INTRODUCTION
Gastric cancer is reported to have the fourth highest mortality rate in the world.1 The stage of gastric cancer at diagnosis is often advanced, except in Japan and Korea. Therefore, the overall 5-year survival rate is <10%.1 However, the prognosis improves in patients diagnosed at an early stage.2 In addition, endoscopic treatment of early gastric cancer (EGC) ensures a patientŌĆÖs quality of life.3 Hence, early diagnosis of gastric cancer is imperative. Although esophagogastroduodenoscopy (EGD) is useful for detecting EGC,4 endoscopists have difficulty learning the ŌĆ£technique,ŌĆØ gaining ŌĆ£knowledge,ŌĆØ and ŌĆ£obtaining experience.ŌĆØ These three topics are essential to enable endoscopists to detect EGC using EGD.5 To address these difficulties, we developed three types of web-based e-learning systems, tested each through randomized controlled trials (RCTs), and demonstrated their usefulness in ensuring correct and precise endoscopic diagnosis of EGC.5-7 In this review, we introduce the basic diagnostic systems employed in e-learning, the outcomes of RCTs testing the usefulness of these three e-learning systems, and our future projects.
THE PRINCIPLES FOR DEVELOPING E-LEARNING SYSTEMS FOR THE ENDOSCOPIC ASSESSMENT OF EGC
The core principles of the e-learning system are that endoscopists should acquire ŌĆ£technique,ŌĆØ ŌĆ£knowledge,ŌĆØ and ŌĆ£experienceŌĆØ for the endoscopic diagnosis of EGC.8 Therefore, we constructed the contents for all e-learning systems imparting ŌĆ£technique,ŌĆØ ŌĆ£knowledge,ŌĆØ and ŌĆ£experience.ŌĆØ
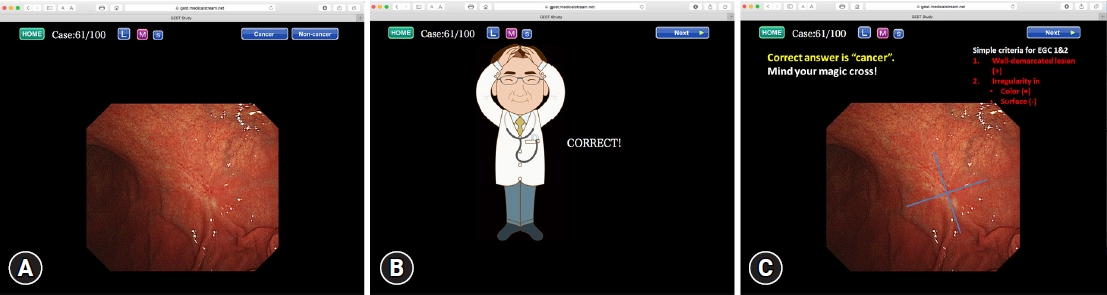
To teach ŌĆ£techniqueŌĆØ and ŌĆ£knowledge,ŌĆØ we employed video lectures. The alternative, ŌĆ£acquiring experienceŌĆØ by e-learning, is challenging. Therefore, we speculated that repeated self-study with 100 consecutive cases (100 cases of repeated self-study) could be useful for accumulating experience similar to that employed in machine learning (Fig. 1).5
BASIC DIAGNOSTIC SYSTEMS AND THEIR PERFORMANCE IN ŌĆ£DETECTION,ŌĆØ ŌĆ£CHARACTERIZATION,ŌĆØ AND ŌĆ£PREOPERATIVE ASSESSMENTŌĆØ EMPLOYED IN THE E-LEARNING SYSTEMS
Detection using conventional white-light imaging
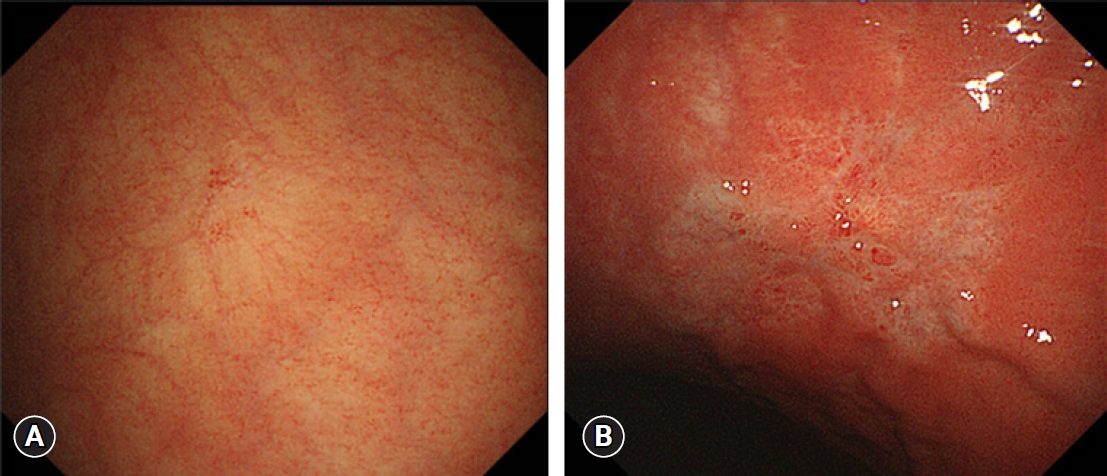
We constructed a color plus surface classification system (CSCS) to characterize mucosal lesions detected using conventional white-light imaging (C-WLI) alone.4,9 The criteria according to the CSCS were as follows: (1) presence of a well-demarcated lesion with irregularity in color, and (2) presence of a well-demarcated lesion with an irregular surface. If the target met either criterion, the diagnosis was ŌĆ£cancerous.ŌĆØ When both were absent, the diagnosis was ŌĆ£noncancerousŌĆØ (Fig. 2).8
We reported that when we applied these criteria to clinical practice, the sensitivity was 81.0%, and the specificity was 88.1%.10 This diagnostic system can help endoscopists improve their skills in the early detection of EGC.
