INTRODUCTION
Endoscopic resection (ER), including endoscopic mucosal resection (EMR) and endoscopic submucosal dissection (ESD), is a well-established therapy for gastrointestinal neoplasms with a negligible risk of lymph node metastasis.1-7 EMR is a technically easy and time-saving procedure for small lesions; however, the procedure cannot resect lesions with sizes larger than that of the endoscopy snare. In contrast, ESD, which is technically challenging and time-consuming, allows for en bloc resection regardless of the tumor size.8-15 Although ER is widely known as a minimally invasive treatment, complications could occur during and after the procedure. Despite mostly being managed conservatively, some complications are still difficult to treat and cause severe conditions. This review focuses on the prevention and management of complications of upper gastrointestinal ER and summarizes the literature regarding this topic.
ESOPHAGEAL ER
Indications for the treatment of superficial esophageal cancer is described in the ESD/EMR guidelines published by the Japan Gastroenterological Endoscopy Society (JGES).16 According to a meta-analysis of 3,796 patients in 21 retrospective studies, ER for superficial esophageal squamous cell cancer showed favorable long-term outcomes with a five-year overall survival and disease-specific survival of 87.3% and 97.7%, respectively.4 Major complications related to esophageal ER are perforation, bleeding, and stricture. A meta-analysis of eight studies, involving 1,081 patients, revealed that ESD had a lower local recurrence rate and higher perforation rate than EMR; however, there was no significant difference in postoperative stricture and bleeding rates between the two techniques.17
Intraoperative perforations
Intraoperative perforation rates of EMR and ESD were reported to be 0% to 1.6% and 2.6% to 6.9%, respectively.9,18-21 The risk of intraoperative perforation is much higher in cases with large tumor sizes or for procedures in less experienced facilities.22,23 Esophageal ESD is technically challenging because of the following reasons: (1) the narrow lumen of the esophagus decreases the efficacy of gravity counter-traction;8 (2) a resected specimen retracts distally, thereby making it difficult to maintain good traction and orientation;8 (3) the thin wall of the esophagus increases the risk of perforation;8 and (4) localized muscle layer defects lead to unexpected extensive perforations, although these are extremely rare.24 Traction-assisted ESD, which helps maintain a good endoscopic view, is useful in overcoming the challenges mentioned above.25 According to CONNECT-E, a multicenter randomized controlled trial (RCT), no perforation occurred in traction-assisted ESD using dental floss, whereas 4.3% of the cases had perforations in conventional ESD.26 The ESD/EMR guidelines for esophageal cancer published by the JGES weakly recommend traction-assisted ESD.16
Clip closure technique and conservative therapy (e.g., fasting and antibiotic therapy) are the first lines for intraoperative perforation.27 Clip placement should begin at the defectŌĆÖs end distal to the endoscope to provide an optimal endoscopic view.28 Recently, the usefulness of the application of a polyglycolic acid (PGA) sheet has also been reported.29,30
Delayed perforations
Delayed perforations after esophageal ESD can occur, owing to tissue necrosis and degeneration due to excessive energy during the procedure.31 A literature that describes the management of delayed perforations is limited to case reports,31,32 in which the temporary use of self-expanding metallic stents (SEMSs) is reported as a nonsurgical treatment.31 There is no consensus on whether surgical intervention or an endoscopic approach should be performed to manage delayed perforations after esophageal ESD; therefore, a therapeutic decision should be made based on the patientŌĆÖs condition.
