INTRODUCTION
Tumors of the small bowel comprise fewer than 2% of gastrointestinal (GI) malignancies. Benign small bowel tumors are usually asymptomatic, but sometimes can cause small bowel obstruction via the development of intussusceptions.1-7
The diagnosis of small bowel lesions is often delayed due to the difficulty of access with conventional endoscopy. However, recent advances allow the entire small bowel to be fully evaluated by capsule endoscopy or balloon-assisted enteroscopy. Balloon-assisted enteroscopy has advantages over other diagnostic modalities for the detection of small bowel lesions due to its capabilities of real-time observation, tissue biopsy and therapeutic intervention.3,8-10
We report a case of asymptomatic small bowel inflammatory polyp that was resected endoscopically using double-balloon enteroscopy (DBE) in a patient who previously underwent total gastrectomy.
CASE REPORT
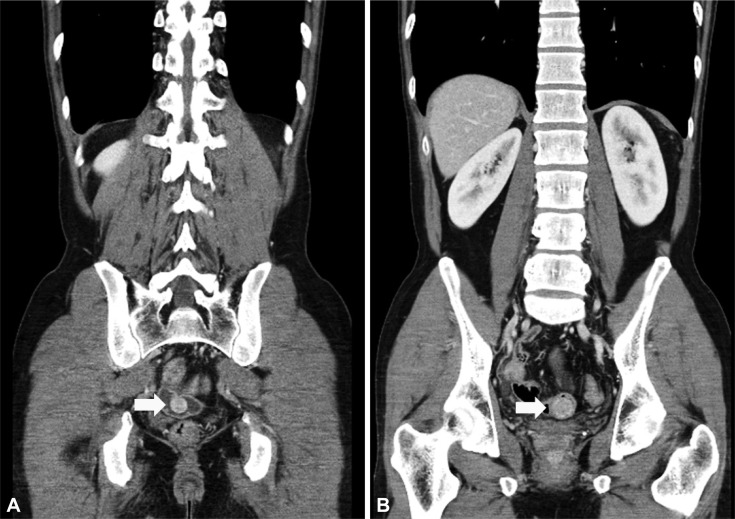
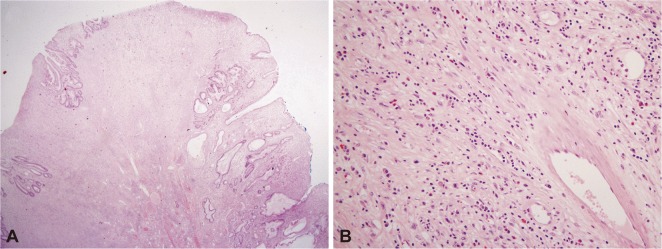
A 39-year-old man was referred to our department for the evaluation of a small bowel mass detected on abdominal computed tomography (CT). He had previously undergone total gastrectomy due to early gastric cancer (T1NOM0) 7 years before referral. After surgery, abdominal CT scan was performed annually and a 1 cm ileal mass was detected on the abdominal CT scan 6 years after the operation. But the patient did not want further evaluation and equipments like DBE was unavailable. A repeat abdominal CT scan one year later showed that the mass had increased in size to about 2.5 cm (Fig. 1). The patient had no associated symptoms. Upon presentation to our clinic, the patient's physical examination and laboratory findings were normal. We first tried conventional colonoscopy, but were unable to access the lesion. Therefore, we performed retrograde DBE (Fujinon EN-450P5/20; Fuji Photo Optical Co., Ltd., Omiya, Japan) and detected a large, pedunculated polyp in the distal ileum, located 50 to 60 cm from the ileocecal valve. After the injection of an indigocarmine-epinephrine mixture at the base of the polyp, a snare polypectomy was performed. Argon plasma coagulation was performed to treat minor bleeding at the polypectomy site (Fig. 2). The total procedure time was 50 minutes. Gross pathologic examination showed a 2.5У2.5 cm lobulated and pedunculated polyp with a wide stalk. The results of the histologic examination were consistent with the diagnosis of inflammatory polyp (Fig. 3). The patient was discharged without complications after the procedure.
DISCUSSION
Inflammatory polyp is a non-neoplastic, proliferating lesion of the gastro-intestinal tract. They most often occur in the stomach, but can occur in any part of the GI tract. Ileal inflammatory polyps are rare benign tumors of the small bowel, and most reports of ileal inflammatory polyps are fibroid polyps that are characterized by the stromal polyps composed of fibrous tissues infiltrated by inflammatory cells, particularly eosinophils. The pathogenesis of inflammatory polyp is unknown, but it is believed that abnormal inflammatory response is associated with the onset process. Microscopically, inflammatory polyps can be mistaken for granulation tissue or sarcoma because of spindle-shape cells. Endoscopically, inflammatory polyps are usually less than 4 cm, but several cases of larger polyps up to 20 cm have been also reported. There is no clear evidence so far whether the polyp grows to a certain size or continues growing.11 In a previous case study, inflammatory polyps were detected in 18% of the small bowels, with the ileum the most frequent site. Patients with small bowel inflammatory polyps are typically asymptomatic until the onset of complications such as small bowel obstruction due to intussusception or bleeding.3,6 Most case reports of inflammatory polyps are complicated cases with intussusceptions or bleeding that were diagnosed and treated by surgical resection.1,2,4,5,7
Small bowel lesions cannot be evaluated by conventional endoscopy. With recent advances, however, the entire small bowel can now be fully evaluated by balloon-assisted enteroscopy and capsule endoscopy. For example, endoscopic resection of small bowel polyps with DBE is an effective and safe treatment that can prevent emergency surgery due to intussusception in patients with Peutz-Jegher syndrome. Balloon-assisted enteroscopy may be a useful tool for preoperative diagnoses of primary etiology in cases of intussusception, and endoscopic decompression of intussusception may be possible in selected cases.8,10,12 Miyata et al.3 reported a case of small bowel intussusception due to inflammatory polyp that was preoperatively diagnosed using DBE. Minimal laparoscopic resection could be performed by the shortening intussusception.
Our patient had a past history of abdominal surgery and an asymptomatic ileal mass that increased in size over time. Abdominal CT was unable to characterize the exact nature of this lesion, although a pedunculated mass was suspected. Therefore, the diagnosis of our patient was uncertain due to lack of further evaluation. Using DBE, a large pedunculated polypoid mass with the characteristics of an inflammatory polyp was detected and easily resected with a conventional snare without complications such as bleeding or perforation. Therefore, pathologic diagnosis and therapeutic removal could be achieved simultaneously, and additional surgical procedures could be avoided.
As far as we know, only one other case of inflammatory polyp resected with balloon associated enteroscopy has been reported. Wolff et al.10 performed an endoscopic resection of an ileal inflammatory fibroid polyp with a single balloon enteroscope in a patient who suffered from obscure GI bleeding.
With the development of new endoscopic devices, selected small bowel lesions that would previously have been diagnosed and treated by surgery can be detected and treated with balloon-assisted enteroscopy.9 For some small bowel lesions that are detected on other diagnostic modalities such as abdominal CT scans, preoperative evaluation with balloon assisted enteroscopy is worthwhile before surgical treatment, and may be helpful to prevent unnecessary surgery. Small bowel inflammatory polyps are appropriate candidates for endoscopic treatment with balloon assisted enteroscopy.