard ratio, 0.29; p=0.012). 12
In recent years, randomized trials analyzing RFA treatment combined with stenting compared to stenting alone in cholangiocarcinoma have emerged. In a study of 65 patients with unresectable cholangiocarcinoma, the overall mean survival time was significantly better in patients who underwent RFA with stenting compared to those who underwent stenting alone (13.2% vs. 8.3%; p<0.001). 13
Photodynamic therapy
PDT achieves local tumor ablation through the accumulation of a photosensitizer in the region of interest and supplying light energy of a specific wavelength and intensity to activate the photosensitizer. 14 Photofrin (Pinnacle Biologics, Bannockburn, IL, USA) is the most frequently used photosensitizer due to its preferential uptake into malignant biliary tissue as opposed to normal tissue. Other photosensitizers such as Foscan (Biolitec Pharma Ltd, Jena, Germany), LS11, MACE, and 5-aminolevulinic acid (5-ALA), have also demonstrated uptake into biliary tissue. After uptake, the next step in PDT is the activation of the photosensitizer through delivery of light energy. This is performed through the use of fiber optics that pass through endoscopes to the target area. In the case of Photofrin, this is generally delivered intravenously at 2 mg/kg with illumination at 48 hours postinfusion at around 180ŌĆō200 J/cm via 630 nm red light. 14 Repeat PDT may be done at 3ŌĆō6 months if clinically indicated. Cholangioscopy can be utilized to center the fiber, which will administer red light to the cancerous lesion ( Fig. 2). The use of PDT in cholangiocarcinoma first emerged through the lens of a case report by McCaughan et al. 15 and has since become a fundamental technique in the management of unresectable cholangiocarcinoma. Similar to RFA, PDT is often used as an adjunct to stenting to allow tumor shrinkage with concurrent resolution of biliary obstruction. However, PDT is associated with photosensitivity. 14
In a randomized study comparing patients who received stenting with subsequent PDT to those who had stenting alone, there was increased survival in the stenting with PDT group as compared to the stenting only group (493 days vs. 98 days; p<0.001). 16 In an observational study of 48 patients over 5 years, there was increased survival in the PDT plus stenting group compared to the stenting only group (16.2 months vs. 7.4 months; p<0.004). 17 An earlier systematic review demonstrated the efficacy and safety of PDT for the treatment of cholangiocarcinoma with minimal complications. 18 In a more recent meta-analysis examining PDT with stenting vs. stenting alone for treatment and palliation in patients with cholangiocarcinoma, the survival period was significantly higher in PDT with stenting compared to stenting alone (413 days vs. 183 days; p=0.004). 19
Photodynamic therapy vs. radiofrequency ablation
A review of 54 studies consisting of 1,668 patients undergoing palliative treatment for cholangiocarcinoma with either PDT or RFA was conducted by the authors. The review included 37 studies on PDT consisting of 1,186 patients and 17 studies on RFA consisting of 482 patients. The overall survival rates and adverse events from the studies are detailed in Tables 116,17,20-48 and 2. 13,38,49-63
Results from a recent systematic review and meta-analysis on the use of RFA, PDT, and biliary stenting in the treatment of unresectable extrahepatic cholangiocarcinoma showed promising use of PDT over RFA or stenting. This review analyzed 55 studies consisting of 2,146 patients, 1,149 of which were treated with PDT, 545 treated with RFA, and 452 treated with stenting only. The study found that the pooled overall survival rate was 11.9 months (95% confidence interval [CI], 10.7ŌĆō13.1) with PDT, 8.1 months (95% CI, 6.4ŌĆō9.9) with RFA, and 6.7 months (95% CI, 4.9ŌĆō8.4) with stenting alone. 64 In addition, this meta-analysis demonstrated that the pooled survival rate of patients undergoing endoscopic and percutaneous RFA were 12 months (95% CI, 9.8ŌĆō14.3) and 5 months (95% CI, 3ŌĆō6.9), respectively. 64 The pooled 30-day mortality rate among patients undergoing PDT was 3.3% (95% CI, 1.6%ŌłÆ6.7%) compared to 7% (95% CI, 4.1%ŌłÆ11.7%) among those undergoing RFA. 64
Adverse events
The PDT and RFA studies cited cholangitis, sepsis, liver abscess pancreatitis, and phototoxicity as the most frequent adverse events. Cholangitis was the most common adverse event in both modalities, reported in 21% and 9.3% of patients who received PDT and RFA, respectively. Sepsis, liver abscess, and pancreatitis were also reported in both modalities. In addition, phototoxicity was reported in 5.6% of patients undergoing PDT. Many of these adverse events may not be intrinsic to the treatment modalities themselves, but may be related to the method of delivery.
