Korean Society of Gastrointestinal Endoscopy Guidelines for Endoscope Reprocessing
Article information
Abstract
The Korean Society of Gastrointestinal Endoscopy (KSGE) issued guidelines for endoscope reprocessing for the first time in 1995, and the version of the guidelines was updated in August 2009, August 2012, and March 2015. Guidelines for endoscope reprocessing should be revised continuously, because new disinfectants and devices are developed and introduced. The current official version of the KSGE guidelines for endoscope reprocessing is explained herein to assist the reader in understanding the KSGE requirements for cleaning and disinfecting endoscopes.
INTRODUCTION
The Korean Society of Gastrointestinal Endoscopy (KSGE) issued guidelines for endoscope reprocessing for the first time in 1995, and the version of the guidelines was updated in August 2009, August 2012, and March 2015 (Table 1). Among the sections within the guidelines, the disinfection section is being used as an evaluation standard for hospital certification and quality of endoscopy for cancer screening. The current version of the KSGE guidelines for endoscope reprocessing is explained herein to assist the reader in understanding the KSGE requirements for cleaning and disinfecting endoscopes. These guidelines have been established after a thorough review of previous reports and guidelines [1-11] by The Disinfection Management and Conscious Sedation Committee, KSGE.
Korean Society of Gastrointestinal Endoscopy Guidelines for Endoscope Reprocessing: Update 2015
GUIDELINES FOR ENDOSCOPE REPROCESSING
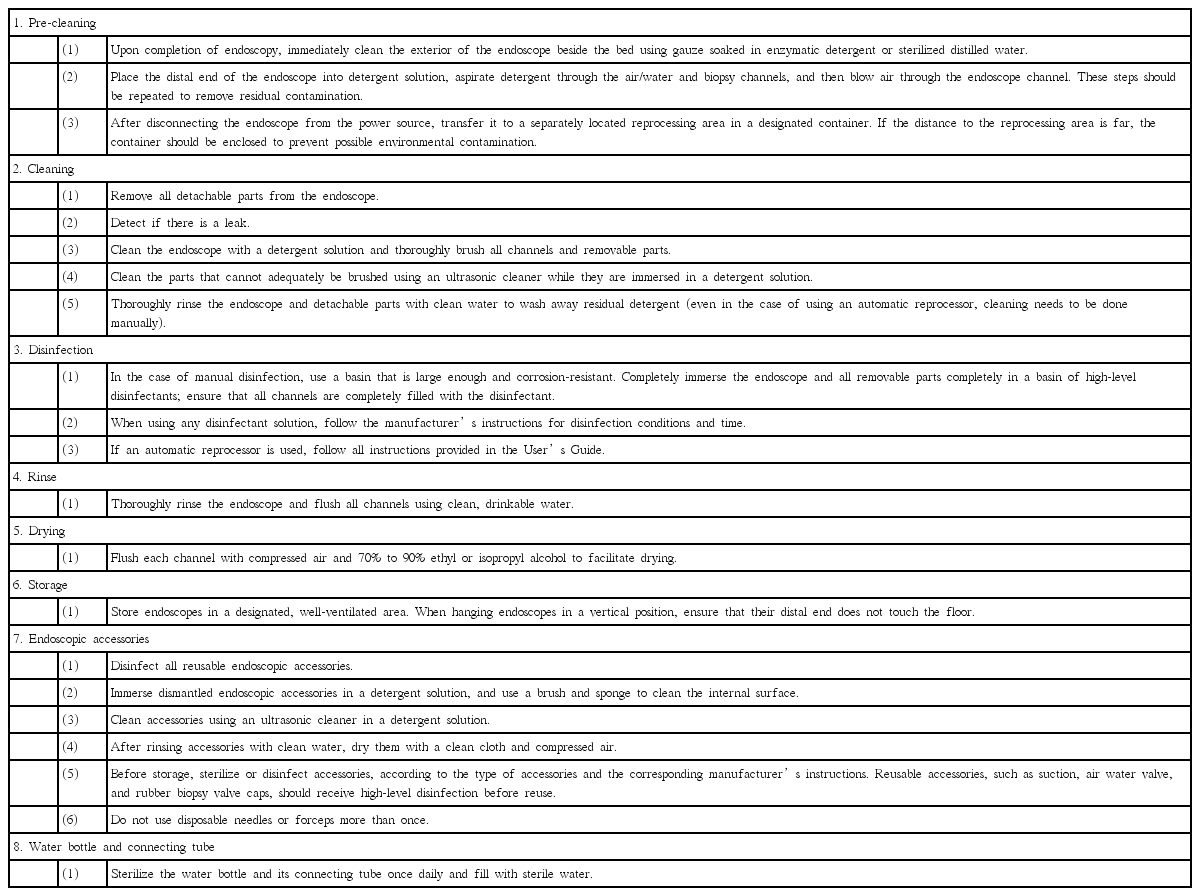
1. Pre-cleaning
(1) Upon completion of endoscopy, immediately wipe the exterior of the endoscope beside the bed using gauze soaked in enzymatic detergent or sterilized distilled water.
