Endoscopic Treatment for Early Foregut Neuroendocrine Tumors
Article information
Abstract
Foregut neuroendocrine tumors (NETs) include those arising in the esophagus, stomach, pancreas, and duodenum and seem to have a broad range of clinical behavior from benign to metastatic. Several factors including the advent of screening endoscopy may be related to increased incidence of gastrointestinal NETs; thus, many foregut NETs are diagnosed at an early stage. Early foregut NETs, such as those of the stomach and duodenum, can be managed with endoscopic treatment because of a low frequency of lymph node and distant metastases. However, controversy continues concerning the optimal management of early foregut NETs due to a lack of controlled prospective studies. Several issues such as indications, technical issues, and outcomes of endoscopic treatment for early foregut NETs are reviewed based on some published studies.
INTRODUCTION
Neuroendocrine tumors (NETs) are defined as epithelial neoplasms with predominant neuroendocrine differentiation, arising throughout the body. Gastrointestinal NETs can be classified into foregut, midgut, or hindgut depending on the point of origin in the disseminated endocrine system.1 Foregut NETs include those arising in the esophagus, stomach, pancreas, and duodenum. The new histologic grading system of 2010 World Health Organization classification for digestive system NETs that could be applied to all stages of neuroendocrine neoplasms (NENs) separates well-differentiated tumors into low grade (G1) and intermediate grade (G2) categories. All poorly differentiated NETs are high grade (G3) neuroendocrine carcinomas according to this classification scheme (Table 1).2-4
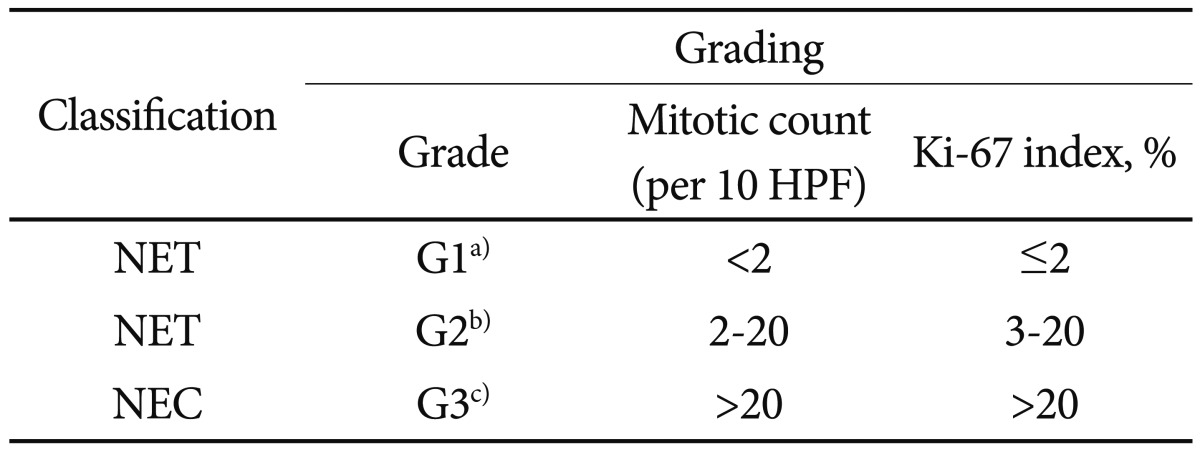
World Health Organization 2010 Classification and Suggested Grading of Neuroendocrine Neoplasms of the Digestive System
Foregut NETs seem to have a broad range of clinical behavior from benign to metastatic. The treatment of choice for a localized NET is usually surgery. Many foregut NETs are diagnosed at an early stage because of the advent of screening endoscopy and, thus, can be managed with endoscopic treatment because of a low frequency of lymph node and distant metastases. However, controversy continues concerning the optimal management of early foregut NETs due to a lack of controlled prospective studies. These debatable issues on endoscopic treatment for early foregut NETs are discussed based on some published data.