CONCLUSIONS
Cholangiocarcinoma is a cancer of the biliary collecting system, with the majority of these tumors being nonresectable at the time of diagnosis. The main objective of palliative treatment for these patients is symptomatic relief through biliary decompression. Biliary stenting combined with ablation techniques such as PDT and RFA are the primary options for palliation.
PDT is a strong modality for palliation, with higher overall survival and lower 30-day mortality rates compared to RFA and/or stenting. The use of PDT requires expertise in the field and a dedicated team. Furthermore, additional effort is needed to prevent photosensitivity and other complications unique to this therapy. In patients who are unable to receive PDT, RFA has been increasingly used as an option for ablation and as an adjunct to biliary stenting.
PDT has some advantages over RFA in the palliative treatment of nonresectable cholangiocarcinoma. It operates through repeated interventions, which allows for additional tumor debulking with each session. Moreover, it is able to treat peripheral and unreachable lesions as it is transmitted through the biliary system and can also be used as downstaging therapy prior to surgery or transplantation. Numerous studies on PDT have demonstrated increased survival rates.
The advantages of RFA include repermeabilization of occluded metal stents and biliary stenoses. RFA also has lower cost and does not lead to photosensitivity, unlike PDT. However, RFA therapy requires the lesion to be reachable to be ablated, so it cannot be used for peripheral lesions. Recent studies suggest that RFA is less efficacious than PDT in terms of overall survival.
In conclusion, both PDT and RFA seem to have specific advantages and limitations, with PDT being potentially more beneficial. Further randomized controlled trials comparing PDT to RFA using an increased number of patients matched in terms of staging, age, and treatment need to be conducted to confirm this data.
Fig.┬Ā1.
Biliary cancer (A) pre- and (B) post-radiofrequency ablation treatment seen by cholangioscopy. 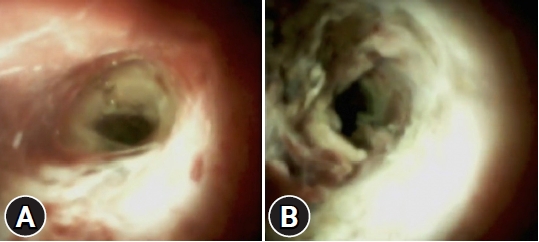
Fig.┬Ā2.
(A) Cancerous lesion assessed prior to photodynamic therapy. (B) Insertion of the fiber under cholangioscopic vision. (C) Administration of the right light under cholangioscopic control. 
Table┬Ā1.