Explanation: Enzymatic detergent components may vary among manufacturers, but they are commonly effective in decontaminating an endoscope contaminated with blood, polysaccharides, lipids and biofilm during endoscopy.
(2) After placing the distal end of the endoscope into detergent solution, aspirate a large volume of detergent solution through the air/water and biopsy channels and then blow air through the endoscope channel. These steps should be repeated to remove residual contamination.
Explanation: One can clean a contaminated endoscope more efficiently by alternating aspiration of the detergent solution and blowing air through the endoscope channel than just aspirating the detergent solution, such as enzymatic or neutral detergent or distilled water. If this pre-cleaning process is not performed immediately after completion of endoscopy, debris, such as blood and secretion, will lead to clogs within the channel, which cannot be removed completely even through the subsequent disinfection process. When the pre-cleaning step is finished, disconnect the endoscope from the power outlet.
(3) Then, transfer the endoscope to the reprocessing area, which is separated from the procedure room, to a designated container. If the reprocessing area is not nearby, the container should be enclosed to prevent environmental contamination.
Explanation: The reprocessing area should be physically separate from the procedure room, if possible, and equipped with adequate reprocessing equipment. Good ventilation is essential in the reprocessing area to prevent personnel from being exposed to the toxicity of disinfectants used for reprocessing. The reprocessing area should be divided into clean and dirty areas to avoid cross contaminating the former. There should be designated and adequate space between contaminated endoscopes and clean ones. To minimize the risks of transmitting infections, place contaminated endoscopes in a designated container, and transport them from the procedure room to a separately located reprocessing room. The transport container should be large enough to prevent damage that may occur if the distal end is coiled tightly. Use an enclosed container or bag if the distance to the reprocessing room is far.
2. Cleaning
(1) Disconnect and disassemble all detachable parts from the endoscope.
Explanation: Disconnect and disassemble suction valves, air water valves, and rubber biopsy valve caps for cleaning and disinfection.
(2) Perform leak testing.
Explanation: Perform leak testing to detect any damage to the interior or exterior of the endoscope, according to the manufacturer’s instructions. As moisture inside the endoscope can lead to malfunction, function of the water-resistant cap should be inspected through leak testing. Leak testing can be performed manually or with a leak tester. Immerse and soak the endoscope in water and carefully observe if there is a stream of air bubbles coming out of the interior of the endoscope. A continuous stream of air bubbles indicates the presence of a leak. In such cases, repair the endoscope before continuing to clean it. Leak testing should be performed before the disinfection cycle. If a leak is not detected, continue to clean the endoscope. Cleaning an endoscope after failed a leak test will cause further damage. Before cleaning, leak testing must be performed to ensure there are no leaks.
(3) Perform manual cleaning with a cleaning solution; thorough brushing of the channels and other detachable parts is required.
Explanation: After checking that the endoscope is free from damage, clean the exterior of the endoscope with a soft cloth or sponge while it is immersed in a detergent solution. Use brushes that are compatible in size with the channels to clean removable debris completely from the inside of the channels. Use a detergent solution that can effectively penetrate and remove debris formed by protein, fat, carbohydrates, and various chemical salts without harming the scope being cleaned. Enzymatic detergent or medical grade, low-foaming neutral detergent solutions are recommended. Foaming can prevent the detergent solution from contacting the endoscope. A soft cloth or sponge should be used once. If not, ensure it is disinfected or sterilized before reuse. All channels and detachable parts should be brushed.
(4) Clean the parts that cannot adequately be brushed using an ultrasonic cleaner while they are immersed in a detergent solution.
(5) After endoscope cleaning, thoroughly rinse the endoscope and detachable parts with clean water to wash away residual detergent (even in the case of using an automatic reprocessor, cleaning needs to be done manually).
3. Disinfection
(1) In case of manual disinfection, use a basin that is large enough and corrosion-resistant. Completely immerse the endoscope and all detachable parts completely in a basin of high-level disinfectants; ensure that all channels are completely filled with the disinfectant.
Explanation: Completely immerse the endoscope and detachable parts in a high-level disinfectant solution and ensure that all channels are filled with the disinfectant solution and that no air pockets remain within the channels. Air pockets can allow microorganisms to survive the high-level disinfection process, making disinfection ineffective. Although most high-level disinfectants are reusable, prolonged and repeated use of the same disinfectants reduces the optimal concentrations and effectiveness of disinfection. Minimum effective concentration of disinfectants should be checked to maintain the level of effective disinfection. If the disinfectant solution fails to meet the minimum concentration in a test conducted before use, dispose it. Additionally, disinfectants should not be used after their expiration date.
