INTRODUCTION
Endoscopic ultrasound (EUS) and EUS-guided fine-needle aspiration (EUS-FNA) have valid diagnostic and therapeutic roles in gastrointestinal and extra-gastrointestinal lesions.1-4 However, tissue acquisition in patients with a surgically altered anatomy (SAA), including those who had undergone Billroth II gastric surgery and Roux-en-Y gastric bypass, is challenging.5 Oblique-view EUS (OV-EUS) is technically difficult and risky in these patients because of the distorted anatomy and long passage in which the small bowel and target lesions are not accessible.
Forward-view EUS (FV-EUS) has many advantages over OV-EUS. One crucial advantage is that it allows the use of needles and other devices in the straight direction, providing high penetration force into the target lesions.6-8 In this study, we report the efficacy and safety of FV-EUS in performing EUS-FNA guided by fluoroscopic imaging in patients with a SAA of the upper gastrointestinal tract.
METHODS
Study population
We retrospectively investigated 32 patients treated at the Gastroenterology Department, Aichi Cancer Center Hospital, Nagoya, Japan, between January 2014 and December 2020. First, EUS-FNA was performed to obtain evidence from patients with suspected cancer recurrence during the follow-up based on the findings of imaging examinations, including abdominal computed tomography (CT), positron emission tomography/CT, and magnetic resonance imaging. Second, EUS-FNA was performed to obtain evidence before cancer chemotherapy and in cases in which imaging was not conclusive. EUS-FNA using FV-EUS was performed under fluoroscopic guidance in all cases. All patients had mass lesions, swollen lymph nodes, or peritoneal dissemination.
All patients had undergone upper gastrointestinal surgery, either pancreaticoduodenectomy (PD), PD+left lobe hepatectomy (left HPD) total pancreatectomy, total gastrectomy, or both esophagectomy and total gastrectomy.
EUS-FNA technique
We examined all study participants using a FV-EUS scope (TGF-UC260J; Olympus Medical Systems, Tokyo, Japan), either at the outset or after the failure of OV-EUS insertion.
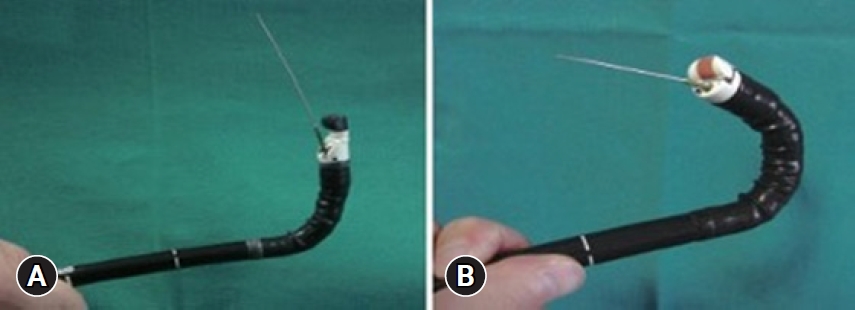
As shown in Figure 1,9 the FV-EUS scope has a straight channel, FV direction, wide bending angle, and a short distal end. These features offer advantages over OV-EUS, including providing a good puncture force and the ability to reach the puncture site smoothly. However, FV-EUS has some limitations, such as a narrow ultrasonographic scanning range (90┬░) compared with that of OV-EUS (180┬░) and the lack of an elevator.
We examined the patients after conscious sedation with intravenous pethidine and midazolam. The procedures were performed with the patients lying in the left lateral position.10,11 The FV-EUS scope was advanced via the trans-jejunum or trans-stomach depending on the type of disturbed anatomy. We used a C-arm radiographic machine to adjust and compare the scope-tip position on the fluoroscopic image to that of the target lesion on the CT image. Thereafter, we localized the target lesion to perform FNA under ultrasonographic guidance. Subsequently, the target lesion was monitored under the ultrasonographic view. Fluoroscopic imaging was also used to guide the direction of the scope tip in relation to the target lesion.
