INTRODUCTION
According to the widely accepted concept of the adenoma-carcinoma sequence, adenomas account for >80% of colorectal cancer development.1 The removal of adenomas during colonoscopy has been associated with about a one-half reduction in colorectal cancer prevalence.2 Furthermore, >90% of colorectal polyps are <10 mm in size, and providing an accurate optical diagnosis for these small lesions is critical.3 However, due to the low diagnostic accuracy of white-light endoscopy (WLE) for optical diagnosis, many innovations in biomedical optics have been made to improve evaluation accuracy.4,5 Among these, a user-friendly, imaging-enhanced endoscopy was developed in 2006, known as narrow-band imaging (NBI). This virtual chromoendoscopy facilitates observation of the microvascular morphology and surface patterns of precancerous lesions.4,5 Recently, dual-focus (DF) mode has emerged as a powerful cutting-edge and tool that greatly enhances the visualization of microstructure patterns by combining digital and optical magnification.6 The utility of NBI and DF mode has been highlighted in several previous studies.5,7-12 In Vietnam, the clinical performance of the NBI system with DF mode for small colorectal polyps has not been sufficiently established due to a lack of data. The purpose of our investigation was to compare and assess the optical diagnostic accuracy of NBI with and without DF magnification in predicting small neoplastic lesions.
METHODS
Study design and eligible patients
This was a cross-sectional, single-center observational study at University Medical Center, Ho Chi Minh City, Vietnam, from September 2020 to May 2021. The inclusion criteria were as follows: (1) consecutive adult patients (age Ōēź18 years) who received elective colonoscopy (screening, surveillance, or diagnostic workup); (2) patients with small colorectal polyps (i.e., <10 mm in size); and (3) patients who underwent polyp retrieval for histologic examination. The exclusion criteria were as follows: (1) patients only presenting with colorectal polyps >10 mm in size or no colorectal polyps detected endoscopically and (2) poor bowel preparation.
Data collection
Demographic characteristics collected included gender and age. Each patient ingested 1.5 to 2 L of polyethylene glycol solution and 1,000 mg of simethicone for bowel preparation.
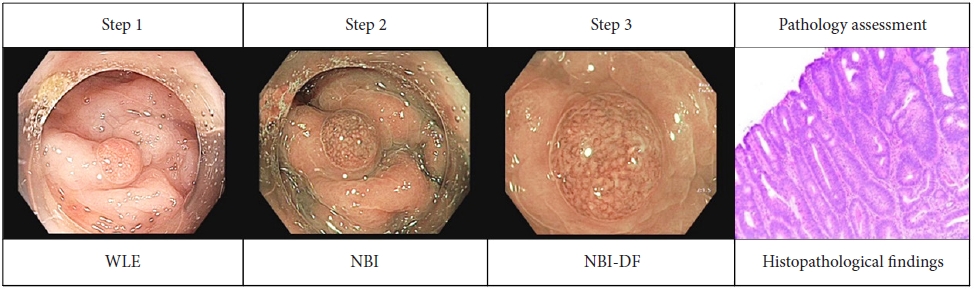
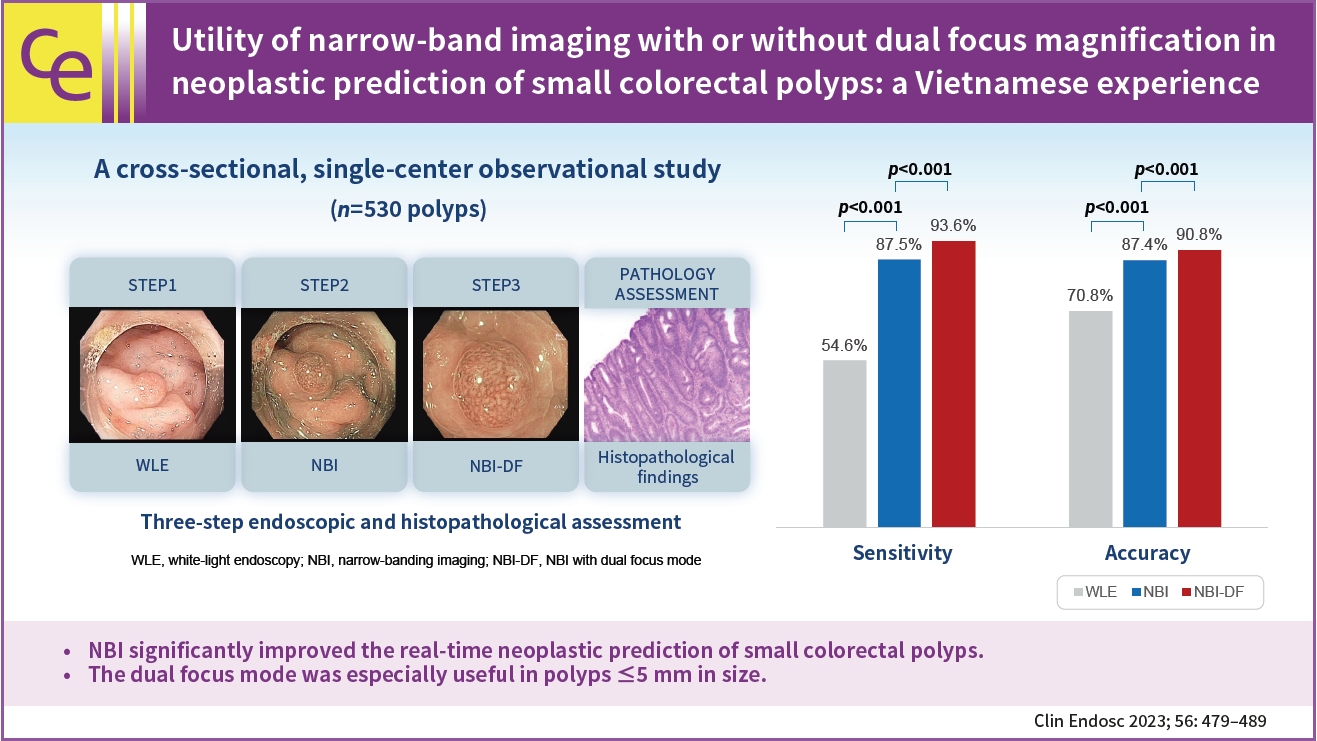