Studies using PDT for treatment of cholangiocarcinoma
|
Study |
Study design |
No. of patients |
OS (mo) |
Adverse events |
|
Berr et al. (2000)20
|
Prospective |
23 |
9.1 |
Cholangitis (8), phototoxicity (3) |
|
Dumoulin et al. (2003)21
|
Prospective |
24 |
9.9 |
Cholangitis (2), phototoxicity (1), peritonitis (1) |
|
Ortner et al. (2003)16
|
RCTa)
|
39 |
16.43 |
Cholangitis (3), phototoxicity (2) |
|
Wiedmann et al. (2004)22
|
Prospective |
23 |
9.3 |
Cholangitis (13), phototoxicity (3) |
|
Shim et al. (2005)23
|
Prospective |
24 |
18.6 |
Phototoxicity (7), sepsis (1), abscess (1) |
|
Zoepf et al. (2005)24
|
RCTb)
|
32 |
21 |
Infection (4) |
|
Witzigmann et al. (2006)25
|
Prospective |
68 |
12 |
Cholangitis (38), phototoxicity (8) |
|
Prasad et al. (2007)26
|
Retrospective |
25 |
7.13 |
Pancreatitis (2), cholangitis (1) |
|
Kahaleh et al. (2008)17
|
Prospective |
19 |
16.2 |
Cholangitis (7), phototoxicity (3) |
|
Fuks et al. (2009)27
|
Prospective |
14 |
13.8 |
Cholangitis (8), phototoxicity (2) |
|
Quyn et al. (2009)28
|
Prospective |
23 |
14.16 |
Sepsis (5), phototoxicity (4) |
|
Gerhardt et al. (2010)29
|
Prospective |
8 |
12.3 |
Cholangitis (1), abscess (1) |
|
Hoblinger et al. (2011)30
|
Retrospective |
10 |
47.6 |
Cholangitis (2), phototoxicity (1) |
|
Cheon et al. (2012)31
|
Retrospective |
72 |
9.8 |
Phototoxicity (10), sepsis (1), abscess (1) |
|
Lee et al. (2012)32
|
Retrospective |
18 |
11.8 |
Cholangitis (1), phototoxicity (1) |
|
Pereira et al. (2012)33
|
Prospective |
36 |
12 |
Sepsis (5), phototoxicity (4) |
|
Bahng et al. (2013)34
|
Prospective |
11 |
4.68 |
- |
|
Talreja et al. (2013),35
|
Retrospectivec)
|
A: 25 |
8.57 |
Cholangitis (28), abscess (6), phototoxicity (3), other (7) |
|
B: 29 |
6.1 |
- |
|
Hong et al. (2014),36
|
Retrospectived)
|
A: 16 |
17.93 |
Cholangitis (1) |
|
B: 58 |
11.13 |
Cholangitis (3), phototoxicity (2), abscess (2) |
|
Park et al. (2014),37
|
RCTe)
|
A: 21 |
17 |
Phototoxicity (2), abscess (1) |
|
B: 22 |
8 |
Phototoxicity (2), abscess (2) |
|
Strand et al. (2014)38
|
Retrospective |
32 |
7.5 |
Cholangitis, abscess |
|
Hauge et al. (2016)39
|
RCTf)
|
10 |
7.9 |
Cholangitis (5) |
|
Wagner et al. (2015)40
|
Prospective |
29 |
15.4 |
Phototoxicity (5), cholangitis (4), abscess (2), cholecystitis (2) |
|
Lee et al. (2016),41
|
Retrospectiveg)
|
A: 24 |
11.6 |
- |
|
B: 13 |
9.5 |
- |
|
Wentrup et al. (2016),42
|
Retrospectiveh)
|
A: 33 |
17.33 |
Cholangitis (25) |
|
B: 35 |
12.47 |
Cholangitis (27) |
|
Yang et al. (2016)43
|
Prospective |
39 |
13.8 |
Cholangitis (1) |
|
Dolak et al. (2017)44
|
Prospective |
88 |
12.4 |
Cholangitis (21), sepsis (1), abscess (1) |
|
Pereira et al. (2018)45
|
RCTi)
|
92 |
6.2 |
Sepsis (2), cholangitis (1), pancreatitis (1) |
|
Gonzalez-Carmona et al. (2019),46
|
Retrospectivej)
|
A: 36 |
20 |
Cholangitis (20), abscess (5), phototoxicity (4), other (4) |
|
B: 34 |
15 |
Cholangitis (15), phototoxicity (3), other (2) |
|
Shiryaev et al. (2019)47
|
Case series |
33 |
14 |
Cholangitis (11) |
|
Wu et al. (2019)48
|
Retrospective |
59 |
17.6 |
- |
Table┬Ā2.
