INTRODUCTION
Endoscopists have sought methods enabling painless endoscopy to increase checkup and follow-up rates for detecting diseases at an early stage. Sedation is a useful option to realize this goal as long as safety is not compromised. Safety includes not only periprocedural acute responses but also delayed events that may occur after the examinees leave the hospital following outpatient-based examinations.
Benzodiazepine (Bz) drugs have been commonly used for sedation worldwide [1]. Although Bzs can be safely used owing to their relatively mild profiles and considerable use experience, a few concerns remain, including oversedation and long-lasting effects. Oversedation causes respiratory suppression, cardiovascular reaction, and prolonged recovery time. The long duration of the drug effects necessitates prolonged care and, thus, recovery beds. Moreover, residual effects such as drowsiness, impaired judgement, and physical instability might cause dangerous accidents.
Propofol has been considered an ideal alternative because of its extremely rapid drug kinetics, reported by several previous publications confirming its clinical favorability [1-6]. However, its safety has not been fully established for outpatient use because the safety of recipients after they have left the hospital has not been studied. The safety of sedatives should be verified in relation to an examineeтs behavior outside the hospital to validate their general use in common practice. Therefore, we conducted a prospective study to evaluate the safety of propofol by using a questionnaire to which examinees replied 24 hours after endoscopy.
MATERIALS AND METHODS
Participant enrollment
All examinees who received propofol sedation for outpatient-based endoscopic examination, including esophagogastroduodenoscopy (EGD), endoscopic ultrasonography (EUS), and total colonoscopy (TCS), between November 2016 and March 2018 were recruited for this study. The decision to be sedated using propofol was made by the examinee voluntarily. Before obtaining informed consent for propofol use, the characteristics of propofol and Bzs (diazepam and midazolam) were impartially explained without a physicianтs recommendation or arbitrariness for propofol use if no medical reasons exist to recommend it. Propofol was not recommended for examinees with the following conditions: (1) age <18 years; (2) pregnancy; (3) moderate or severe comorbidity of cardiopulmonary, renal, or liver function; (4) allergy or intolerance to propofol, chicken egg, soy, or coconut; and (5) no written informed consent for endoscopy and propofol use.
The exclusion criteria for study enrollment were as follows: (1) previous participation in the study, (2) endoscopy as a treatment intervention, (3) inability to respond and send a questionnaire, and (4) no written informed consent for participation in the study.
This prospective observational single-arm study was conducted at Sendai City Medical Center after approval by the institutional review board of Sendai City Medical Center.
Procedures and monitoring
A venous route was established using an indwelling catheter for all the examinees who requested for propofol sedation. Oxygen saturation levels and heart rates were monitored using a pulse oxymeter before, during, and after the procedure until full recovery of wakeful consciousness. Blood pressure was measured before the procedure and when needed during the procedure.
For EGD and EUS, 80 mg of lidocaine was sprayed (10 pushes of 8% lidocaine) into the throat before sedation. For TCS, the examinees took 10 mL of 0.75% sodium picosulfate the night before and 2,000 mL of enterolavage liquid with polyethylene glycol the morning before the procedure. Immediately before inserting the colonoscope, 5 mg of scopolamine butylbromide was intravenously administered.
Propofol was administered by an assisting nurse under the direction of an endoscopist who was experienced in sedation. An anesthesiologist was always present in the hospital during the examinations performed in this study. The initial amount of propofol administration was 60 mg for examinees aged <60 years, 40 mg for those aged between 60 and 79 years, and 20 mg for those aged тЅ80 years. The initial amount was reduced at the endoscopistтs discretion on the basis of comorbidity. When the sedation depth was insufficient, 10т20 mg of propofol was added if cardiopulmonary suppression was not problematic. The maximal dose was defined to be 200 mg. Diazepam, midazolam, and pentazocine were used in combination when propofol alone was insufficient.
When adverse events occurred owing to the endoscopic procedures or sedatives, the endoscopist took appropriate actions, including oxygen administration, drug administration, and/or cessation of endoscopy. For a persistently low level of oxygen saturation (<89%), oxygen was administered.
For patients who underwent examinations under coverage by the Japanese national insurance system, the fee for propofol use was similarly covered under approval by the regional Bureau of Health and Welfare. When examinees had to bear the cost of the check-up, the costs for propofol sedation were covered by our institution.
After the endoscopic examination, the examinees were required to lie on a bed in a recovery room for at least 30 minutes. When a Bz drug or pentazocine was administered in combination, the examinees were confined for an additional 30 minutes. After the mandatory rest time, a nurse checked if the examinee could (1) clearly respond to the nurse and (2) stably walk, and (3) had a тЅ94% oxygen saturation level. When all three conditions were satisfied, the examinee was permitted to leave the recovery room. In cases where the examinee was unstable on their feet or had a low oxygen saturation level before sedation, a physician judged if the drug reaction had sufficiently diminished. Otherwise, the examinee was required to rest until they fully recovered. Driving after the examination with sedation was prohibited on the day of the examination, although this is not illegal in Japan.