The two endoscopists who performed all colonoscopic procedures in this study (QDL and NQL) had previously experienced >1,000 colonoscopy procedures using NBI and NBI-DF. All polyps were assessed in three stages: first by WLE, then then NBI, and subsequently by NBI with DF (NBI-DF) (Fig. 1, Supplementary Video 1).
All examinations were performed using a 190 series Exera III NBI system (CF-HQ190L; Olympus Co., Ltd.) with DF mode. Both the NBI and DF functions were programmed as push-button techniques and were easily interchangeable with conventional white light and normal focus modes. NBI-DF mode was performed using a 1.4├Ś electronic zoom (approximately up to 63├Ś magnification) for all polyps. The electronic zoom enlarged the image without decreasing the image resolution. A transparent cap was utilized to ensure optimum focus.
After being washed intensively with simethicone solution, the size, location, and morphology of each polyp was documented. The lesion size was estimated by comparing the size of the polyp to that of the biopsy forceps (2.3 mm closed; Endo-Flex GmbH) and polypectomy snare (10 mm open, SnareMaster; Olympus Co., Ltd.). Lesions were assigned to one of the following colon segments. Polyp morphology was classified using the Paris classification system for superficial neoplastic lesions of the gastrointestinal tract.13
Classification of colorectal polyps
In WLE mode, we adapted the criteria of differentiation between non-neoplastic and neoplastic (adenoma) lesions based on their surface patterns: polyps were simply classified as either non-neoplastic (circular white pits, very fine capillary network bordering the pit) or neoplastic (circular/oval/linear/cerebri form pits, dendrite or gyrus-like pits or an irregular arrangement or loss decrease of pits), based on previous reports.10,14 In NBI and NBI-DF mode, endoscopists were asked to predict polyp types using the NBI international colorectal endoscopic (NICE) classification (Supplementary Table 1) and to rate their level of confidence (high or low).5 For example, the optical diagnosis would be considered ŌĆ£high confidenceŌĆØ when a polyp presented all three endoscopic features of color, surface, and vascular pattern, which were only associated with a specific type of NICE classification and with none of the others.9 An independent observer (TMH) recorded the diagnosis at each stage and ensured that the initial prediction would not change after the subsequent assessment stages.
