Small Bowel Stent-in-Stent Placement for Malignant Small Bowel Obstruction Using a Balloon-Assisted Overtube Technique
Article information
Abstract
Self-expanding metal stents are a useful therapy to palliate malignant and benign luminal gastrointestinal obstruction. Self-expanding metal stents has been widely reported for colonic, esophageal, and gastric obstruction. However, endoscopic delivery and placement to the small bowel is more challenging and difficult. This case illustrates the usefulness and technical advantages of the balloon-overtube and enteroscopy technique for the palliative treatment of neoplastic stenosis affecting the small intestine.
INTRODUCTION
Self-expanding metal stents (SEMSs) are a useful therapy to palliate malignant and benign luminal gastrointestinal (GI) obstruction.1 Although SEMS placement has been widely reported for colonic, esophageal, and gastric obstructions,2-5 little is known about its applicability for small bowel strictures. SEMS placement into the small bowel is more challenging. Here, we present a balloon overtube technique that enabled successful SEMS placement in the distal duodenum.
CASE REPORT
An 80-year-old woman who underwent a pylorus-preserving Whipple procedure 6 years previous for pancreatic head cancer and recurrent disease with duodenal obstruction of the previous placement of two palliative SEMSs was referred to our institution for bowel obstruction distal to the ligament of Treitz. The stents had been placed 2 years and 11 months prior, respectively. Placement of a third stent using esophagogastroduodenoscopy and standard and pediatric colonoscopes had failed. We used a double-balloon enteroscope (DBE) to perform the procedure. The previously placed SEMS was obstructed owing to ingrowth with tissue and the small bowel kinking distally to the stent (Fig. 1). A large amount of impacted food was removed by flushing and suctioning. Using endoscopic and fluoroscopic visualization, the enteroscope was carefully advanced into the jejunum after dilating the stricture. After the scope was advanced, the overtube was gently pushed across the dilation. Deep enteroscopy was then performed, and no other obstructions were found in the afferent or efferent limbs. The Roux-en-Y anastomosis was located approximately 50 cm distal to the pylorus.
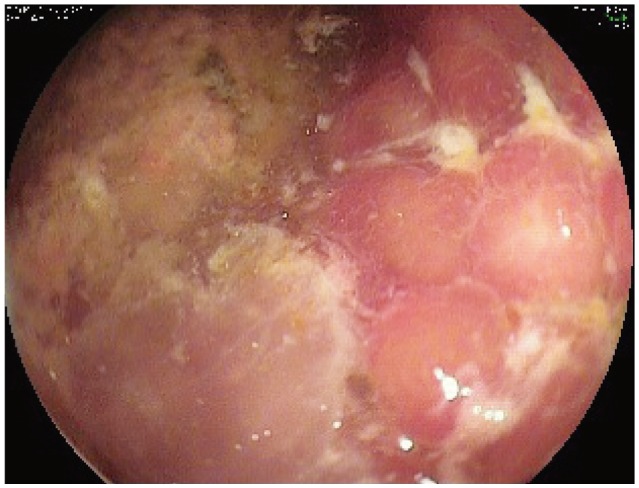
The previously placed self-expanding metal stent was obstructed owing to tissue ingrowth and the small bowel kinking distally to the stent.
A new SEMS (90-mm length, 10-mm diameter; Boston Scientific, Natick, MA, USA) was inserted across the previous two SEMS using the herein described balloon overtube technique using the following six steps. First, the enteroscope was kept across the stenosis in the upper jejunum (Fig. 2). Second, a Jagwire guidewire (Boston Scientific) was inserted in the jejunum (Figs. 2, 3). Third, the scope was removed under fluoroscopic guidance and the wire was left in place (Fig. 4). Fourth, the overtube, which was looped and kinked in the J-shaped stomach, was straightened (Fig. 5). A trick was used to straighten the overtube without losing its position; that is, the balloon of the overtube was inflated distally to the stent. This maneuver allowed the overtube tip to get hooked to the distal part of the overtube while being pulled (i.e., straightened). The overtube straightening was essential to advance the stent through the wire inside the overtube and across the previous stents (Fig. 6; step 5). Sixth, the distal part of the stent was deployed under fluoroscopic guidance while the now deflated overtube was carefully brought back into the stomach through the old stent, thus permitting the new stent to deploy distal to the old stent and the overtube tip across the obstruction (Figs. 6, 7). The patient is asymptomatic 3 months after the procedure.