EPIDEMIOLOGY OF FOREGUT NETs
The incidence of NETs is reported to be rising in Western countries and Asia.5-8 In the United States, a significant increase in reported annual age-adjusted incidence of NETs from 1973 (1.09/100,000) to 2004 (5.25/100,000) was reported.5 Also, the incidence of NETs in Taiwan increased steadily from 1996 (0.30/100,000) to 2008 (1.51/100,000).6 Despite such increase, the incidence rate of NETs in Taiwan is lower than that of Norway and the United States.5-7 Many factors may contribute to increase the incidence of NETs around the world. These factors can be a better awareness, improved diagnostic strategies, and increased and more widespread use of gastrointestinal endoscopy.7,9-14 The distribution of gastrointestinal NETs seemed to be different between Japan and Western countries.8 The distribution of gastrointestinal NETs in the United States is reported to be 19.4% in the foregut, 38.7% in the midgut, and 41.9% in the hindgut.5 In contrast, in Japanese population, 30.4% were in the foregut, 9.6% in the midgut, and 60.0% in the hindgut.8
NENs OF THE ESOPHAGUS
Esophageal NENs are extremely rare. Most cases of esophageal NENs are poorly differentiated endocrine carcinoma (PDEC) and mixed adenoneuroendocrine carcinoma. The few reported cases have been mostly treated by esophagogastrectomy.1
NENs OF THE STOMACH
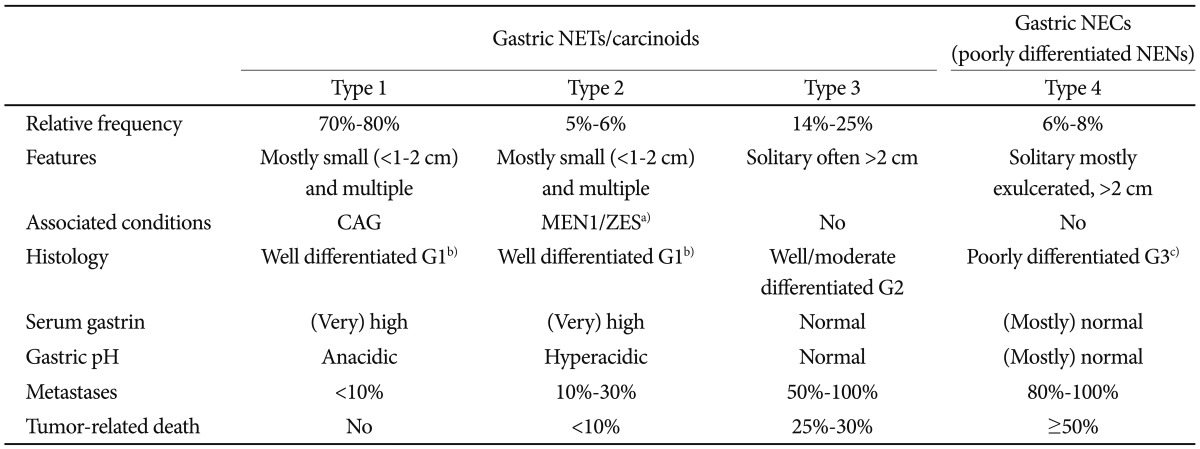
The stomach is the most common foregut location for NETs. Gastric NETs comprise 7% of all gastrointestinal NETs and 2% of all removed gastric polyps.15,16 Four types of gastric NENs have been proposed and recognition of the type is important for defining the diagnostic approach and treatment. Gastric NENs are subdivided into four categories, with differing biologic behaviors and prognoses: type 1, arising on atrophic body gastritis; type 2, a manifestation of type I multiple endocrine neoplasia (MEN-I); type 3, with no specific background disease; type 4, poorly differentiated NENs (Table 2).17
Therapy of Gastric Neuroendocrine Neoplasms
Type 1 gastric NET is the most common type and tends to be nearly all benign lesions, with a low risk for progression or metastasis. The type 1 is mostly diagnosed at an early stage, with 80% to 90% of them being ≤1 cm in diameter.12
Diagnosis of early NETs of the stomach
Endoscopy is the only method to detect early gastric NETs that are usually asymptomatic. Widespread use of gastrointestinal endoscopy and endoscopic screening may lead to increased detection of small sized gastric NETs.12 Well-differentiated NETs of the stomach (gastric carcinoid tumors) are observed more often, with a 10-fold increase in the United States in the last 35 years, and the prognosis has improved greatly in that time.5 Small, less than 1 cm, well-differentiated (G1) NETs of the stomach that do not infiltrate the muscularis propria and do not show angioinvasion have a very low risk of metastatic spread, that are considered early NETs of the stomach.17
Type 1 gastric NETs are usually detected during endoscopy as lesions greater than 5 mm in diameter. It is important to perform additional sampling biopsies of the surrounding mucosa of the stomach to assess microcarcinoids and to identify the condition of the background gastric mucosa.18
Several serum markers can be valuable in diagnosis and surveillance of type 1 gastric NETs. Chromogranin A (CgA) level is increased in 80% to 90% of patients with type 1 gastric NETs.19-21 However, serum CgA level may be increased in hypergastrinemia, enterochromaffin-like cells hyperplasia, nonfunctioning tumors of the endocrine pancreas and medulllary thyroid cancers;22 thus, increased CgA level may not indicate the presence of gastric NETs. CgA level can be useful as a surveillance marker for progression of NETs. Several studies have demonstrated significant decrease in CgA level after both medical therapy and surgical treatment of NETs.23-25 Possible other markers for identifying gastric NETs are synaptophysin, vesicular monoamine transporter and VMAT-2.26-28
