INTRODUCTION
Endoscopic biliary drainage is the gold standard treatment for cholangitis and obstructive jaundice caused by biliary tract infections.1-4 The first choice of treatment for endoscopic biliary drainage is endoscopic retrograde cholangiopancreatography (ERCP). The two methods of biliary drainage are endoscopic biliary stenting (EBS) and endoscopic nasobiliary drainage (ENBD). Evidence suggests that there are no significant differences in the technical success rate, clinical success rate, or adverse event rate between EBS and ENBD, and that the choice depends on the endoscopistŌĆÖs judgment.5-8
EBS does not cause patient discomfort, and there is no risk of self-removal of the drainage tube. However, it does not allow post-stenting cholangiography or monitoring of bile drainage. In contrast, the use of ENBD allows for cholangiography, bile monitoring, and bile duct cleaning. However, self-removal may result in the inability to drain the biliary tract, requiring an additional endoscopic procedure.
A novel integrated outside biliary stent and nasobiliary drainage catheter system has recently been developed (UMIDAS NB stent; Olympus Medical Systems). This system is thought to provide the combined benefits of EBS and ENBD and is expected to be efficacious for acute cholangitis, as the biliary stent remains in the bile duct after removal of the ENBD, allowing continuous biliary drainage.
The outside-type UMIDAS NB stent is a new concept, and its efficacy in acute cholangitis has not yet been elucidated.
In this study, we evaluated the efficacy of the UMIDAS NB stent in the treatment of cholangitis caused by common bile duct stones or distal bile duct strictures.
METHODS
We performed a retrospective pilot study by examining the medical records of patients who required endoscopic biliary drainage for cholangitis due to common bile duct stones or distal bile duct strictures and who were treated with a UMIDAS NB stent, between December 2021 and July 2022.
The diagnosis of cholangitis was made based on the Tokyo Guidelines for Acute Cholangitis 2018 (TG18), and the severity of cholangitis was graded based on the TG18. Mild disease (grade I) was defined as not meeting the criteria for moderate or severe disease. Moderate disease (grade II) was defined as meeting two out of the following five criteria at the time of initial examination: (1) white blood cell (WBC) count >12,000 or WBC <4,000/╬╝L; (2) fever >39┬░C; (3) jaundice (total bilirubin Ōēź5 mg/dL); (4) elderly (aged over 75 years); and (5) albumin (Alb) level <standard level├Ś0.73 g/dL. Severe disease is defined as cholangitis with organ dysfunction.3
The inclusion criteria for the use of the UMIDAS NB stent were as follows: (1) patients in whom endoscopic biliary drainage was possible, (2) aged Ōēź20 years, (3) patients without altered intestinal anatomy after surgery, (4) patients who could undergo ENBD and had consented to ENBD placement, and (5) patients with cholangitis caused by common bile duct stones or distal bile duct strictures.
All included patients were treated with antimicrobial agents in combination with endoscopy. In this study, patients were temporarily discharged from the hospital and managed as outpatients after their cholangitis improved. Stone removal was performed at a later date following the improvement of their cholangitis.
UMIDAS NB stent
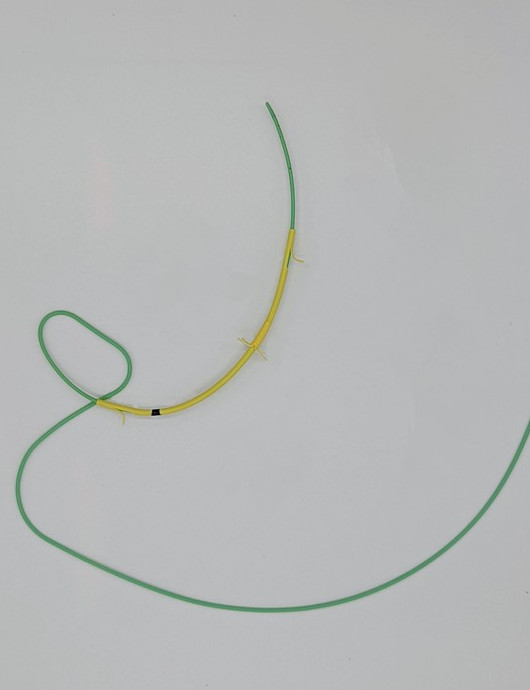
The UMIDAS NB stent is an integrated outside biliary stent and nasobiliary drainage catheter system in which biliary and ENBD catheters are integrated. The ENBD catheter has a straight-tip shape, whereas the biliary stent has a Tannenbaum-shaped flap in the center, which prevents its dislocation into the intestinal tract. When the ENBD catheter is removed, the biliary stent remains in the bile duct. The stent sizes used are usually a 7-Fr biliary stent+4-Fr ENBD or an 8.5-Fr biliary stent+5-Fr ENBD (Fig. 1).