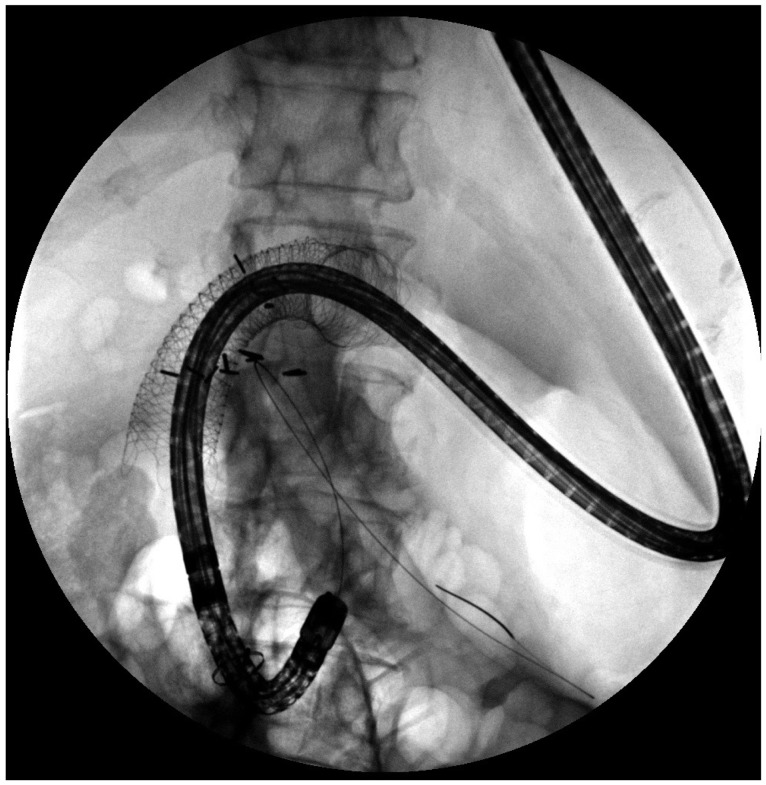
The enteroscope was introduced into the overtube, across the stenosis, and into the jejunum.

The scope was removed under fluoroscopic guidance, leaving the wire in place inside the overtube across the small bowel stricture.
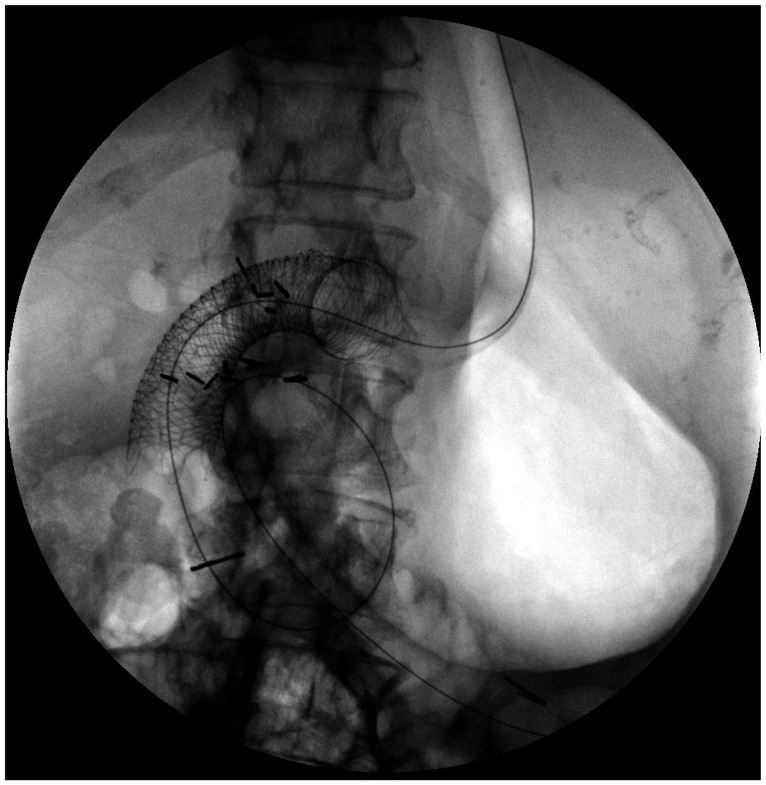
The overtube now lies along the lesser curvature of the stomach. On previous attempts without an overtube in place, the stent followed the wire along the greater curvature, making it practically impossible to place the stent across the previous stents.
Overtube straightening was essential to advance the stent over the wire through the tube and then across the previous stents.