Endoscopic ultrasound is very useful for determining exact tumor size and depth of invasion. However, endoscopic ultrasound is not essential for type 1 gastric NETs measuring less than 1 cm, because those generally do not infiltrate the muscular layer.17 Abdominal ultrasound and computed tomography/magnetic resonance imaging are not useful for early type 1 or 2 gastric NETs. Somatostatin receptor scintigraphy (Octreoscan) has been used since the early 1990s as a methods of localizing both primary and metastatic tumors expressing somatostatin receptors.29 However, Octreoscan is often negative in early type 1 and 2 gastric NETs. Also, standard 18F-fluorodeoxyglucose positron emission tomography is also of limited value when assessing gastric NETs.29
Prognosis of early NETs of the stomach
Type 1 gastric NETs is the most common type of the gastric NENs which is usually detected at early stage. Most of them are less than 1 cm in diameter.12 Type 2 gastric NETs, similar to type 1 are usually diagnosed at an early stage, thus having an excellent long term prognosis.17 A retrospective study from Italy showed that there was no tumor-related death at an overall mean follow-up of 53 months in 152 patients with type 1 gastric NETs and only one tumor-related death 49 months after diagnosis at an overall mean survival of 84 months in 12 patients with type 2 gastric NETs.30 Ravizza et al.31 observed 11 patients with type 1 gastric NETs each less than 1 cm in diameter. No patients had any evidence of local or distant metastases at a median follow-up of 54 months. However, four of the 11 patients (36%) had an increased number of lesions. This uncontrolled small study may indicate that small type 1 gastric NETs can be followed without any surgical or medical treatments.
Merola et al.32 recently investigated clinical outcome and recurrence of type 1 gastric NETs treated by endoscopic approach in 33 patients. At diagnosis, seven tumors were intramucosal carcinoids and 26 were polyps (median diameter 5 mm, range 2 to 20), multiple in 17 patients. After removal of tumors by endoscopic methods, patients were managed by endoscopic follow-up every 6 to 12 months. During a 46-month median follow-up, survival was 100% and no metastases occurred. Twenty-one patients (63.6%) had recurrence after a median of 8 months, 14 of these (66.6%) had a second recurrence after a median of 8 months following the previous carcinoid removal. Median recurrence-free survival was 24 months. These results indicate that endoscopic management for early type 1 gastric NETs may be considered safe and effective.
Treatment of early NETs of the stomach
Endoscopic resection is the treatment of choice for early NETs of the stomach.17 Small, less than 1 cm in diameter, well-differentiated (G1) NETs of the stomach that do not infiltrate the muscularis propria and do not show angioinvasion have a very low risk of metastatic spread. Thus, early, G1-differentiated NETs of the stomach should be removed by endoscopic methods.17 However, a large retrospective study using Niigata Registry from Japan showed that even in minute (≤5 mm in diameter) and small (5.1 to 10 mm in diameter) gastric NETs at a depth of invasion restricted to the mucosa and submucosa (sm carcinoids), metastases rate were 4.6% and 9.6%, respectively. These metastatic rates are compatible with those of gastric sm adenocarcinoma.33 This result suggest that when treating patients with early gastric NETs, possibility of metastases should be considered. However, the 5-year survival rates of patients with gastric sm carcinoids after endoscopic resection was 89.6%.