Delayed bleeding
Delayed bleeding after esophageal ESD is a relatively rare complication with an incidence rate of 0% to 1.3%.21,22,33 The risk factors for delayed bleeding are not well described in previous reports. Delayed bleeding after esophageal ESD is usually managed with endoscopic hemostasis and does not need surgical intervention.33
Stricture
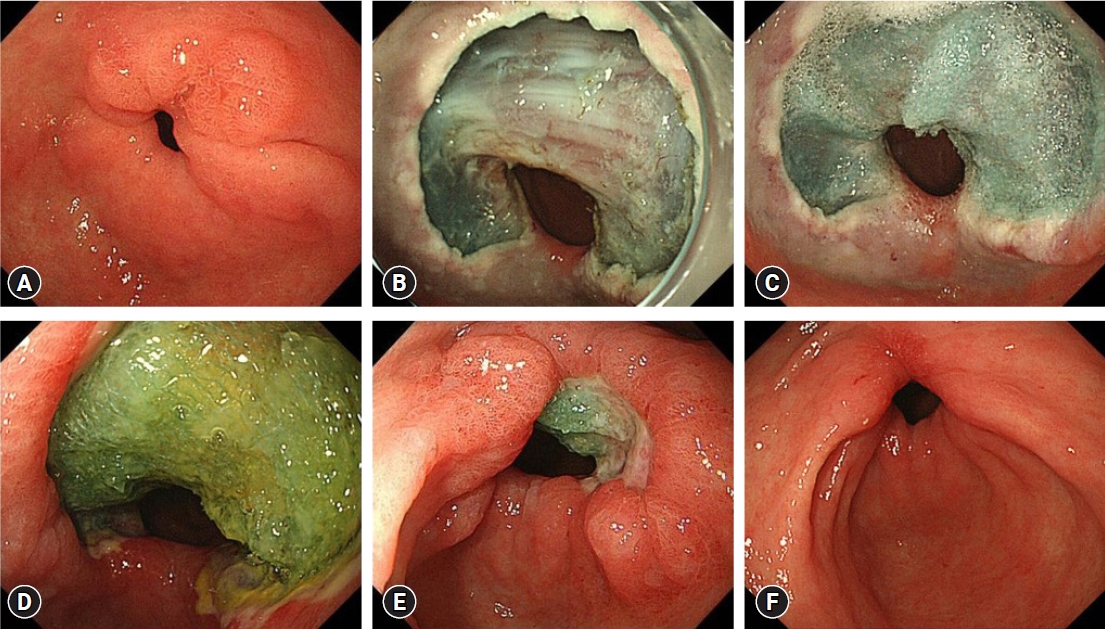
According to Shi et al.,34 the rate of post-ER stricture in patients who underwent esophageal ER for superficial esophageal carcinoma was 11.6% (42/362), and the median time from ER to stricture was 28 days (21ŌĆō90 days). Moreover, the incidence of stricture increases as the circumferential range of the mucosal defect increases (Ōēż1/2 circumferential mucosal defect, 0.7%; 1/2ŌĆō3/4 circumferential mucosal defect, 27.6%; and Ōēź3/4 circumferential mucosal defect, 94.1%). A widespread mucosal defect involving three-quarters of the circumference of the esophagus is a strong risk factor for the development of post-ER stricture.34-36 Several preventive methods and management strategies have been developed for post-ER stricture (Table 1).37-44
1) Stricture prevention methods
Ezoe et al.45 reported that prophylactic endoscopic balloon dilation (EBD) decreases the incidence of post-ESD stricture from 92% to 59% in patients with a mucosal defect covering more than three-quarters of the circumference, and there were no complications after 166 prophylactic EBD procedures were performed for 29 patients. Although prophylactic EBD might be effective in decreasing the incidence of stricture, it could not prevent stricture formation in almost half of the cases. Moreover, several EBD sessions are needed to prevent stricture, thereby leading to a substantial cost and burden for the patients.
SEMS placement has been explored as an option to prevent and treat benign esophageal strictures. Wen et al.37 conducted an RCT on patients with mucosal defects covering more than three-quarters of the circumference, and the incidence of stricture in a stent group was significantly lower than that of a non-stent group (18.2% vs. 72.7%, p<0.05). Stent placement is a simple procedure and might be effective in preventing stenosis; however, there is a risk of stent migration and perforation.