ERCP procedure
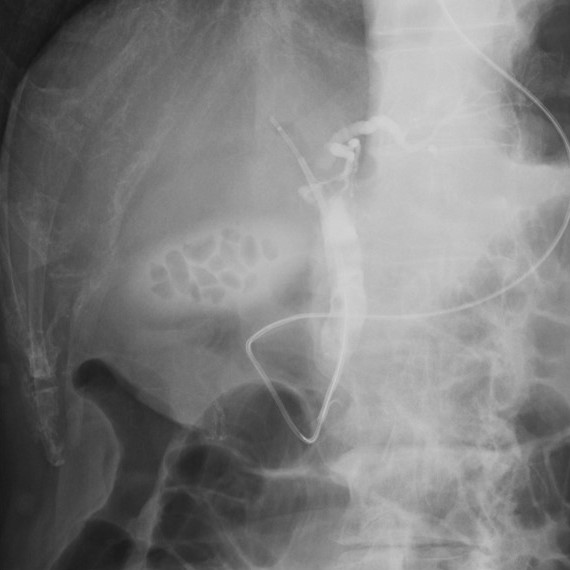
ERCP was performed using a JF-260V or TJF-Q290V endoscope (Olympus Medical Systems) and a contrast catheter was inserted into the bile duct for cholangiography. The evaluation for bile duct stenosis or stones was performed to determine the required length and diameter of the biliary stent. The ENBD catheter was deployed following the insertion of the biliary stent into the bile duct (Fig. 2, Supplementary Video 1). Examinations were performed under fluoroscopic guidance and all patients were sedated with midazolam.
The UMIDAS NB stents were placed without endoscopic sphincterotomy (EST) or endoscopic papillary balloon dilatation (EPBD). Patients who had previously undergone EST or EPBD underwent UMIDAS NB stent placement without any additional papillary procedures. Additionally, the removal of common bile duct stones was performed after the improvement of the cholangitis. Stent insertion after stone removal was not included in the protocol.
Definitions
Technical success was defined as the ability to deploy both a biliary stent and an ENBD catheter. Clinical success was defined as improvement in the cholangitis after endoscopic treatment or improvement in jaundice or liver damage within one week of stent deployment.
Procedure time was defined as the time from endoscope insertion to completion of the procedure. The shift in the position of the ENBD catheter was determined by comparing the position of the ENBD catheter tip with its position immediately after deployment in cases in which fluoroscopy or radiography was available after ENBD deployment. To evaluate the misalignment of the EBS at the time of ENBD removal, we compared the positional changes before and after ENBD removal in cases where the ENBD was removed under fluoroscopic observation.
An early adverse event was defined as any adverse event that occurred within two weeks of endoscopic treatment. A late adverse event was defined as any adverse event that occurred after two weeks. Moreover, adverse events were graded according to the American Society for Gastrointestinal Endoscopy lexicon severity grading system.9
The follow-up period was defined as the day of stent removal or August 31st, 2022. Performance status was defined according to the Eastern Cooperative Oncology Group performance status as follows: PS0, no limitation of activity at all; PS1, able to walk and do light work; PS2, able to walk and perform personal tasks; PS3, spends more than 50% of the day in a sitting or lying position; and PS4, bedridden with no activity at all.10
Statistical analysis
The study analyses included an intention-to-treat analysis of patient characteristics, technical success rate, clinical success rate, and adverse events. The results were presented as numerical values (%) or median values (range) for continuous variables. All statistical analyses were performed using Statistical Product and Service Solutions software (IBM SPSS ver. 26.0; IBM Corp.).
RESULTS
We reviewed the records of 54 consecutive patients who required endoscopic biliary drainage for cholangitis due to common bile duct stones or distal bile duct strictures, and who were treated using the UMIDAS NB stent, between December 2021 and July 2022.