Characterization using magnifying endoscopy with narrow-band imaging
We established a vessel plus surface classification system (VSCS) (Fig. 3),11 which has already proven helpful in the accurate assessment of EGC12,13 and in delineating EGCs for curative endoscopic resection.14 The VSCS has been approved through a multi-society consensus as a standardized magnifying endoscopy diagnostic system.15 The criteria were as follows: (1) Presence of an irregular microvascular (MV) pattern with a demarcation line. (2) Presence of an irregular microsurface (MS) pattern with a demarcation line. If the target lesion met either or both criteria, the diagnosis of the lesion was ŌĆ£cancerous.ŌĆØ If both criteria were absent, the diagnosis was ŌĆ£noncancerous.ŌĆØ
We report the diagnostic performance of magnifying endoscopy with narrow-band imaging (M-NBI) with a high-confidence prediction according to the VSCS. The sensitivity was 85.7%, and the specificity was 99.4%.12 The case determined to be a false-negative was a signet-ring cell carcinoma that was pale in color and did not represent either an irregular MV pattern or an irregular MS pattern without a demarcation line. When we excluded the false-negative case that showed a pale superficial mucosal lesion, the sensitivity increased from 85.7% to 100%.12 Hence, when the VSCS is used for diagnosis using M-NBI, M-NBI is deemed an optical biopsy.
Preoperative assessment to select the optimal therapeutic strategy for EGC (endoscopic vs. surgical resection) for predicting submucosal cancer
To determine the indications for endoscopic resection, we need to assess the (1) histological findings (differentiated vs. undifferentiated type), (2) size, (3) depth of invasion (mucosal vs. submucosal invasion), and (4) presence or absence of an ulcer.16
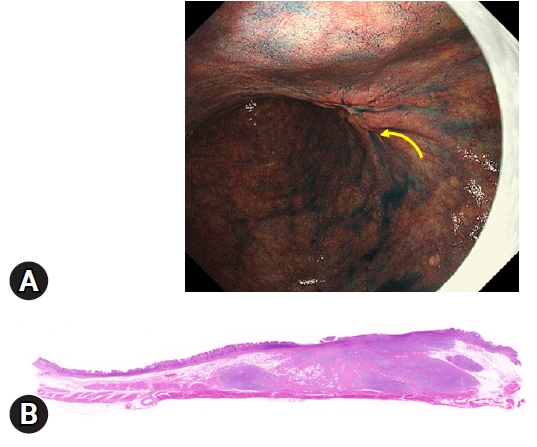
We focused on the endoscopic diagnosis of the depth of invasion by chromoendoscopy, referring to ŌĆ£the non-extension signŌĆØ (NES).17 The NES is a phenomenon characterized by focal thickness and rigidity of the submucosal layer caused by massive submucosal invasion of cancerous tissue. When endoscopic air is insufflated and the stomach is distended, the form of extension differs depending on the