Studies using RFA for treatment of cholangiocarcinoma
|
Study |
No. of patients |
Study design |
OS (mo) |
Adverse events |
|
Mizandari et al. (2013)49
|
39 |
Retrospective |
2.98 |
- |
|
Butros et al. (2014)50
|
7 |
Retrospective |
38.5 |
- |
|
Dolak et al. (2014)51
|
58 |
Retrospective |
10.6 |
Cholangitis (5), hemobilia (3) sepsis (2), empyema (1) |
|
Strand et al. (2014)38
|
16 |
Retrospective |
9.6 |
- |
|
Tal et al. (2014)52
|
12 |
Retrospective |
6.4 |
Hemobilia (2) |
|
Laquiere et al. (2016)53
|
12 |
Case series |
12.3 |
Cholangitis (3), sepsis (1) |
|
Wang et al. (2016)54
|
12 |
Retrospective |
7.7 |
Infection (2), pancreatitis (1) |
|
Wang et al. (2016)55
|
18 |
Retrospective |
6.1 |
Cholangitis (3) |
|
Wang et al. (2016)56
|
9 |
Retrospective |
5.3 |
Cholangitis (4) |
|
Cui et al. (2017)57
|
50 |
Retrospective |
5 |
Cholangitis (10), pancreatitis (1) |
|
Wu et al. (2017)58
|
35 |
Retrospective |
6.97 |
Hemobilia (3), cholangitis (2) |
|
Xia et al. (2017)59
|
43 |
Retrospective |
2.68 |
- |
|
Acu et al. (2018)60
|
21 |
Retrospective |
2.53 |
Cholangitis (9), abscess (1) |
|
Yang et al. (2018)13
|
65 |
RCT |
13.2 |
Cholangitis (2) |
|
Bokemeyer et al. (2019)61
|
32 |
Case control |
11.4 |
Cholangitis (6), pancreatitis (2), other (1) |
|
Hu et al. (2019)62
|
23 |
Retrospective |
36 |
Pancreatitis (1) |
|
Lee et al. (2019)63
|
30 |
Prospective |
12.7 |
Pancreatitis (2), cholangitis (1) |
REFERENCES
1. Krasinskas AM. Cholangiocarcinoma. Surg Pathol Clin 2018;11:403ŌĆō429.   4. Chung YE, Kim MJ, Park YN, et al. Staging of extrahepatic cholangiocarcinoma. Eur Radiol 2008;18:2182ŌĆō2195. 6. Dumonceau JM, Tringali A, Blero D, et al. Biliary stenting: indications, choice of stents and results. European Society of Gastrointestinal Endoscopy (ESGE) clinical guideline. Endoscopy 2012;44:277ŌĆō298. 8. Sangchan A, Kongkasame W, Pugkhem A, et al. Efficacy of metal and plastic stents in unresectable complex hilar cholangiocarcinoma: a randomized controlled trial. Gastrointest Endosc 2012;76:93ŌĆō99. 9. Larghi A, Rimbas M, Tringali A, et al. Endoscopic radiofrequency biliary ablation treatment: a comprehensive review. Dig Endosc 2019;31:245ŌĆō255. 10. Steel A, Postgate A, Vlavianos P, et al. T1611: the use of a novel endoscopically placed radiofrequency probe for the management of malignant bile duct obstruction. Gastrointest Endosc 2010;71:PAB321. 12. Sharaiha RZ, Natov N, Glockenberg KS, et al. Comparison of metal stenting with radiofrequency ablation versus stenting alone for treating malignant biliary strictures: is there an added benefit? Dig Dis Sci 2014;59:3099ŌĆō3102. 13. Yang J, Wang J, Zhou H, et al. Efficacy and safety of endoscopic radiofrequency ablation for unresectable extrahepatic cholangiocarcinoma: a randomized trial. Endoscopy 2018;50:751ŌĆō760. 14. Allison RR, Zervos E, Sibata CH. Cholangiocarcinoma: an emerging indication for photodynamic therapy. Photodiagnosis Photodyn Ther 2009;6:84ŌĆō92. 15. McCaughan JS Jr, Mertens BF, Cho C, et al. Photodynamic therapy to treat tumors of the extrahepatic biliary ducts: a case report. Arch Surg 1991;126:111ŌĆō113. 16. Ortner ME, Caca K, Berr F, et al. Successful photodynamic therapy for nonresectable cholangiocarcinoma: a randomized prospective study. Gastroenterology 2003;125:1355ŌĆō1363. 