Patient characteristics
The median age of the patients was 70 years. The most common cause of the disease was common bile duct stones (50 patients, 92.6%). The median pre-total bilirubin (T-Bil) level before treatment was 2.92 mg/dL, and the median pre-C-reactive protein (CRP) level was 2.13 mg/dL. The median WBC count was 8,400/┬ĄL before treatment, the median prothrombin timeŌĆōinternational normalized ratio (PT-INR) was 0.85, and the median Alb level was 3.3 mg/dL. The performance status of 88.9% of patients was Ōēż2. TG18 grade I (mild) was applied to 33/54 (61.1%) patients, grade II (moderate) to 18/54 (33.3%), and grade III (severe) to 3/54 (5.6%). The median observation period was 52 days (Table 1).
Procedural outcomes
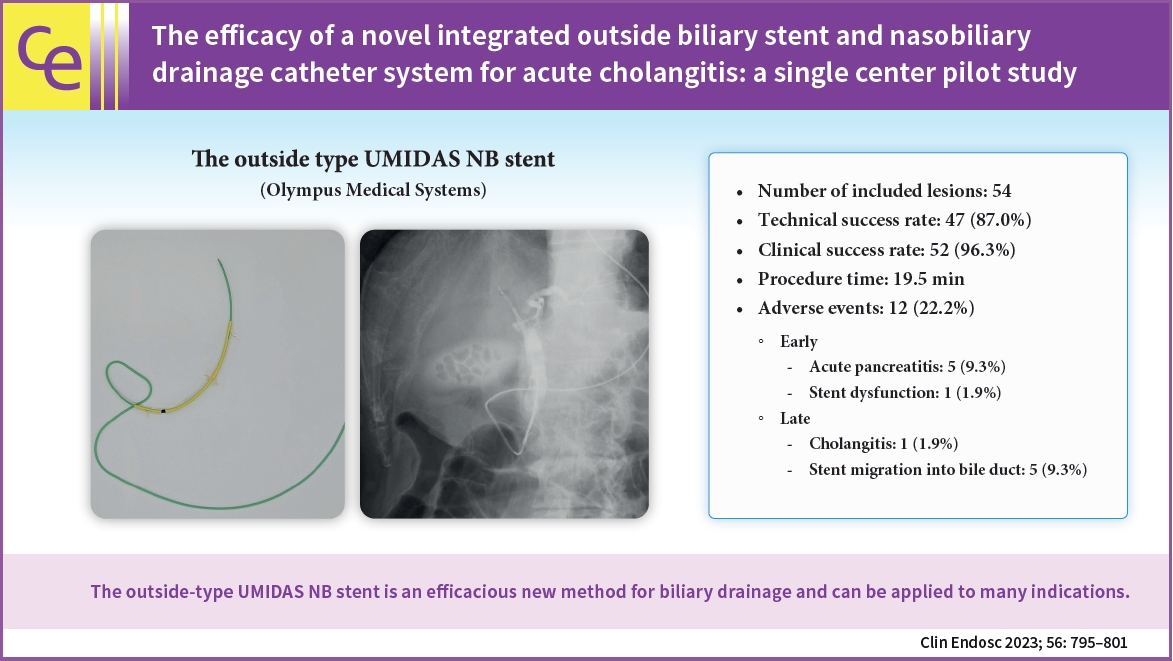
The technical and clinical success rates were 47/54 (87.0%) and 52/54 (96.3%), respectively. An example of procedural failure is catheter traction dislocation during the placement of the ENBD catheter into the nasal cavity. The traction caused by the patient's body motion was attributed as the cause. The redeployment of the ENBD catheter was not performed in any of our cases. The median T-Bil level after treatment was 1.35 mg/dL, and the median WBC, CRP, Alb, PT-INR, and temperature were 5,900/┬ĄL, 0.94 mg/dL, 3.4 mg/dL, 0.94, and 36.9Ōäā, respectively. Disease-related death occurred in one patient. The median procedure time was 19.5 minutes. The most commonly used stent was the 7-Fr and 7 cm biliary stent+4-Fr ENBD catheter (used in 32 [59.3%] patients). The 7-Fr and 5 cm biliary stent+4-Fr ENBD catheter type stent was used in 17 (31.5%) patients. The UMIDAS stent with an 8.5-Fr biliary stent was used in only five (9.3%) patients (Table 2).
Adverse events
Adverse events were observed in 12 patients. Of these, six patients had pancreatitis after ERCP as an early adverse event. Stent dysfunction was also observed as an early adverse event in one patient. Regarding late adverse events, five cases (9.3%) of biliary stent migration into the bile duct were found, and one case of recurrent cholangitis was observed (Table 3).