depth of the cancer. For example, T1a-T1b1 cancers and noncancerous mucosa are well extended and flattened. However, two distinct patterns are found in the case of T1b2 cancer. (1) The T1b2 submucosal invasive cancer is not flattened and is poorly extended, forming a trapezoid elevation (Fig. 4). (2) The tips of the mucosal folds, which converge onto the trapezoid elevation, become elevated (Fig. 4). If the endoscopic findings show both or either of these findings, the lesion is determined to be NES-positive. If both findings are negative, it is assessed as NES-negative. The sensitivity of NES for predicting a T1b2 cancer was 92.0% (95% confidence interval [CI], 87.0%ŌĆō97.0%), and the specificity was 97.7% (95% CI 96.7%-98.8%).17
OUTCOMES OF RCTS TESTING THE USEFULNESS OF THE E-LEARNING SYSTEMS
The first e-learning system: ŌĆ£detectionŌĆØ
In the first step, mucosal lesions suspicious for EGC should be detected using C-WLI, which is commonly available worldwide. Accordingly, the first e-learning system was designed to enable endoscopists to increase the detection of EGC using C-WLI alone.5 The principles and details of this e-learning system are comprehensively reported elsewhere.8
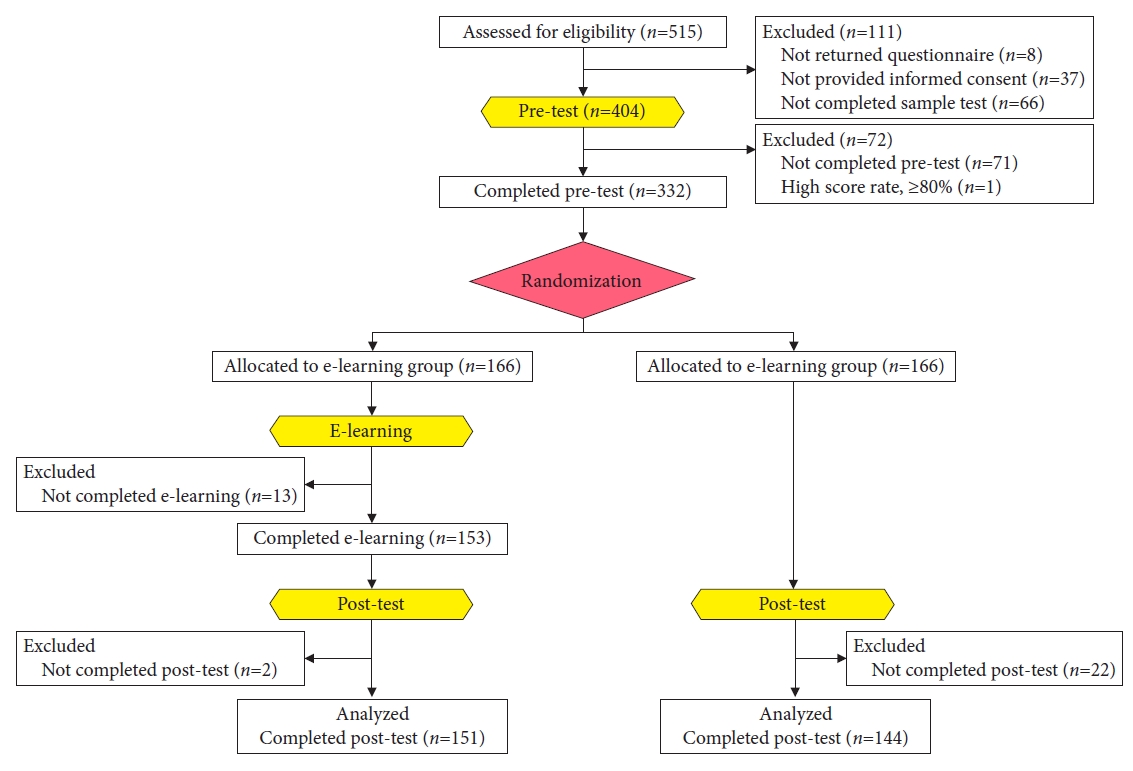
In this study, participants took a pretest and were randomly assigned to either the e-learning group (ELG) or non-e-learning group (NELG). Only the participants assigned to the ELG could perform e-learning. After 2 months, both groups underwent a posttest. Eligibility was determined by 515 endoscopists from 35 countries, and 332 endoscopists were enrolled in the trial. We then randomly assigned 166 participants to either the ELG or NELG. Finally, we analyzed the data obtained from 151 participants who completed e-learning (ELG) and 144 (NELG) who did not have access to e-learning (Fig. 5). The mean improvement rate┬▒standard deviation in the ELG was 1.24┬▒0.26, which was significantly higher than that of the NELG (1.00┬▒0.16) (p<0.001, unpaired t-test) (Table 1).5 Regarding the other analysis, the scores of the ELG were better than those of the NELG, which means that the e-learning system was beneficial regardless of the pretest rating, participantsŌĆÖ expertise, or geographical origin (Table 1).5