(2) When using any disinfectant solution, follow the manufacturer’s instructions for disinfectant conditions and time.
Explanation: Use disinfectant solutions approved by the Ministry of Food and Drug Safety in Korea, United States Food and Drug Administration, Conformité Européene in Europe, and Japanese Ministry of Health, Labor, and Welfare (including those permitted, reported, or registered).
(3) If an automatic reprocessor is used, follow all instructions provided in the User’s Guide.
Explanation: An automatic reprocessor is recommended, because it can perform a standardized disinfection process and reduce personnel exposure to disinfectants.
4. Rinse
(1) After high-level disinfection, thoroughly rinse the endoscope and flush all channels using clean, drinkable water.
Explanation: Thoroughly rinse the endoscope and flush all channels of the endoscope using sterile water, because residual disinfectants can cause injury of the skin and mucous membrane. The volume of water needed for adequate rinsing is equal to three times the total area to be rinsed. For instance, to rinse an internal channel, at least 150 mL of water is required.
5. Drying
(1) After reprocessing, flush each channel with compressed air and 70% to 90% ethyl or isopropyl alcohol to facilitate drying.
Explanation: As moisture breeds microbial bacteria such as Pseudomonas aeruginosa to multiply, drying is a crucial procedure in reprocessing. Keep flushing with alcohol until the alcohol can be seen at the opposite end of each channel. Alcohol helps residual water evaporate as air flows through the channel. Caution is needed because excessively high air pressure can damage the internal channels of the endoscope.
6. Storage
(1) Store endoscopes in a designated, well-ventilated area. When hanging endoscopes in a vertical position, ensure that their distal end does not touch the floor.
Explanation: Decontaminated endoscopes should be stored separately from contaminated endoscopes in a clean, dust-free area. Hang endoscopes in a vertical position in a cabinet while all detachable parts are still removed. Store channels, suction valves, air water valve and water-resistant caps separately from the endoscope to prevent clogs. Make sure that the endoscopes hang freely in a vertical position in a clean, well-ventilated, dust-free cabinet. Keep the cabinet clean by wiping the inside everyday with an eco-friendly disinfectant.
7. Endoscopic accessories
(1) Disinfect all reusable endoscopic accessories.
(2) Immerse dismantled endoscopic accessories in a detergent solution, and use a brush and sponge to clean the internal surfaces.
(3) Clean accessories using an ultrasonic cleaner in a detergent solution.
(4) After rinsing accessories with clean water, dry them with a clean cloth and compressed air.
(5) Before storage, sterilize or disinfect accessories, according to the type of accessory and the corresponding manufacturer’s instructions. Reusable accessories, such as suction, air water valve, and rubber biopsy valve caps, should receive high-level disinfection before reuse.
Explanation: Endoscopic accessories include all detachable parts of the endoscope and devices inserted into the channels. Major devices include biopsy forceps, the hook wire, guide wire, and balloon dilator. All accessories that penetrate the mucosal membrane are recommended for use only once or sterilized before reuse. Sterilization refers to a process that eliminates and destroys all microorganisms, including spores through physical and chemical means.
(6) Do not use disposable needles or forceps more than once.
Explanation: Proper reprocessing of endoscopic accessories is crucial, but it is also important to consider that repeated sterilization and reuse can gradually reduce the effectiveness of the accessories. In the case of biopsy forceps, repeated reprocessing may cause damage to the forceps, because they are not durable, making them more susceptible to contamination. Biopsy forceps have been reprocessed and reused in a cost-effective way. However, biopsy forceps are increasingly used only once in many countries, and Lim et al. [12] reported that the clinical relevance of biopsy forceps was greater when they were used only once. Additionally, single-use biopsy forceps can be cost-effective if the reprocessing costs are high. However, disposable biopsy forceps must be used for patients with infectious diseases to prevent the spread of infection. The guidelines for using disposable needles are increasing in Europe.
8. Water bottle and connecting tube
(1) Sterilize the water bottle and its connecting tube once daily and fill with sterile water.
Explanation: To date, there has been no report of the optimal replacement frequency, safety, and potential risks associated with water bottle, lens wash water, tubing for air insufflation, waste vacuum container, and suction tube used in endoscopy. However, these accessories should be disinfected once daily and contain sterile water.
CONCLUSIONS
The KSGE guidelines are compiled based on international guidelines to provide global standards for endoscope reprocessing. Compliance with this guidance will minimize the risk of transmission of endoscopy-related infection.
Notes
Conflicts of Interest: The authors have no financial conflicts of interest.
Acknowledgements
The Disinfection Management and Conscious Sedation Committee, Korean Society of Gastrointestinal Endoscopy greatly appreciate Jinsu Kim (The Catholic University of Korea), Jae-Young Jang (Kyung Hee University), Ja Seol Koo (Korea University College of Medicine), and Jung Ho Park (Sungkyunkwan University) for their sincere devotion to preparing this guideline