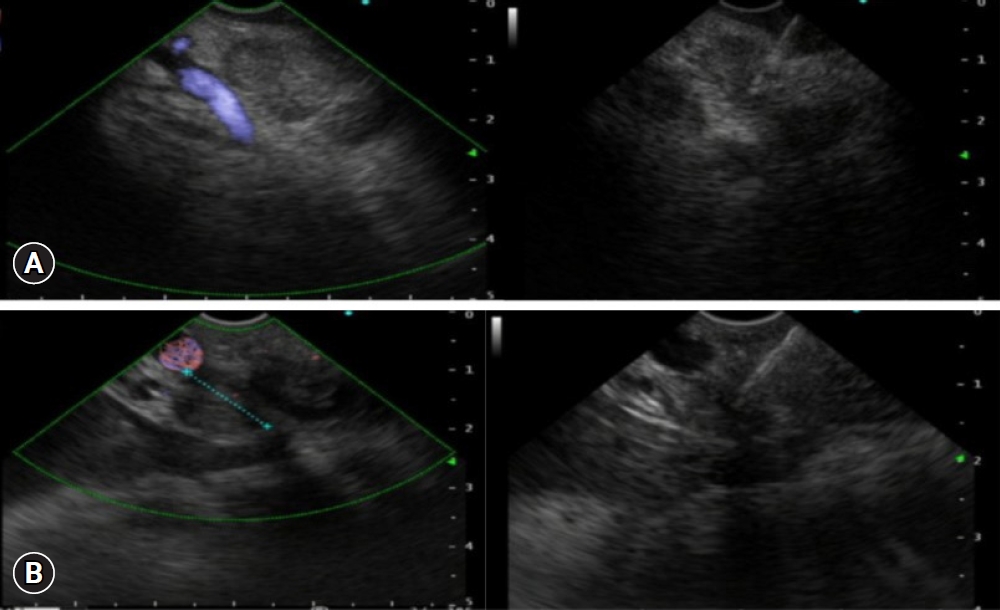
We performed FNA using a 22- to 25-gauge Expect needle (Boston Scientific) or a 22-gauge Acquire needle (Boston Scientific) and a 22-gauge Ez-Shot needle (Olympus Medical Systems). After each puncture, the specimens were sent for rapid onsite evaluation (ROSE), cytology, or tissue cell block. The number of punctures ranged from one to six, depending on the ROSE results (Fig. 2). The procedures were performed in a fluoroscopy room by expert endosonographers.
RESULTS
Of the 32 studied patients, 26 underwent EUS-FNA using FV-EUS combined with fluoroscopic guidance to evaluate for tumor recurrence suspected on the basis of abdominal CT, magnetic resonance imaging, or positron emission tomography results; five patients underwent the procedure to help the clinicians make informed decisions before chemotherapy; and one patient underwent the procedure after the failure of diagnosis by imaging.
In our study, the specificity, sensitivity, and accuracy of EUS-FNA using FV-EUS were 100%, 87.5%, and 87.8%, respectively. Of the 32 patients, four could not be evaluated with EUS-FNA because of insufficient specimens, and one patient was finally diagnosed radiologically. In this latter patient, the lesion was difficult to diagnose by FNA although the specimen was reported to be sufficient and confirmed to be nonmalignant by cell block and cytology techniques.
FV-EUS was performed for FNA under fluoroscopic guidance either at the outset (24 patients) or after the failure of OV-EUS (eight patients). FV-EUS was technically successful in all studied patients (100%).
The patients who underwent postoperative assessment with FV-EUS had a previous history of pancreatic cancer (19 patients), cholangiocarcinoma (eight patients), intraductal papillary mucinous cancer (one patient), duodenal cancer (one patient), gastric cancer (one patient), ampulla of Vater cancer (one patient), and both gastric and esophageal cancers (one patient) (Table 1).
The patients had undergone either PD (26 patients), total pancreatectomy (three patients), left HPD (one patient), total gastrectomy with Roux-en-Y reconstruction (one patient), or both esophagectomy and total gastrectomy (one patient) (Table 1).
The lesions targeted in our study included peritoneal dissemination (14 patients), lymph node swelling (nine patients), anastomotic mass (four patients), liver metastasis (two patients), mass around the celiac artery (one patient), mass around the superior mesenteric artery (one patient), and pelvic mass (one patient) (Table 2).
FNA was performed in all patients using a FV-EUS scope through the trans-jejunum route in 27 patients, from the stomach in three patients, from both the trans-jejunum and trans-stomach in one patient, and from the Y-leg anastomosis in one patient (Table 2).
The site of puncture differed according to the cases, as shown in Table 2. The median lesion diameter was 15.7 mm (range, 8ŌĆō23 mm), and the median procedural time (from scope insertion to withdrawal) in all study participants was 51 minutes (range, 18ŌĆō135 minutes). The specificity, sensitivity, and accuracy of EUS-FNA using FV-EUS was 100%, 87.5%, and 87.8%, respectively. No adverse events due to the EUS-FNA procedure were recorded (Table 3).