Evaluated outcomes
An attending nurse in the examination room and a nurse in the recovery room recorded the kinds and amounts of administered drugs, adverse events, and necessity for oxygen administration. A questionnaire was handed to the examinee after recovery. It was filled out тЅ24 hours after the examination and posted with the examineeтs written consent. The questions were as follows:
-
(1) Until when did you feel drowsiness, sleepiness, or physical instability among the following options?
a. Before hospital dischargeb. Until early evening (around sunset) on the same dayc. Until nighttime on the same dayd.Until the next morninge. Not sure (2) Did any accident occur because of impaired judgment caused by the effects of the drug?
(3) Did you feel any symptoms other than drowsiness, sleepiness, and physical instability?
-
(4) Do you hope to receive propofol sedation in future endoscopic examinations?
a. Yesb. Yes, but I desire deeper sedationc. No, I desire another kind of sedatived.No, I desire to receive endoscopy without sedatione. Not sure
For evaluating factors related to outcomes, statistical calculations were conducted using the Fisher exact test or t-test if necessary.
Ethical considerations
Propofol use and this prospective investigation were approved by the institutional review board of Sendai City Medical Center (approval No. 20160027). This prospective study was registered in the University Hospital Medical Information Network (UMIN; issued ID No. UMIN000040330). As mentioned earlier, written informed consent for all the endoscopic examinations, sedation, propofol use, and participation in this study was obtained from all the participants.
RESULTS
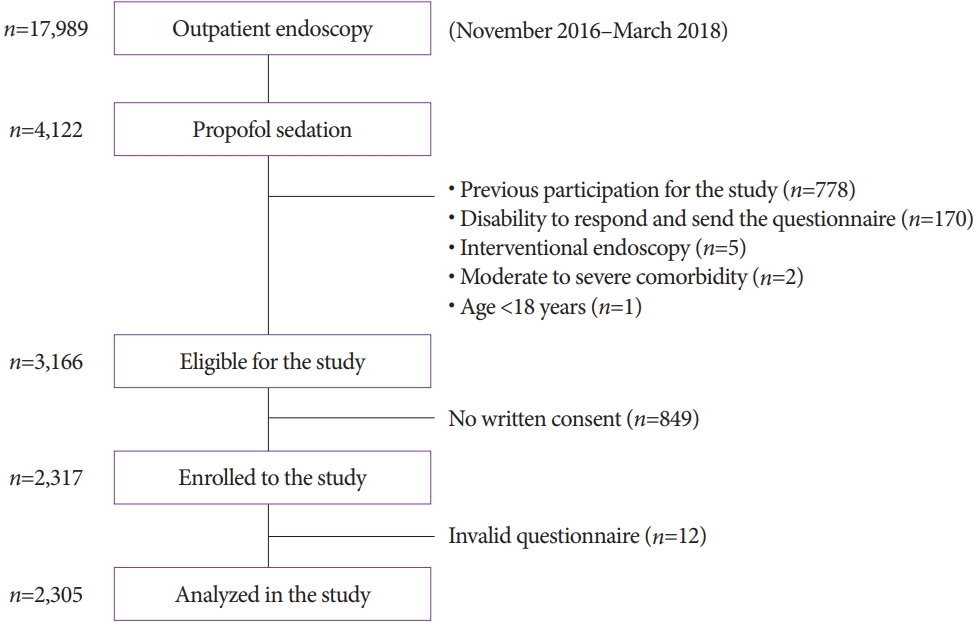
In the 17,978 outpatient-based endoscopic examinations performed between November 2016 and March 2018, 4,122 examinees underwent endoscopic examination under propofol sedation and 2,317 were eligible to participate in this study and submitted the questionnaire with their written consent (Fig. 1). After eliminating 12 examinees who submitted invalid questionnaires with incomplete signatures or unreadable answers or who posted it on the procedure date, 2,305 examinees were included in the analyses. The ages, sexes, and types of endoscopy are shown in Table 1.
The mean propofol dose was 69.6ТБ24.4 mg (range, 20т200 mg) and was combined with diazepam for 92 examinees, midazolam for 39, and/or pentazocine for 21 (Table 2). A drug combination was used more frequently for the examinees aged <70 years than for the older examinees (7.4% vs. 4.4%, p=0.005).
Mild oxygen desaturation requiring oxygen administration at a rate of 2т3 L/min occurred in 59 examinees (2.6%), although no severe respiratory suppression occurred (Table 3). Oxygen desaturation frequently occurred in (1) the examinees to whom тЅ170 mg of propofol was administered (27.3% [3/14] vs. 2.4% [56/2,291], p=0.005; Table 4), (2) elderly examinees aged тЅ70 years (4.0% [34/840] vs. 1.7% [25/1,465], p=0.001), and (3) the examinees who received a combination of sedatives as compared with those who only received propofol (10.3% [15/146] vs. 2.0% [44/2,159], p<0.001).