Outcome following the deployment of the UMIDAS NB stent
Cholangiography from the ENBD catheter was performed in 41 patients (75.9%) after deployment of the UMIDAS NB stent, and self-extraction of the ENBD catheter occurred in six patients. Biliary stent malpositioning did not occur in any case during or after the removal of the ENBD catheter.
Stone removal was performed in 34 patients at the time of biliary stent removal, with a median time between stent placement to stone removal of 49 days (7ŌĆō125 days). Furthermore, biliary stent removal for stone removal or cholangiography was performed in 37 patients (68.5%), with stent removal possible in all patients (Table 4).
DISCUSSION
The gold standard of treatment for acute cholangitis is endoscopic biliary drainage.1-4 ERCP is the first choice. However, the choice of drainage method (EBS or ENBD) is at the discretion of the endoscopist. The UMIDAS NB stent used in this study is a novel integrated outside biliary stent and nasobiliary drainage catheter system. The outside-type UMIDAS NB stent has a wide range of indications, including biliary stasis due to distal bile duct strictures and cholangitis due to common bile duct stones. The shape of this biliary stent is unique, with a Tannenbaum-shaped flap in the center of the stent, which is expected to make stent dislodgement difficult.
In this study, the technical success rate was 87.0%, with seven cases of catheter dislocation during ENBD catheter placement. As the biliary stent remained after the dislocation of the ENBD catheter and biliary drainage was possible, the ENBD catheter was not reinserted. The clinical success rate was 96.3%, with no treatment effect observed in two patients. However, there was one case of disease-related death. Overall, the UMIDAS NB stent was an effective drainage method in our study population. Regarding adverse events, post-ERCP pancreatitis was observed as an early adverse event in five patients (11.1%). Five cases of biliary stent migration into the bile ducts were observed as late adverse events. Pancreatitis was slightly more common than previously reported, although all cases were mild and improved with conservative treatment.11-13 In this study, stenting was performed without EST, which may have increased the risk of developing pancreatitis. EST may not be performed in cholangitis when routine ENBD and EBS are performed because of the urgency of the situation. The findings of this study suggest that EST should be considered with UMIDAS NB stents.
During re-intervention for common bile duct stone removal or bile duct stent replacement, 37 cases of biliary stent removal were performed during the follow-up period. All stents could be removed, but the Tannenbaum-shaped central portion of the plastic stent required careful removal because it had a strong holding force in the bile duct. The Tannenbaum-shaped portion of the plastic stent did not cause dislocation during any of the ENBD removals.
The inside-type UMIDAS NB stent, an integrated inside biliary stent and nasobiliary drainage catheter, has been reported to be useful for hilar stenosis, especially for multiple drainage areas in hilar bile duct cancer.14,15 The outside-type UMIDAS NB stent is considered to have a wider range of indications. In particular, the outside-type UMIDAS NB stent is efficacious in distal bile duct lesions and cholangitis due to common bile duct stones. Moreover, the UMIDAS NB stent may be effective in severe cholangitis requiring bile duct cleaning with an ENBD catheter and for resectable malignant distal bile duct strictures. In cholangiocarcinoma, the ability to perform cholangiography may be useful for preoperative examination. However, in this study, biliary stent migration into the bile duct was observed in 9.3% of patients. For patients with resectable malignant distal bile duct stenosis, recurrent cholangitis and difficulty with biliary stent removal are expected when the stent migrates into the bile duct. Moreover, the procedure is more complicated than the existing EBS and ENBD procedures, and care must be taken to avoid problems, such as ENBD catheter dislocation or plastic stent migration into the bile duct.
The greatest advantage of the UMIDAS NB stent is that the biliary stent remains in the bile duct after the removal of the ENBD catheter. The biliary stent remains in the bile duct even after self-extraction of an ENBD catheter in an elderly patient means that additional endoscopic procedures or biliary drainage are not required. Furthermore, the ability to remove the ENBD catheter after the improvement of cholangitis and to perform bile duct stone removal as an outpatient procedure on a standby basis are considered to be major advantages. In this study, there were six cases of self-extraction of the ENBD catheters. In all cases, the cholangitis had improved without the need for additional biliary drainage.
This study has some limitations. First, it was a single-center retrospective study with a small sample size. In addition, the follow-up period after stent use was short and there was no long-term follow-up.
In conclusion, the outside-type UMIDAS NB stent is a novel system that combines the advantages of EBS and ENBD. This is an efficacious new method of biliary drainage that can be applied to many indications.