Histopathological investigations
Each polyp was completely resected, and specimens were sent for pathological evaluation. However, if multiple rectal hyperplastic polyps <5 mm were found, the endoscopists were not required to remove them all, and only the first one was removed. Resected specimens stained with standard hematoxylin and eosin were assessed by an expert gastrointestinal pathologist (HML), who was blinded to all endoscopic images and assessments, and classified them according to the World Health Organization classification 2019.15
Statistical analysis
The data were investigated using IBM SPSS statistical software (ver. 23.0; IBM Corp.). The predicted histology and final polyp histology were used to determine the sensitivity, specificity, accuracy, positive predictive value (PPV), and negative predictive value (NPV) of WLE, WLE+NBI, and WLE+NBI+NBI-DF. Continuous variables were presented as means (┬▒standard deviation), while categorical ones were presented as proportions or percentages. Paired proportions were compared utilizing McNemarŌĆÖs test. Statistical significance was set at p<0.05 (two-sided).
Ethical statements
Ethical approval this study was provided by the Board of Ethics in Biomedical Research of the University of Medicine and Pharmacy at Ho Chi Minh City, Vietnam (number 150/DHYD-HDDD, signed on September 3, 2020). The study protocol conforms to the provisions of the Declaration of Helsinki in 1975. Before the examination, all patients provided their written informed consent.
RESULTS
PatientsŌĆÖ clinicopathological features
The clinical, endoscopic, and pathological characteristics of 343 patients and 530 lesions are shown in the flow chart (Fig. 2) and Table 1. Nine polyps were excluded from the analysis due to poor quality of the pathology specimens and the loss of patient data. Overall, the median polyp size was 3.6┬▒2.1 mm, and 76% of polyps were Ōēż5 mm. The most frequent lesion location was the rectosigmoid (45.3%). The 0-IIa type was the most frequently observed morphology. The most common histological findings were tubular adenoma (287/530 lesions, 54.2%). Of 530 polyps, 235 were non-neoplastic, including 105 hyperplastic polyps and other histologies such as inflammatory polyps and lymphoid follicles. The proportion of adenomas in polyps Ōēż5 mm and 6 to 9 mm in size were 50.1% (213/425 polyps) and 78.1% (82/105 polyps), respectively. Regarding advanced lesions, six polyps were tubular adenomas with high dysplasia. Since the investigation only included polyps <10 mm in size, the polyp detection rate and adenoma detection rate were not calculated.
Relationship between real-time optical diagnosis and pathological findings
1) Overall diagnostic efficacy of the three-stage assessment
The diagnostic value of the three steps is shown in Table 2 and Supplementary Table 2. Moreover, six advanced lesions were all predicted to have NICE 2 classification with high confidence in both WLE+NBI mode and WLE+NBI+NBI-DF mode. No polyps were predicted to have NICE 3 classification. Overall, NBI and NBI-DF mode assistance significantly improved the optical neoplastic diagnostic values. WLE was combined with NBI had a significantly improve sensitivity compared with WLE alone (54.6% vs. 87.5%, p<0.001) and NPV alone (61.5% vs 84.7%, p<0.001). Adding the NBI-DF mode significantly improved the diagnostic value, especially the sensitivity (93.6% vs. 87.5%), NPV (84.7% vs. 92.5%), and accuracy (87.4% vs. 90.8%, p<0.001). However, there were no significant differences between WLE+NBI and WLE+NBI+NBI-DF in terms of specificity (87.2% vs. 87.7%, p=0.250) or PPV (89.6% vs. 89.3%, p=0.250).
2) Impact of the polyp size on the accuracy of neoplastic predictions using dual focus magnification
The diagnostic yields for optical diagnosis and high-confidence rate across different polyp sizes are summarized in Table 3. The addition of the DF mode significantly increased the optical characterization yield and high confidence rate for lesions Ōēż5 mm (p<0.001). When the NBI and NBI+ NBI-DF modes were compared, the accuracy, sensitivity, specificity, PPV, and NPV in predicting neoplastic polyps were 87.3%, 84.1%, 90.6%, 90.0%, and 85.0% for the NBI mode, and 90.1%, 91.1%, 89.2%, 89.4%, and 90.9% for the NBI-DF mode, respectively. In addition, the high-confidence rate rose significantly, from 84.2% to 93.4%. However, the differences between NBI and NBI+NBI-DF were not significant in the 6 to 9 mm group.