Steroids exert anti-inflammatory effects and reduce collagen synthesis and fibroblast proliferation. Nonaka et al.46 investigated the healing process of esophageal mucosal defects with and without steroid injection using porcine models. The characteristic process underlying the formation of the stenotic luminal ridge is the proliferation of spindle-shaped myofibroblasts at the ulcer bed. Local steroid injection modifies this healing process and contributes to preventing esophageal stricture. Hanaoka et al.38 conducted a prospective study to evaluate the efficacy of single-session local triamcinolone injection (LTI); they revealed that a study group had a significantly lower stricture rate (10% vs. 66%, p<0.001) and lower number of EBD sessions (median value 0, range 0ŌĆō2 vs. median value 2, range 0ŌĆō15, p<0.001) than a historical control group. Yamaguchi et al.39 compared clinical outcomes between oral prednisolone administration (OPA) and preemptive EBD groups in a retrospective study. Post-ESD esophageal stricture was significantly less frequent in the OPA group than in the preemptive EBD group (5.3% vs. 31.8%, p<0.05). Recently, Tanaka et al.40 reported the results of an open-label, multicenter RCT (JCOG1217) investigating the superiority of OPA over LTI for preventing post-ESD stricture. In this study, primary endpoint was stricture-free survival (SFS), and it was 88.5% (95% confidence interval [CI], 81.6%ŌĆō92.9%) in an LTI group and 94.8% (89.4%ŌĆō97.5%) in an OPA group. OPA was not superior to LTI for SFS (hazard ratio, 0.672; 90% CI, 0.361ŌĆō1.250], one-sided p=0.144); This study concluded that LTI is a standard treatment for the prevention of esophageal stricture after ESD for non-circumferential esophageal cancer.
The efficacy of LTI for preventing post-ESD stricture is limited in the case of whole circumferential resection.47 Chu et al.41 reported that LTI plus OPA reduces the incidence of stricture in patients with mucosal defects involving whole or near-whole circumference (>90%) compared with no treatment (18.2% vs. 83.3%, p<0.001), with no refractory stricture occurring in the treatment group. Although the combination therapy showed preferable results for preventing stricture after near-whole circumferential resection, it should be noted that one patient experienced delayed perforation in the treatment group.
Preventive methods other than steroid interventions for postoperative esophageal stricture include tissue shielding methods with a PGA sheet42,48,49 and application of autologous cell sheet transplantation.43,44 A pilot study on the efficacy of PGA sheet for mucosal defects of more than three-quarters of the circumference demonstrated that the incidence of stricture was 37.5% (3/8).49 Sakaguchi et al.42 conducted a single-center retrospective analysis of 500 consecutive cases of esophageal ESD, excluding cervical esophageal cancer and complete circumferential resection. Postoperative stricture rates for PGA sheet with steroid injection, PGA-sheet-alone, and control groups were 18.9%, 41.4%, and 51.7%, respectively (p=0.015).42 Although the PGA-sheet-alone is insufficient in preventing post-ER stricture, a combination of steroid injection and PGA sheet might be effective for non-circumferential resection.
Ohki et al.43,44 developed a technique for endoscopic transplantation of cultured autologous oral mucosal epithelial cell sheets to a post-ER mucosal defect. The incidence of stricture was 10.0% (1/10) in cases with mucosal defect involving more than half of the circumference, and the autologous cell sheets completely epithelialized the mucosal defect after a median of three weeks.43,44 The problems of this novel method include costs of the cell sheet, long procedure time for transplantation, and limited amount of oral mucosa that can be harvested.
Currently, although several other innovative methods have been developed, steroid therapies are still the first-line options for preventing esophageal strictures.
2) Management of strictures
EBD is the standard approach for the treatment of postoperative stricture.27 The success rate of EBD for post-ER stricture is 89.7% (26/29), and median time to treatment success is 4.4 months.50 A balloon dilates the stiff tissue of the postoperative scar with mechanical force; therefore, EBD carries an inevitable risk of perforation.51,52 Takahashi et al.51 reported perforation rates of EBD for post-ESD stricture to be 9.2% (7/76) per patient and 1.1% (7/648) per procedure. Stricture dilation with a balloon >15 mm is a significant risk factor for perforation.53 Therefore, the size of the balloon dilater should be started from 12 mm or less to reduce the risk of perforation during EBD.