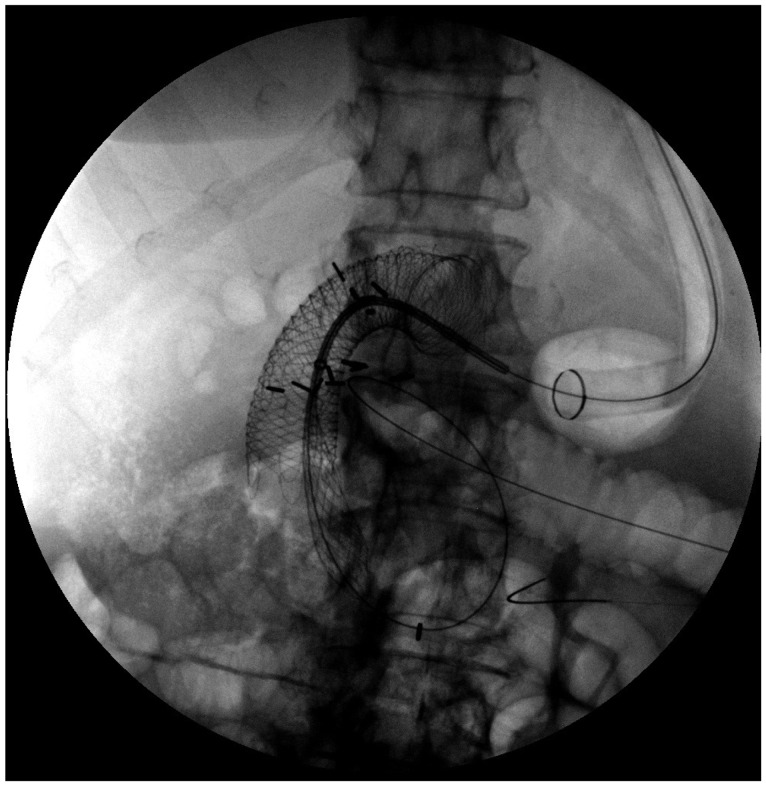
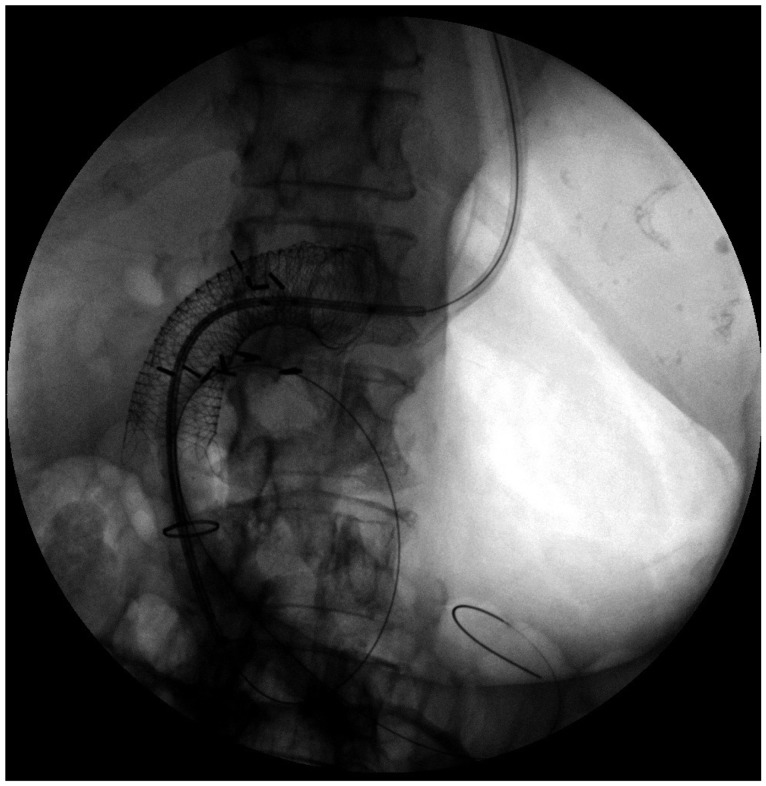
The distal part of the stent was deployed under fluoroscopic guidance while the now deflated overtube was carefully brought back into the stomach through the old stent, thus permitting deployment of the new stent distal to the old stent and the overtube tip across the obstruction.

Full deployment of stent-in-stent with perfect distal positioning is confirmed.
DISCUSSION
Malignant small bowel obstruction usually results from primary small bowel malignant neoplasm, invasive locoregional tumors or metastasis.1,6-9 SEMSs represent a potential palliative measure.6-9 In an interesting study, Lee et al.6 describe the usefulness of the DBE technique to advance a wire through malignant small bowel strictures to enable SEMS placement. In that study, the authors passed another scope along the wire to visualize and aid the stent insertion. In our case, we used an overtube as an extralarge working channel. Although a similar technique using spiral single-balloon enteroscopy and spiral enteroscopy was previously described,7-9 our case is of additional interest because we describe in detail all the steps necessary to perform a balloon overtube placement of a SEMS into the proximal small bowel. In addition, limited data are available on this technique.10
SEMS placement within the small bowel is challenging for both anatomic and mechanical reasons. The anatomic challenge is caused by the shape of the stomach and small bowel. The technical challenge includes the tortuous endoscope position and limitations of the stent delivery devices, which are often stiff and inflexible, that disallows easy travel through angled or long curves of the GI tract, such as a J-shaped stomach and the duodenal sweep. In this case, we show how a balloon overtube helped to overcome most of this challenges, allowing for accurate SEMS placement. Use of the DBE permitted the placement of the overtube distal to the previously placed metal stent. Inflation of the overtube balloon allowed for the tube to be straightened while remaining hooked distal to the stent. The straightened overtube allowed us to advance the stent over a previously placed floppy guidewire. Although stent placement through the endoscopic channel is feasible, the previously placed SEMS and the angulated position of the distal duodenum prevented us from choosing this option. Although several overtubes are available for use during endoscopy, our technique using the balloon overtube is unique, adds to the interventional endoscopist's armamentarium, and represents another useful option for SEMS placement in the small bowel. In summary, we recommend that clinicians consider using an overtube or balloon overtube when placing stents into difficult locations within the GI tract.
Notes
The authors have no financial conflicts of interest.