3) Optical diagnosis misclassification in WLE+NBI and WLE+NBI+NBI-DF modes
NICE 1 classification misclassified 37 polyps as adenomatous (6.9%) in WLE+NBI mode and 19 (3.5%) in WLE+NBI+NBI-DF mode. NICE 2 classification misclassified 30 polyps (5.6%) in WLE+NBI and 33 polyps (6.2%) in WLE+NBI+NBI-DF.
DISCUSSION
To the best of our knowledge, this is the first study to evaluate the real-time optical diagnostic performance when implementing NBI and NBI-DF for small colorectal neoplastic polyps in Vietnam. The two main findings of our research were as follows: first, neoplastic optical diagnosis improved considerably with the assistance of NBI and NBI-DF in our Vietnamese setting. Second, in lesions Ōēż5 mm in size, NBI-DF significantly improved diagnostic performance.
In our study, the diagnostic values for WLE+NBI were significantly higher than those for WLE only, with improved sensitivity (87.5% vs 54.6%, p<0.001) and accuracy (87.4% vs 70.8%, p<0.001). A large meta-analysis of 56 studies also revealed good diagnostic performance for NBI in neoplastic prediction, with a sensitivity of 91.0% and an NPV of 82.5%.16 The recent advancement in NBI-assisted real-time optical diagnosis may be attributed to four primary factors: (1) improved endoscopic systems; (2) more intensive cleaning of polyp surface; (3) use of the appropriate classifications; and (4) more experienced colonoscopists. First, the endoscopic system (Exera III) delivers the NBI technique, which enhances the visibility of vascular and surface patterns by modifying the spectral properties of the illuminating light using an optical filter. Additionally, Exera III has a better imaging display than previous generation systems with greater display screen brightness.6 Using the Olympus pre-freeze fuction, which keeps the most recent image frames in a buffer in the video processor and shows the clearest still image, is also beneficial.17 These systems aid endoscopists in identifying preneoplastic manifestations earlier and more accurately. Second, the cleaner the pre-evaluation polyp surface is, the more accurate the endoscopistŌĆÖs prediction. In our study, simethicone was used for bowel preparation and was added to the auxiliary water pump for intensive cleaning of the polyp surface. This facilitated endoscopic diagnosis by improving the pre-evaluation cleanness of the colonic and lesion surfaces. Third, our study used the NICE classification, a universal tool for optical assessment, which has been validated in many studies for optical histology prediction of small polyps with both NBI and NBI-DF.5,14,16,18 Hewett et al.5 reported that the diagnostic yield can achieve an accuracy of 89%, a sensitivity of 98%, and an NPV of 95% during real-time endoscopy performed by a skilled colonoscopist. The NICE classification was shown to have good inter-observer and intra-observer agreement between more and less experienced endoscopists.5 Fourth, optical diagnosis is also dependent on the expertise of the colonoscopists. In our study, experienced colonoscopists participated in a standardized, continuous training program. Afterward, they performed optical diagnostics in vivo and routinely received feedback on pathology findings to improve their diagnostic performance.
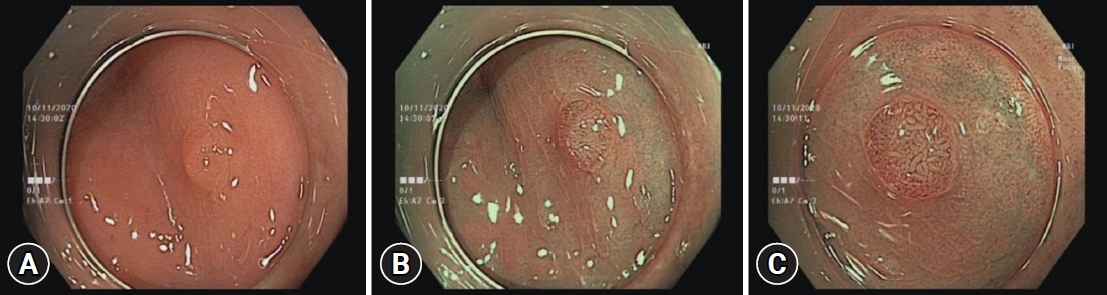
Nevertheless, the endoscopists experienced difficulty in early detection of neoplastic features with WLE, as reflected by the low diagnostic values. Nonetheless, in cases where the colonoscopist could identify any specific neoplastic characteristics, such as depressed or excavated lesion shapes, or tubulogyrus pattern, WLE had an accurate optical neoplastic prediction with a high specificity of 90.4% and a PPV of 88.5% (Fig. 3). A head-to-head comparison of WLE with WLE-DF was not conducted because there is currently no validated classification scheme for predicting neoplastic lesions solely based on WLE, whether with digital or optical magnification.