Although EBD is an effective approach for postoperative stricture, there are several cases of strictures refractory to repetitive EBD. For these cases, additional treatment should be considered, and radical incision and cutting might be effective methods for refractory strictures.54
GASTRIC ER
The treatment indications for early gastric cancer (EGC) are described in the ESD/EMR guidelines published by the JGES.55 A Japanese multicenter prospective cohort study using a web registry system, including 10,926 lesions from 9,715 patients (J-WEB/EGC), investigated the short- and long-term outcomes of ER for EGC.7,15 En-bloc and R0 resection rates were 99.2% and 91.6%, respectively.15 Moreover, the incidence of adverse events was acceptable, with postoperative bleeding and intraoperative perforation rates of 4.4% and 2.3%, respectively. The five-year overall survival and disease-specific survival rates were 89.0% (95% CI, 88.3%ŌĆō89.6%) and 99.5% (95% CI, 99.3%ŌĆō99.6%), respectively.7 ER for EGC showed favorable short- and long-term outcomes and was widely utilized as a standard approach. In gastric ER, the major complications included perforation, bleeding, and stricture.
Intraoperative perforations
The J-WEB/EGC cohort revealed that intraoperative perforations during gastric ESD occurred in 2.3% of lesions (218/10,821); however, most of them could be treated with conservative management, and only seven cases required emergency surgery.15 Endoscopic clip closure is the first-line therapeutic choice for intraoperative perforations.56,57 Other methods (such as endoloop and endoclip closure method,58 over-the-scope clip [OTSC] method,59 and PGA sheet and fibrin glue60) are used for perforations that are difficult to close completely with the simple clip closure method. The American Gastroenterological AssociationŌĆÖs expert review recommends using standard through-the-scope clips (TTSCs) or OTSCs for perforations Ōēż2 cm and endoscopic suturing or a combination of TTSCs and endoloops for perforations >2 cm.28 The most important factor regarding the indication for emergency surgery is the condition of the patient, including vital signs and symptoms.27,28
Risk factors for intraoperative perforations during gastric ESD include the involvement of the upper third of the stomach, severe fibrosis, invasion depth, and tumor size Ōēź20 mm.61,62 ESD for gastric tumors in the upper third of the stomach is challenging, owing to frequent intraoperative bleeding and thinner wall thickness than that of other parts of the stomach.62 CONNECT-G, a multicenter RCT, demonstrated a lower incidence of perforations in traction-assisted ESD than in conventional ESD (0.3% vs. 2.2%, p=0.01). The traction-assisted technique can reduce the risk of perforations by improving the visibility of the submucosal dissection plane, which helps in the identification of muscle direction during submucosal dissection.63
Delayed perforations
Delayed perforations after gastric ESD are rare, but can cause peritonitis, which requires emergency surgery. A single-center retrospective study of 4,943 cases showed that delayed perforations after gastric ESD occurred only in seven (0.1%) cases, and the median time until delayed perforations was 11 hours (range, 6ŌĆō172 hours).64 Gastric tube cases, lesions located in the upper stomach, and excessive electrocautery are associated with delayed perforations.64,65 Symptoms of peritoneal irritation and rebound tenderness are critical physical signs, indicating a necessity for emergency surgery.65 Although emergency surgery can be required with a high probability,65,66 several cases of delayed perforations were successfully managed conservatively.67,68 Suzuki et al.64 reported that early detection of the onset of delayed perforations within 24 hours after the procedure might be helpful in avoiding emergency surgery. Although no report has described effective prevention methods for delayed perforations, owing to their rarity, complete closure of the mucosal defect theoretically contributes to reducing the incidence of delayed perforations.
Delayed bleeding
Delayed bleeding is a major complication related to gastric ESD. Although administering proton pump inhibitors (PPIs) and prophylactic coagulation after ESD are reportedly effective for preventing delayed bleeding,69-71 the incidence of delayed bleeding remains as high as 2.6% to 5.8%.15,72,73 A meta-analysis indicated that significant risk factors for delayed bleeding after gastric ESD were the use of antithrombotic agents, chronic kidney disease, resected specimen size >30 mm, and use of histamine-2 receptor antagonists instead of PPIs.74 Hatta et al.75 reported the BEST-J score, which is a novel scoring system for predicting delayed bleeding using risk factors, such as comorbidities, tumor factors, and use of antithrombotic agents. This prediction model stratifies the risk of delayed bleeding into four levels, according to the total score of risk factors: low-risk (0ŌĆō1 point; 2.8%), intermediate-risk (2 points; 6.1%), high-risk (3ŌĆō4 points; 11.4%), and very high-risk (Ōēź5 points; 29.7%) (Table 2).75 Notably, the management of antithrombotic agents in the BEST-J score is based on the 2014 JGES guideline,76 which does not include the management of direct oral anticoagulants.