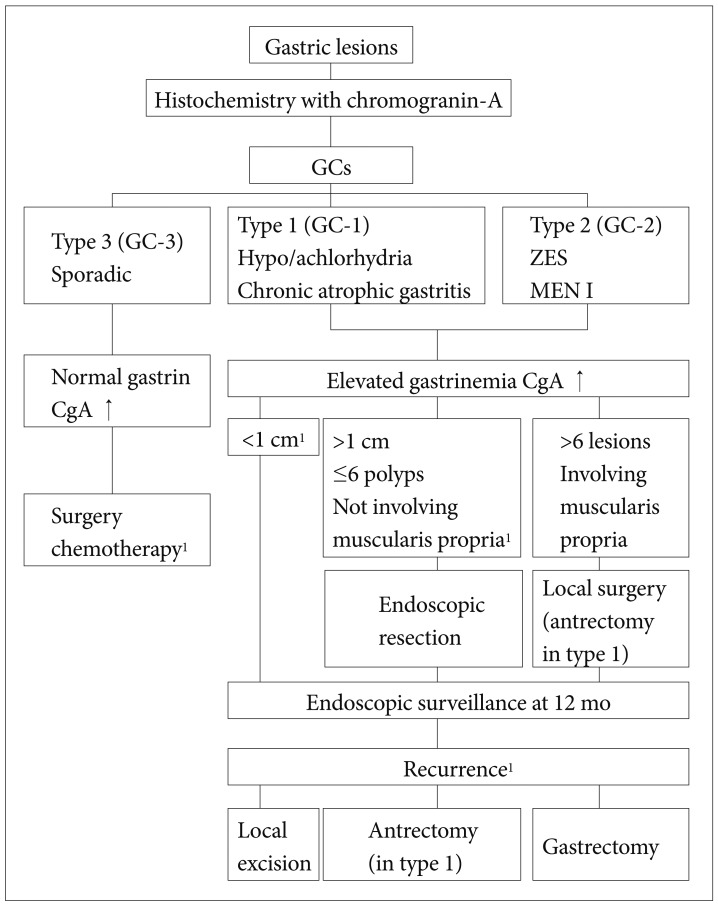
In the European Neuroendocrine Tumor Society Consensus Guidelines for managements of gastroenteropancreatic NETs (including carcinoid)34 management of type 3 gastric carcinoids is fairly clear and includes partial or total gastrectomy with extended lymph node dissection. Management of type 1 and type 2 gastric carcinoids is more controversial. In patients with type 1 gastric carcinoids less than 10 mm in diameter, annual surveillance is appropriate. Endoscopic resection is recommended in cases of tumors >10 mm in diameter and in the presence of up to six polyps not involving the muscularis propria at EUS examination (Fig. 1).29,34
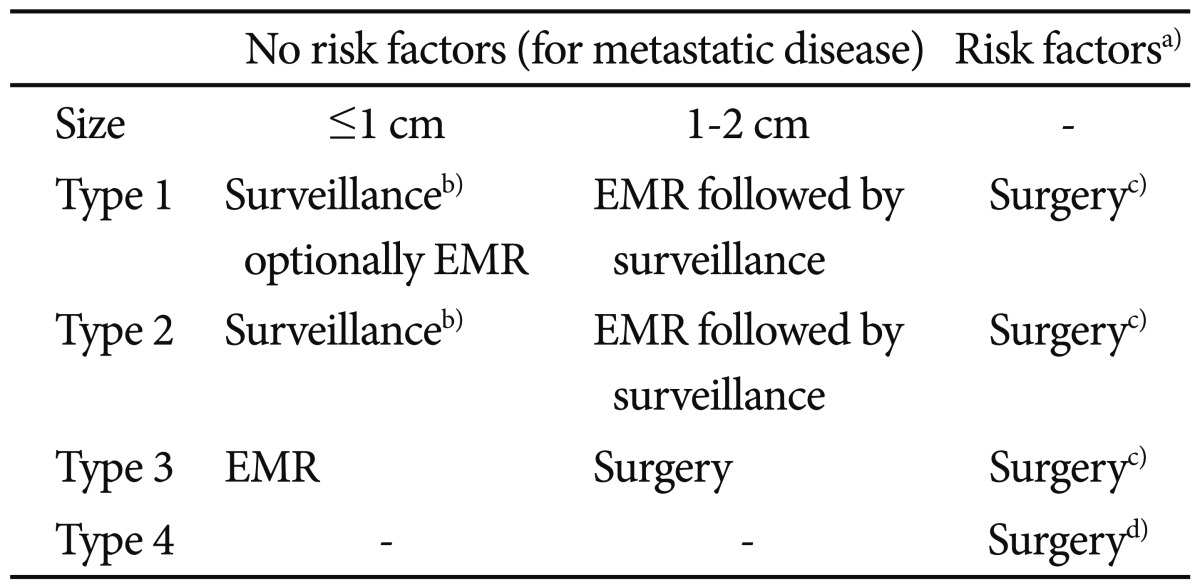
The management of G1 NETs sized 1 to 2 cm is a matter of debate. There are no controlled studies that compared endoscopic treatment with surgical approach. In case of type 1 or 2 gastric NETs of 1 to 2 cm in diameter, the endoscopic treatment should be preferred to surgery in patients with significant comorbidities and in elderly patients with a high surgical risk (Table 3).17
Clinicopathological Characteristics of Gastric Neuroendocrine Neoplasms
Another issue we should consider is a method of endoscopic treatments. Endoscopic submucosal dissection technique can increase complete resection rate compare with other techniques, such as endoscopic polypectomy, strip biopsy, aspiration resection, and band snare resection.32,35-41
Rescue surgery after endoscopic resection should be considered in certain properties of foregut NETs. The indication for additional surgery is usually based on the location, type, grade, and stage of the foregut NETs. In the case of type 1 or type 2 gastric NETs with positive margins, size >20 mm, G2-G3 histologic grading, invasion into the muscularis propria or vessel infiltration of tumor cells, additional surgery is recommended.12 In the case of type 3 gastric NETs with a size >10 mm, irrespective of other risk factors, and localized type 4, rescue surgery is necessary.12
NENs OF THE DUODENUM