17. Kahaleh M, Mishra R, Shami VM, et al. Unresectable cholangiocarcinoma: comparison of survival in biliary stenting alone versus stenting with photodynamic therapy. Clin Gastroenterol Hepatol 2008;6:290ŌĆō297. 18. Gao F, Bai Y, Ma SR, et al. Systematic review: photodynamic therapy for unresectable cholangiocarcinoma. J Hepatobiliary Pancreat Sci 2010;17:125ŌĆō131. 20. Berr F, Wiedmann M, Tannapfel A, et al. Photodynamic therapy for advanced bile duct cancer: evidence for improved palliation and extended survival. Hepatology 2000;31:291ŌĆō298. 21. Dumoulin FL, Gerhardt T, Fuchs S, et al. Phase II study of photodynamic therapy and metal stent as palliative treatment for nonresectable hilar cholangiocarcinoma. Gastrointest Endosc 2003;57:860ŌĆō867. 22. Wiedmann M, Berr F, Schiefke I, et al. Photodynamic therapy in patients with non-resectable hilar cholangiocarcinoma: 5-year follow-up of a prospective phase II study. Gastrointest Endosc 2004;60:68ŌĆō75. 23. Shim CS, Cheon YK, Cha SW, et al. Prospective study of the effectiveness of percutaneous transhepatic photodynamic therapy for advanced bile duct cancer and the role of intraductal ultrasonography in response assessment. Endoscopy 2005;37:425ŌĆō433. 24. Zoepf T, Jakobs R, Arnold JC, et al. Palliation of nonresectable bile duct cancer: improved survival after photodynamic therapy. Am J Gastroenterol 2005;100:2426ŌĆō2430. 26. Prasad GA, Wang KK, Baron TH, et al. Factors associated with increased survival after photodynamic therapy for cholangiocarcinoma. Clin Gastroenterol Hepatol 2007;5:743ŌĆō748. 27. Fuks D, Bartoli E, Delcenserie R, et al. Biliary drainage, photodynamic therapy and chemotherapy for unresectable cholangiocarcinoma with jaundice. J Gastroenterol Hepatol 2009;24:1745ŌĆō1752. 29. Gerhardt T, Rings D, Hoblinger A, et al. Combination of bilateral metal stenting and trans-stent photodynamic therapy for palliative treatment of hilar cholangiocarcinoma. Z Gastroenterol 2010;48:28ŌĆō32. 34. Bahng S, Yoo BC, Paik SW, et al. Photodynamic therapy for bile duct invasion of hepatocellular carcinoma. Photochem Photobiol Sci 2013;12:439ŌĆō445. 37. Park DH, Lee SS, Park SE, et al. Randomised phase II trial of photodynamic therapy plus oral fluoropyrimidine, S-1, versus photodynamic therapy alone for unresectable hilar cholangiocarcinoma. Eur J Cancer 2014;50:1259ŌĆō1268. 38. Strand DS, Cosgrove ND, Patrie JT, et al. ERCP-directed radiofrequency ablation and photodynamic therapy are associated with comparable survival in the treatment of unresectable cholangiocarcinoma. Gastrointest Endosc 2014;80:794ŌĆō804. 39. Hauge T, Hauge PW, Warloe T, et al. Randomised controlled trial of temoporfin photodynamic therapy plus chemotherapy in nonresectable biliary carcinoma: PCS Nordic study. Photodiagnosis Photodyn Ther 2016;13:330ŌĆō333. 40. Wagner A, Denzer UW, Neureiter D, et al. Temoporfin improves efficacy of photodynamic therapy in advanced biliary tract carcinoma: a multicenter prospective phase II study. Hepatology 2015;62:1456ŌĆō1465. 41. Lee TY, Cheon YK, Shim CS. Photodynamic therapy in patients with advanced hilar cholangiocarcinoma: percutaneous cholangioscopic versus peroral transpapillary approach. Photomed Laser Surg 2016;34:150ŌĆō156. 