Second-look endoscopy (SLE) has been empirically performed to prevent delayed bleeding; however, three RCTs revealed that routine SLE did not reduce delayed bleeding in patients with an average risk of bleeding.77-79 Furthermore, in a single-center retrospective study, there was no statistical difference in the incidence of delayed bleeding between SLE and non-SLE groups in patients taking antithrombotic agents (21.7% vs. 21.9%, respectively).80 There is no prospective study investigating the efficacy of SLE in a high-risk group, and the indication of SLE in high-risk patients remains unclear.
Several researchers have developed innovative approaches, such as tissue shielding methods (PGA sheets and fibrin glue) (Fig. 1),81,82 endoscopic closure of artificial ulcers (the endoloop and endoclip closure method, OTSCs, and hand-suturing method),83-86 and the use of hemostatic powder,87,88 for the prevention of delayed bleeding. These methods are particularly used in high-risk patients.
Kataoka et al.81 conducted an RCT that investigated the efficacy of PGA sheets and fibrin glue in high-risk patients. There was no significant difference in delayed bleeding rates between PGA and control groups (4.5% vs. 5.7%, p>0.99). Although this study enrolled high-risk patients, delayed bleeding occurred in only 5.7% of the control group; this incidence rate is equivalent to that of low-risk patients.81 This result implies that the inclusion criteria were not optimal. Therefore, further well-designed and advanced large-scale studies are required to provide evidence for PGA sheets in the prevention of delayed bleeding.
Endoscopic closure of mucosal defects (including the endoloop and endoclip closure method,83 OTSCs,84 and hand-suturing method85,86) has a clinical potential to reduce the risk of delayed bleeding (Table 3). However, it is difficult to achieve complete closure of a gastric mucosal defect and avoid dehiscence because of the thickness of the gastric wall. Endoloop and endoclip closure method is an easy-to-perform and low-cost procedure, but it is not satisfactory in keeping the mucosal defect closed.83 Ego et al.83 reported that the endoloop and endoclip closure method did not prevent delayed bleeding in patients with antithrombotic therapy compared with control individuals (11.5% vs. 11.9%, p=0.89), and sustained closure rate in patients who underwent SLE was 47.8% (33/69). Endoscopic hand-suturing (EHS) demonstrated an incredibly high rate of complete closure (97%ŌĆō100%) and sustained closure of mucosal defects (84%ŌĆō100%).85,86 Akimoto et al.85 reported that there was no delayed bleeding in patients taking antithrombotic agents without perioperative cessation (0%, 0/20). EHS is a promising method for achieving complete and sustained closure, thereby allowing for the prevention of delayed bleeding. However, EHS is a technically challenging and time-consuming procedure. Further improvement is required to utilize EHS in clinical practice. Polysaccharide hemostatic powder (PHP) is a novel topical hemostatic method used for non-variceal upper gastrointestinal bleeding,89 and its efficacy for preventing post-ER bleeding has been investigated.87,88 Jung et al.87 conducted an RCT to investigate the efficacy of PHP in preventing post-ESD bleeding among patients with a high risk of bleeding (resected specimen size >40 mm and regular use of antithrombotic agents). This study showed that there was no significant difference in post-ESD bleeding rates between PHP and control groups (5.5% vs. 7.1%, p=0.74). However, a subgroup analysis of patients who discontinued antithrombotic agents during ESD showed that post-ESD bleeding rate tended to be lower in the PHP group than in the control group (0% vs. 6.3%, p=0.06).
Considering the increasing population of patients taking antithrombotic agents, the development of an effective preventive method for delayed bleeding is desirable. However, there is no RCT demonstrating the efficacy of preventive approaches. This topic is still under investigation, and further innovative methods are required.