Primary duodenal NETs account for less than 2% of all gastrointestinal NETs.42 Five major types of NETs can be seen in the duodenum: 1) gastrinomas (type I) are most common and are usually seen in the proximal duodenum. One third is associated with ZES and MEN1; 2) second in frequency are somatostatinomas (type II), which often have a periampullary location. They may be associated with von Recklinghausen disease; 3) gangliocytic paragangliomas (type III) are benign tumors found at the ampulla or in the periampullary region; 4) type IV is rare and contains tumors that produce serotonin and calcitonin; and 5) PDECs (type V) is extremely rare and highly malignant and is usually located at the ampulla of Vater.43
Diagnosis of early NETs of the duodenum
Most duodenal NETs are asymptomatic and generally diagnosed during upper gastrointestinal endoscopy for unrelated symptoms. In addition, duodenal NETs are usually hormonally silent. Upper gastrointestinal endoscopy is the only method of choice to detect early duodenal NETs.17
In a retrospective analysis of duodenal carcinoid tumors, Burke et al.44 identified three pathologic features of the primary tumor as independent risk factors for metastasis: invasion of the muscularis propria, tumor size greater than 2 cm, and the presence of mitotic figures. A retrospective study from Mayo Clinic showed that 18 of 19 patients with tumors smaller than 2 cm remained disease free after local (endoscopic or transduodenal) excision.38
Early duodenal NETs can be considered if tumors are ≤10 mm in size, G1, show neither angioinvasion nor infiltration of the muscular layer, have no associated hormonal secretion and have a very low metastatic potential.17
Treatment of early NETs of the duodenum
No consensus guidelines exist for the endoscopic management of duodenal NETs. Multiple factors must be taken into account when considering treatment options. Well-differentiated, nonfunctioning duodenal NETs with no evidence of invasion to the muscularis layer and 1 cm or less in size can be endoscopically removed (Table 4).17 These tumors carry a low risk for lymphatic or distant metastasis. In case of duodenal carcinoids more than 1 cm in size, the option of management is a matter of debate. A recent case series from Japan showed complete and safe results of endoscopic resection for duodenal bulb NETs more than 10 mm in size.41
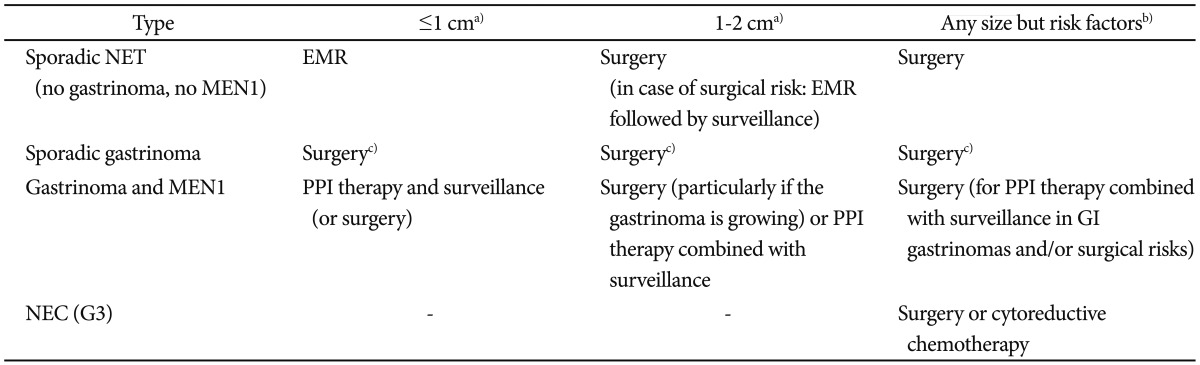
Therapy of Duodenal Neuroendocrine Neoplasms
CONCLUSIONS
Endoscopic treatment may be one of therapeutic options for eligible foregut NETs. However, the appropriate selection criteria of foregut NETs for endoscopic resection is still controversial and further studies are needed.
Notes
The author has no financial conflicts of interest.