43. Yang J, Shen H, Jin H, et al. Treatment of unresectable extrahepatic cholangiocarcinoma using hematoporphyrin photodynamic therapy: a prospective study. Photodiagnosis Photodyn Ther 2016;16:110ŌĆō118. 45. Pereira SP, Jitlal M, Duggan M, et al. PHOTOSTENT-02: porfimer sodium photodynamic therapy plus stenting versus stenting alone in patients with locally advanced or metastatic biliary tract cancer. ESMO Open 2018;3:e000379.  46. Gonzalez-Carmona MA, Bolch M, Jansen C, et al. Combined photodynamic therapy with systemic chemotherapy for unresectable cholangiocarcinoma. Aliment Pharmacol Ther 2019;49:437ŌĆō447. 47. Shiryaev AA, Musaev GK, Levkin VV, et al. Combined treatment of nonresectable cholangiocarcinoma complicated by obstructive jaundice. Photodiagnosis Photodyn Ther 2019;26:218ŌĆō223. 48. Wu L, Merath K, Farooq A, et al. Photodynamic therapy may provide a benefit over systemic chemotherapy among non-surgically managed patients with extrahepatic cholangiocarcinoma. J Surg Oncol 2019 Nov 19 [Epub]. https://doi.org/10.1002/jso.25773. 49. Mizandari M, Pai M, Xi F, et al. Percutaneous intraductal radiofrequency ablation is a safe treatment for malignant biliary obstruction: feasibility and early results. Cardiovasc Intervent Radiol 2013;36:814ŌĆō819. 50. Butros SR, Shenoy-Bhangle A, Mueller PR, et al. Radiofrequency ablation of intrahepatic cholangiocarcinoma: feasability, local tumor control, and long-term outcome. Clin Imaging 2014;38:490ŌĆō494. 51. Dolak W, Schreiber F, Schwaighofer H, et al. Endoscopic radiofrequency ablation for malignant biliary obstruction: a nationwide retrospective study of 84 consecutive applications. Surg Endosc 2014;28:854ŌĆō860. 53. Laquiere A, Boustiere C, Leblanc S, et al. Safety and feasibility of endoscopic biliary radiofrequency ablation treatment of extrahepatic cholangiocarcinoma. Surg Endosc 2016;30:1242ŌĆō1248. 57. Cui W, Wang Y, Fan W, et al. Comparison of intraluminal radiofrequency ablation and stents vs. stents alone in the management of malignant biliary obstruction. Int J Hyperthermia 2017;33:853ŌĆō861. 58. Wu TT, Li WM, Li HC, et al. Percutaneous intraductal radiofrequency ablation for extrahepatic distal cholangiocarcinoma: a method for prolonging stent patency and achieving better functional status and quality of life. Cardiovasc Intervent Radiol 2017;40:260ŌĆō269. 60. Acu B, Kurtulus Ozturk E. Feasibility and safety of percutaneous transhepatic endobiliary radiofrequency ablation as an adjunct to biliary stenting in malignant biliary obstruction. Diagn Interv Imaging 2018;99:237ŌĆō245. 62. Hu B, Sun B, Gao DJ, et al. Initial experience of ERCP-guided radiofrequency ablation as the primary therapy for inoperable ampullary carcinomas. Dig Dis Sci 2020;65:1453ŌĆō1459. 63. Lee YN, Jeong S, Choi HJ, et al. The safety of newly developed automatic temperature-controlled endobiliary radiofrequency ablation system for malignant biliary strictures: a prospective multicenter study. J Gastroenterol Hepatol 2019;34:1454ŌĆō1459. 64. Mohan BP, Chandan S, Khan SR, et al. Photodynamic therapy (PDT), radiofrequency ablation (RFA) with biliary stents in palliative treatment of unresectable extrahepatic cholangiocarcinoma: a systematic review and meta-analysis. J Clin Gastroenterol 2022;56:e153ŌĆōe160.
|
|