Regarding NBI-DF, we observed improved sensitivity and accuracy in preliminary diagnoses (from 87.5 to 93.6% and 87.4 to 90.8%, respectively, p<0.001). In accordance with our results, Table 4 summarizes previous reports of NBI-DF, showing positive results regarding its usefulness for real-time optical diagnosis.8,12,17,19-21 The heterogeneity may be due to differing polyp sizes, diagnostic yields of classifications, types of endoscopic equipment, and endoscopistsŌĆÖ experience. Our study was designed specifically for small polyps on a medium scale. Throughout the evaluation, the NICE classification and endoscopic system, which is more popular outside Japan, were utilized. An independent observer was also present to ensure objective evaluation. Moreover, since the medicalŌĆōlegal issue in Vietnam, all specimens must be fully histologically evaluated, so the resect and discard policy is not permitted. Therefore, we decided not to investigate whether adequate accuracy could be achieved to implement the resect and discard strategy.
Previous investigations have reported that magnifying of NBI is useful for assessing the microvascular and surface architecture of premalignant lesions, such as mesh capillaries, oval, and tubular white structures.8,17,19,20 Endoscopists may be able to make improved pathology predictions for lesions by using the magnification function, which can be easily enabled at the press of a button. DF mode magnifies images using natural optical methods, without losing image resolution. The NBI-DF can magnify objects up to 100 times and has a depth of field ranging from 2 to 100 mm. While using traditional magnification, the scope needs to be moved close to the lesion to obtain a clear magnified image (depth of field, 1.5ŌĆō3.0 mm), while in DF mode an enlarged, close-up image can easily be observed by moving the scope tip as close as 2 mm from the mucosa, with a relatively wide depth of field (3.0ŌĆō7.0 mm).6
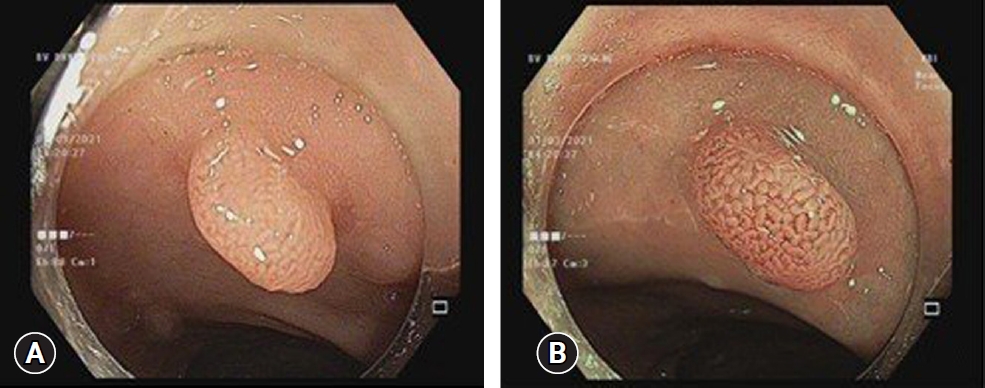
We found that the greatest benefit of adding DF mode over NBI alone for improving diagnosis occurred the Ōēż5 mm group (Fig. 4). Similar to prior observational studies, in the Ōēż5 mm group, NBI-DF had a significantly higher rate of high confidence in predicting neoplastic lesions than NBI, where the proportions of high confidence level ratings in NBI and NBI-DF were 84.2% and 93.4%, respectively (p<0.001).8,17,21,22
With the assistance of DF mode, the endoscopist may more accurately predict the neoplastic nature of diminutive lesions (<5 mm). Although most diminutive polyps are less clinically important than 10-mm polyps with advanced histology, differentiating adenomas from non-neoplastic polyps is meaningful, especially in regions with limited medical resources. Accurately predicting the neoplastic nature of minute colon polyps helps the endoscopist determine which lesions should be removed. As the majority of diminutive polyps were non-neoplastic, unnecessary costs for pathologic examination could be avoided. In the 6 to 9 mm group, neoplastic prediction in NBI mode was not inferior that with NBI-DF magnification; this may be because lesion size affects the proportion of adenomas and the accuracy of neoplastic prediction. Additionally, by using confidence levels, endoscopists with different levels of diagnostic proficiency can be calibrated and standardized, minimizing interobserver variation.9