Stricture
It is reported that stricture occurs in 0.8% to 2.5% of cases following gastric ESD.90-93 An extensive mucosal defect that comprises three-quarters of the circumference in the antrum or cardia is a significant risk factor for stenosis.91 An EBD is empirically performed to alleviate stricture and stasis symptoms; however, it carries a certain risk of perforation (7.8%ŌĆō14.3%).91,94 Moreover, cases of post-gastric ESD stricture require repeated EBD until the stricture is eliminated, and there are cases of strictures refractory to repeated EBD. Contrary to esophageal stricture, there is limited evidence for preventive methods, such as local steroid injection and prophylactic EBD for stricture following gastric ESD.94,95 Further investigations should be conducted to determine the optimal approach for preventing strictures.
DUODENAL ER
According to a large-scale national database in Japan, the incidence of duodenal cancer was 23.7 per 1,000,000 person-years.96 Almost half of duodenal cancers were detected at the localized stage (56.4%, 1,694/3,005), and 48.0% (813/1,694) of localized duodenal cancers were endoscopically resected.96 Although duodenal cancer is rare, the number of ER procedures for duodenal tumors has been increasing with the development of endoscopic modalities.97 ER of duodenal neoplasms is still challenging due to the anatomic characteristics of the duodenum, such as the tortuous duodenal lumen, thin wall, and exposure to bile and pancreatic juices. Several previous studies have shown preferable clinical outcomes of underwater EMR (UEMR) and cold snare polypectomy, and these novel ER techniques are among therapeutic options for duodenal neoplasms.98-102 Major complications associated with duodenal ER are perforation and bleeding, which substantially differ among the procedures (Table 4).98-105
Perforations
A multicenter retrospective observational study, including 3,107 cases (187, 579, 1,324, and 1,017 cases of cold polypectomy, UEMR, conventional EMR, and ESD, respectively) revealed that intraoperative perforation and delayed perforation rates were significantly higher in an ESD group than in other groups.103 Fukuhara et al.106 analyzed the clinical course of 32 patients with intraoperative perforations during duodenal ESD. Either simple closure using clips or the string clip suturing technique was attempted to close a perforation, and complete closure was achieved in 13 of 32 patients (40.6%). They found that if the whole mucosal defect, including the perforation, was closed completely, the clinical course was significantly better than that of incomplete closure and was equivalent to that of cases without perforations. Moreover, incomplete closure cases with an endoscopic nasobiliary and pancreatic duct drainage tube (ENBPD tube) could be managed without additional intervention. However, one of eight cases with neither complete closure nor an ENBPD tube required percutaneous drainage for an abscess. An ENBPD tube might prevent mucosal defect exposure to pancreatic and bile juices and help to avoid a worse clinical course in a case without complete closure of the mucosal defect.
Delayed perforations
Delayed perforation is a more severe complication than intraoperative perforation and requires emergency surgery. A meta-analysis revealed that the incidence of delayed perforations in a closure group tended to be lower than that in an unclosed group, although it was not statistically different (1.6% vs. 3.8%, p=0.13; risk ratio, 0.39; 95% CI, 0.12ŌĆō1.32).107 Complete closure of the mucosal defect might help to reduce the risk of delayed perforations; however, it is sometimes difficult to achieve complete closure for a lesion in the medial or anterior wall and in lesion size >40 mm.108 In order to overcome these difficulties, various endoscopic closure techniques (the clip with string method, endoloop and endoclip closure method, OTSCs, and PGA sheets) were developed.109-113 Moreover, external drainage of bile and pancreatic juices using an ENBPD tube might be a therapeutic option for preventing delayed perforation in cases of difficult complete mucosal defect closure. Fukuhara et al.114 reported that no patients developed delayed perforation (0/21) with immediate insertion of ENPBD tubes after duodenal ESD, whereas 4.1% (2/49) of the patients who did not undergo ENBPD tube insertion developed delayed perforations. It should be noted that ENBPD has a risk of post-endoscopic retrograde cholangiopancreatography pancreatitis and mucosal defect perforation when inserting a side-viewing endoscope. Therefore, the indications for ENBPD should be limited to cases in which endoscopic closure is impossible or difficult.