Two examinees developed hypotension with mild bradycardia, which required administration of intravenous atropine sulfate (0.09%), namely a 64-year-old woman who underwent EUS with 60-mg propofol and an 84-year-old man who underwent EUS with 80-mg propofol (Table 3). A 78-year-old male EGD examinee who was sedated using 40-mg propofol and had been hospitalized owing to a feeling of illness after previous EGD examinations without propofol was hospitalized because of a similar feeling. A loose tooth fell out after EGD in the case of a 78-year-old woman who was sedated using 50-mg propofol. No other severe adverse events that required medication, procedure cessation, mask ventilation, tracheal intubation, or chest compression occurred. Overall, the total rate of acute adverse events was 2.7% (63/2,305, Table 3).
From the data compiled from the submitted questionnaires, the feelings of drowsiness, sleepiness, and physical instability disappeared before hospital discharge in 86.6% of the participants, whereas in 2.7% of the participants, these feelings persisted until nighttime on the same day or the next morning (Table 5). After eliminating the examinees who answered тnot sureт or invalidly (by providing no answer or checking multiple options), the feelings disappeared prior to hospital discharge in 88.0% of the patients and by early evening in 97.3%. Serious unfavorable events, including traffic accidents, falling, incidents related to amnesia, and abnormal behavior, were not reported.
Unfavorable symptoms after hospital discharge were reported by 151 examinees (6.6%, Table 5). Miscellaneous symptoms were reported by 19 examinees (others in Question 3 in Table 5), including a feeling of illness, pyrexia (EGD with 60 mg of propofol), judgment impairment (EGD with 70 mg of propofol), head itchiness (EGD with 60 mg of propofol), pain inside the nose (EGD with 40 mg of propofol), mouth dryness (EGD with 70 mg of propofol), coughing (EGD with 60 mg of propofol), heartburn (EGD with 50 mg of propofol), hand numbness (EGD with 40 mg of propofol), leg cramps (EGD with 60 mg of propofol), hallucination (EUS with 120 mg of propofol), tinnitus (EUS with 70 mg of propofol), eye floater (EUS with 80 mg of propofol), subepithelial bleeding on a lip (EUS with 80 mg of propofol), body itchiness (EUS with 100 mg of propofol), lumbar pain (EUS with 100 mg of propofol), a feeling of poor intestinal peristalsis (EUS with 60 mg of propofol), flatus (EUS with 60 mg of propofol), and involuntary defecation (EUS with 70 mg of propofol). Most symptoms such as throat pain/discomfort (n=60), abdominal pain/discomfort (n=10), and pain at the puncture site of the indwelling catheter (n=3) did not seem to be directly linked to propofol use. All symptoms improved without medical intervention.
After eliminating 181 participants who answered тnot sureт or invalidly, 97.7% (2,065/2,124) of the participants desired propofol sedation in future examinations. For each examination, 97.9% (1,238/1,264) of the participants who underwent EGD, 97.3% (818/841) who underwent EUS, and 100% (19/19) who underwent TCS replied to have such a preference.
No significant differences in all the items evaluated in the questionnaire survey were found between the examinees who received and did not receive combinations of diazepam, midazolam, and/or pentazocine (Table 5).
DISCUSSION
Propofol has several advantageous profiles that are useful in sedation such as rapid induction and its extremely short half-life as compared with the traditional Bz drugs. Recipients lose consciousness immediately after injection and recover consciousness a few minutes after the last injection. This characteristic appears ideal for the usual endoscopic examinations that require only 5т10 minutes. Psychomotor recovery evaluated using driving simulators has been reported with significantly favorable outcomes in comparison with the traditional sedatives in several studies [2-7].
In a meta-analysis published in 2019, 11 randomized controlled trials involving 1,767 recipients were analyzed to compare the outcomes of propofol with those of Bzs as sedatives for endoscopy [1]. Although Bzs appear to lead to oxygen desaturation with borderline significance (p=0.06), differences in the occurrences of bradycardia and hypotension have not been reported. The pooled occurrence rates of oxygen desaturation, bradycardia, and hypotension in this meta-analysis are reported to be 9.4%, 2.8%, and 8.9%, respectively, which are higher than the rates in our study (2.6%, 0.09%, and 0.09%, respectively). Although the reason for the differences is unknown, the studies analyzed in the meta-analysis may have involved invasive procedures such as enteroscopy, endoscopic retrograde cholangiopancreatography, and endoscopic submucosal dissection. In addition, several studies have been conducted to analyze outcomes purely for TCS requiring procedure times longer than those required for EGD and EUS. These invasive or long procedures might have resulted in the use of high dosages, which are related to the occurrence of adverse events.