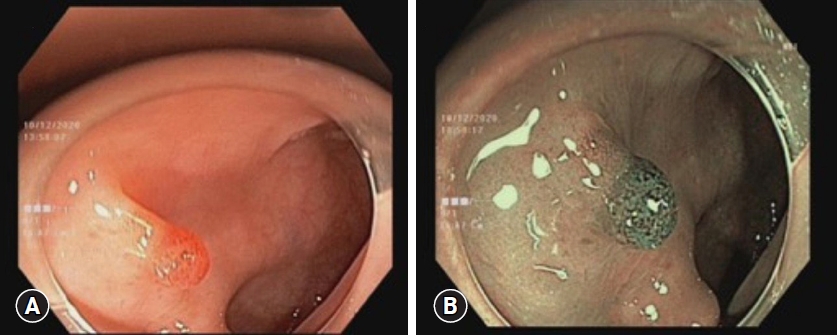
On the other hand, there are several probable reasons for the insufficient diagnostic improvement with NBI-DF. Firstly, factors such as lesion location, the presence of mucus or residual fecal material on a lesion, colonic peristalsis, and breathing or heartbeat movements might hinder real-time optical assessment. This can lead to inability to obtain optimal images for evaluation in NBI-DF mode. Secondly, this technique focuses on angiogenesis, as it enhances the premalignant vascular pattern. For the non-neoplastic optical diagnostic, Szura et al.19 reported there was no observed difference between WLE and NBI-DF. At least 3% to 6% of non-neoplastic lesions could have false positive signs (dark surfaces or visible blood vessels, such as mesh capillaries) leading to misdiagnosis.9,11 These polyps may have a thinner epithelial layer or other layers with congested surfaces caused by inflammation. They factors can impact endoscopic predictions with NBI (Figs. 5, 6).
Our findings may help establish the clinical benefits of NBI-DF and promote wider adoption of magnification-based optical diagnosis in Vietnamese clinical settings where endoscopic equipment is becoming more readily available. Moreover, despite the disparity between academic and general practice, more and more endoscopists are participating in annual training courses on enhanced imaging technology at the academic center. Moreover, magnification can increase the differential optical diagnostic skill of non-expert colonoscopists after extending their training to a threshold at which they become equivalent to experts.22
This study has some limitations. First, this is a single-center study, and each polyp was evaluated subjectively by a single expert colonoscopist in a real-time setting. Further multicenter research is required to validate the reliability and accuracy of using optical diagnosis in Vietnam's routine practice. Second, the adenoma detection rates and interobserver variations between the two endoscopists who evaluated endoscopic findings in this study were not available. Third, some bias during predictions depending on the location, size, gross appearance, and presence of other polyps cannot be excluded. Fourth, all polyps were evaluated with WLE first, followed by NBI and NBI-DF, which may have given the NBI examination an undue advantage (sequence effect). However, if a randomized design (NBI vs. NBI-DF) had been employed, NBI-DF would have been used without NBI, although this would not occur in daily clinical practice.
In conclusion, when used appropriately in experienced hands, real-time NBI-based neoplastic prediction of small colorectal polyps can achieve high accuracy in the Vietnamese clinical setting. The addition of NBI-DF gives significant optical neoplastic prediction improvement for lesions Ōēż5 mm. Our findings underscored the potential clinical value of NBI and NBI-DF in Vietnam, where optical zoom endoscopy is not widely available, in aiding the selection of the most appropriate treatments.