Delayed bleeding
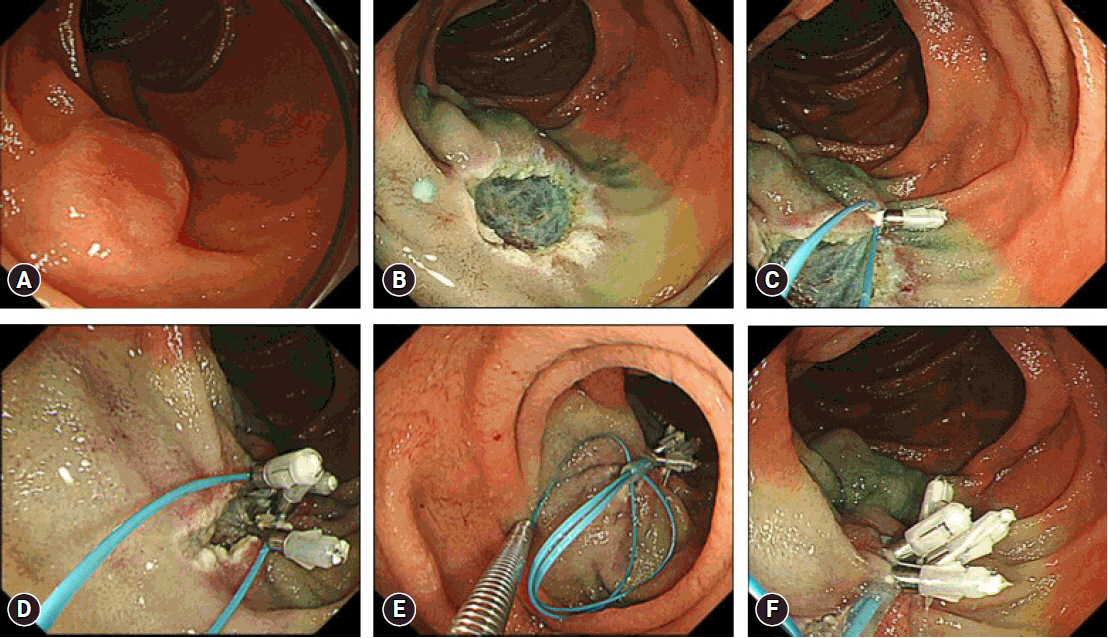
The incidence of delayed bleeding in cold polypectomy, UEMR, conventional EMR, and ESD are 0% to 0.5%, 0% to 2.1%, 0% to 2.6%, and 4.7% to 5.2%, respectively.98-105 A meta-analysis revealed that the incidence of delayed bleeding was significantly lower in a closure group than in an unclosed group (2.0% vs. 17.3%, p<0.01; risk ratio, 0.14; 95% CI, 0.06ŌĆō0.33).107 Simple endoscopic clip closure is the standard method for closing mucosal defect after ER of duodenal neoplasms. However, it is technically challenging to achieve complete closure of extensive mucosal defects, particularly after ESD. Thus, various endoscopic closure techniques (the clip with string method, endoloop and endoclip closure method, OTSCs, and PGA sheets) are reported to prevent delayed bleeding after ER of duodenal neoplasms (Fig. 2).109-113 These studies are single-arm descriptive studies or case reports with small samples. A clinician can determine a preferred method based on procedural difficulty and device availability and cost. A database analysis using propensity-score matching demonstrated that vonoprazan significantly reduced the incidence of delayed bleeding compared with PPIs following duodenal ESD.115 However, it should be noted that this study did not consider the effect of endoscopic preventive procedures after duodenal ESD.
In summary, endoscopic closure of post-ER mucosal defect is highly recommended for preventing delayed bleeding. The indications for ER of duodenal neoplasms should be determined based on the technical difficulty of defect closure, as well as resection.
CONCLUSIONS
We reviewed complications related to ER of upper gastrointestinal neoplasms. Despite the low incidence of complications, it is critical for clinicians to properly manage adverse events during and after ER because serious complications can result in emergency surgery. Although basic management has been standardized for many of the complications, appropriate preventive methods have not yet been established, particularly for strictures after extensive esophageal and gastric ESD and for delayed bleeding after gastric ESD. Further innovative and large-scale prospective studies are warranted to solve the issues and provide better patient cases in real clinical practice.