In their prospective study involving 10,662 EGD examinees, Horiuchi et al. reported the safety of low-dose bolus propofol, for which the maximal dose has been defined to be 120 mg, with no adverse events except for the occurrence of a mild decrease in SpO2 of 0.26% in the patients, requiring transient oxygen administration [8]. In another prospective single-arm study, they reported administering 0.24% oxygen for 2,101 TCS examinees, but reported no cardiovascular events after administering a maximal propofol dose of 200 mg [9]. The low initial dose based on the examineeтs age and a maximal dose of 200 mg seem safe to prevent acute unfavorable responses. In our study, although the oxygen desaturation rate was higher (2.6%) than that in the studies of Horiuchi et al., especially when other drugs were used in combination, no severe events were observed using a similar method [9]. Our data are obviously favorable in comparison with those obtained from most of the randomized studies with reported incidences of bradycardia (pooled rate, 2.8%; range, 0%т6.6%), hypotension (8.9%; 0%т33.8%), and oxygen desaturation (9.4%; 0%т36.8%) [1].
In the meta-analysis, patient satisfaction was significantly higher in the propofol group (p<0.001) in 6 evaluated studies involving 679 recipients in the settings of outpatient colonoscopy (2 studies from the same institution) [10,11], outpatient EUS (1 study) [12], or in-hospital advanced endoscopy such as double-balloon enteroscopy and endoscopic retrograde cholangiopancreatography (the other 3 studies) [1,13-15]. Although no prospective comparative study involving EGD has been conducted, in the single-arm study, Horiuchi et al. [8] reported that 94% of 400 outpatients who underwent EGD reported being satisfied with the sedation for EGD and 99% wished to be sedated using the same method in future procedures. Considering the results from previous studies and our data from 2,305 examinees, the satisfaction level appears to be acceptable.
None of the participants reported accidents within 24 hours in our study, although car driving was prohibited. In the studies by Horiuchi et al., examinees could drive home after hospital discharge [8,9]. Of the 400 EGD examinees who replied to the questionnaire, 92% were reported to have driven without any accidents [8]. If propofol is proven to have little effect even for relatively risky activities or if the conditions to ensure safety are clarified, propofol sedation would become a more ideal sedation method for endoscopy examinees who desire to do their usual activities during the remainder of the day.
Although our study was not designed to be a comparative study, this is the largest prospective study to have evaluated patient satisfaction for propofol sedation during outpatient endoscopy. Although 4.5% of the participants desired deeper propofol sedation, 97.7% hoped to receive propofol sedation in future examinations. Given that this survey was performed using a postal questionnaire after hospital discharge rather than face-to-face interviews, the results seem reliable.
Unfavorable symptoms were evaluated not by the medical personnel but by the examinees, resulting in several reports on symptoms that apparently had no direct relation to sedation, such as throat pain, throat discomfort, abdominal discomfort, and pain at the puncture site for the venous route. These outcomes were impartial evaluations that followed the recent common method to appraise clinical features of drugs. Although these cannot be compared with the outcomes from other examinations or other sedatives, all the symptoms were not significant, and the examinees recovered without medical interventions.
This study has some limitations. First, the design did not include comparative controls such as those who did not receive sedation and those who underwent sedation using another drug. Although randomized designs are theoretically ideal, studies randomizing the use of sedation or kinds of sedatives for screening endoscopy appear ethically difficult to conduct with a large population. Only a single-arm design seems acceptable for prospective evaluation with large population sizes. Second, adverse events were analyzed using only questionnaires without evaluation by medical personnel, resulting in possible overestimations and underestimations, as mentioned earlier. Third, owing to the nature of its prospective design, this study evaluated only participants who completely matched the criteria and provided written informed consent. Some examinees might have experienced some unfavorable events but could not submit the questionnaire due to, for example, a serious accident, although the hospital did not receive reports on accidents caused by outpatient sedation during the study period. Fourth, 6.3% of the participants received sedation using a drug combination, which included diazepam, midazolam, and/or pentazocine. Although these combinations led to the need to administer oxygen (Table 4), no differences were detected in the effect duration, accident occurrence, adverse events, and satisfaction. If the study prohibited the use of a drug combination, the outcome might have been different because a drug combination was used to sedate examinees who could not be effectively sedated using only propofol. However, this prohibition in a protocol is unethical, and a protocol excluding examinees who received a drug combination must involve selection bias. Considering the results of our study, a combination of propofol and other drugs appears to be a reasonable option.
In conclusion, propofol was found to be safe without severe adverse events and accidents for outpatient endoscopy on the basis of next-day patient self-evaluations. Given the high satisfaction level, sedation with propofol might be an ideal tool for painless endoscopic screening.