DISCUSSION
In this retrospective study, we evaluated the efficacy and technical success of EUS-FNA using FV-EUS in patients with a SAA. Vilmann et al.1 first described the feasibility of EUS-FNA in 1992. Since then, many studies have reported the efficacy of EUS-FNA in sampling gastrointestinal and perigastrointestinal lesions.12,13 Using the conventional OV-EUS for tissue sampling from gastrointestinal lesions in patients with a SAA is challenging because of equipment limitations. Advancing the OV-EUS scope through the distorted anatomy of the small bowel is difficult. In addition, the angulation of the tip is limited because of the relatively long transducer at the scope tip.14
To overcome these limitations, we attempted FV-EUS guided by fluoroscopic imaging in performing EUS-FNA in patients with suspected recurrent tumors, either as a first-line procedure in 24 patients (75%) or after a failed EUS-FNA using OV-EUS in eight patients (25%). FV-EUS has some advantages over OV-EUS. First, owing to its FV orientation, the FV-EUS scope could be easily advanced into the surgically altered small bowel (Fig. 3). Second, it has a higher degree of tip angulation than the OV-EUS scope.
To our knowledge, only three studies have reported the feasibility of EUS-FNA in patients with a SAA. First, Wilson et al.15 retrospectively evaluated patients with a SAA who underwent EUS screening and EUS-FNA using OV-EUS. Among 39 patients who had undergone Billroth II reconstruction, the pancreatic head and distal bile duct could not be visualized in 10 patients because of difficult scope intubation to the afferent loop. In addition, among 37 patients indicated for FNA, puncture was not possible with OV-EUS in seven patients because the suspected lesions could not be visualized, the target area could not be reached, or intervening blood vessels could not be avoided. Second, Tanaka et al.16 investigated the feasibility of EUS-FNA using OV-EUS in patients with a SAA. In patients with a history of total gastrectomy and double-tract reconstruction, the OV-EUS scope could not be advanced through the jejunal limb. They needed to change the scope to a single-balloon enteroscope and used a nasobiliary catheter to guide the OV-EUS scope in reaching the duodenum under fluoroscopic guidance. However, in patients with Roux-en-Y reconstruction, they could not insert the OV-EUS scope through the jejunal limb even with the use of nasobiliary catheter guidance. They eventually had to change to FV-EUS. This procedure seems riskier, more time-consuming, and requires more resources than using FV-EUS as the first-line technique. Third, Fusaroli et al.17 also examined the performance of FV-EUS for pancreaticobiliary examination in patients with a SAA. They demonstrated the effectiveness of FV-EUS as a screening method and that of EUS-FNA in obtaining samples in patients with a history of Billroth II gastric surgery. However, they reported some limitations in patients with Roux-en-Y reconstruction, probably owing to the defective flexibility of the FV-EUS scope and the variable limb length.
FV-EUS scanning and tissue sampling vary according to the type of patients and whether they have a residual stomach or have undergone subtotal or total gastrectomy. Before FNA in patients with a SAA, we carefully assessed the altered anatomy to determine how to reach the target lesion. In our study, the FV-EUS scope passed smoothly through the jejunal limb and was easier to insert into the afferent loop in 27 patients, into the stomach in three patients, from both the trans-jejunum and trans-stomach in one patient, and from the Y-leg in one patient.
Our team previously examined the efficacy of FNA using FV-EUS in tissue acquisition from pericolonic lesions under fluoroscopic guidance. We reported that the specificity, sensitivity, and accuracy of EUS-FNA for detecting malignant lesions were 100%, 91%, and 92%, respectively.18 Our current study found that EUS-FNA using FV-EUS was efficient in differentiating malignant from benign lesions, with the sensitivity, specificity, and accuracy of 87.5%, 100%, and 87.8%, respectively.
In four of the 32 patients, FNA using FV-EUS failed to obtain sufficient samples (one patient with a history of total pancreatectomy and three patients with a history of PD), which could be attributed to low tumor cellularity after chemotherapy (Table 4). This finding is in agreement with the result of a previous multicenter study from Europe that reported that the technical success in patients with a SAA was significantly lower than that in patients with a normal anatomy.19
Our study had some limitations. First, it was based on a retrospective review of a single-center experience. Second, the equipment limitation of FV-EUS is its narrow scanning range (90┬░) compared with that of OV-EUS (180┬░). To overcome this limitation, we used fluoroscopy to help localize the target lesions by approaching the scope tip closer to the target lesions previously detected with CT. In addition, we used a detachable cap (endoscopic distal attachment cap; Olympus Medical Systems) over the scope tip to hold the scope in place and for effective air suction to obtain a clearer ultrasound image (Fig. 4).
In conclusion, FV-EUS is safe and effective for performing EUS-FNA in patients with a SAA of the upper gastrointestinal tract.