The second e-learning system: characterization
After detecting a suspicious mucosal lesion by C-WLI, the next process should be ŌĆ£characterization.ŌĆØ M-NBI helps differentiate between cancerous and noncancerous lesions12,13 and reduces the number of biopsies.12
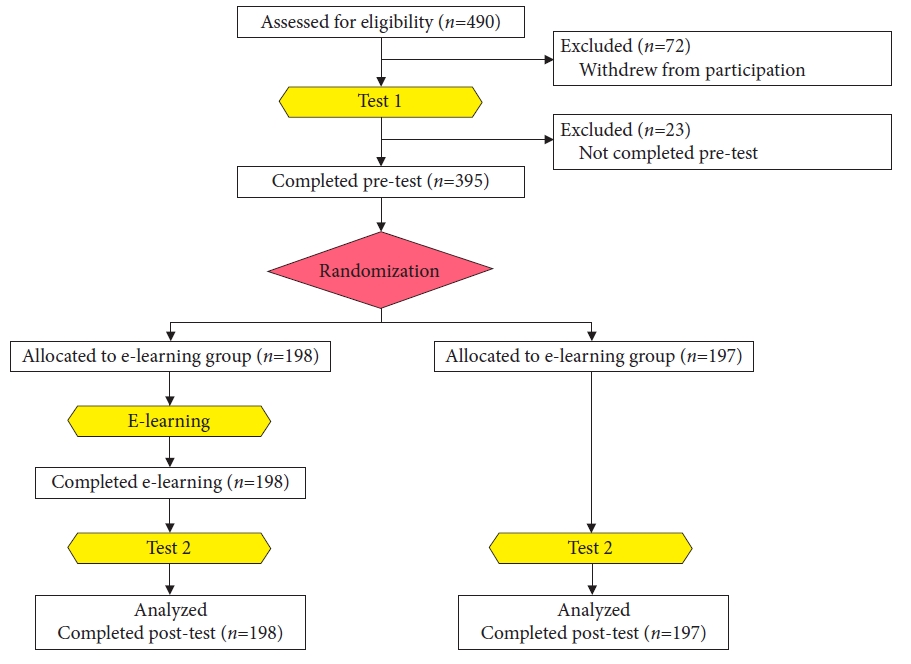
Although VSCS is simple, endoscopists require substantial effort to acquire ŌĆ£technique,ŌĆØ ŌĆ£knowledge,ŌĆØ and ŌĆ£experienceŌĆØ to be accustomed to this system. Because no systematic learning system has proven its usefulness through a well-designed clinical trial, we developed an e-learning system for EGC diagnosis using M-NBI and tested its efficacy using an RCT. Endoscopists from all over Japan participated in this study. After the participants received test 1, they were randomly allocated to either the ELG or NELG. The ELG could learn the M-NBI diagnosis through the e-learning system. After the ELG finished e-learning, both the ELG and NELG took test 2.
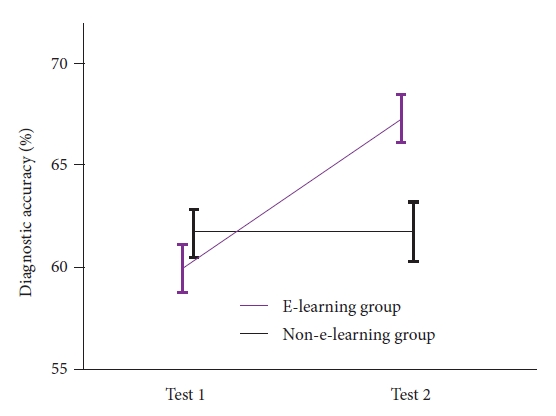
A total of 395 endoscopists from 77 facilities who completed test 1 were randomly assigned to the ELG (n=198) or NELG (n=197) (Fig. 6). The change in the score in test 2 of the ELG was 7.4 points, which was significantly higher than that (0.14 points) of the NELG (p<0.001, unpaired t-test) (Fig. 7).6 This trial demonstrated the usefulness of this second e-learning system for improving the diagnosis of EGC by M-NBI.
The third e-learning system: ŌĆ£preoperative diagnosis
After completing two e-learning systems for ŌĆ£detectionŌĆØ and ŌĆ£characterization,ŌĆØ we were confident that acquiring ŌĆ£technique,ŌĆØ ŌĆ£knowledge,ŌĆØ and ŌĆ£experienceŌĆØ is beneficial to endoscopists to improve the diagnosis of EGC. Teaching ŌĆ£techniqueŌĆØ and ŌĆ£knowledgeŌĆØ by giving lectures using recorded video clips in an e-learning context is not so difficult. However, the ŌĆ£accumulation of experienceŌĆØ is difficult for every endoscopist. The experience of endoscopists in hospitals with few cases is limited. We assumed that for predicting submucosal EGC according to endoscopic findings, ŌĆ£experienceŌĆØ is essential for acquiring the diagnostic ability in addition to learning ŌĆ£the techniqueŌĆØ and gaining ŌĆ£the knowledge.ŌĆØ
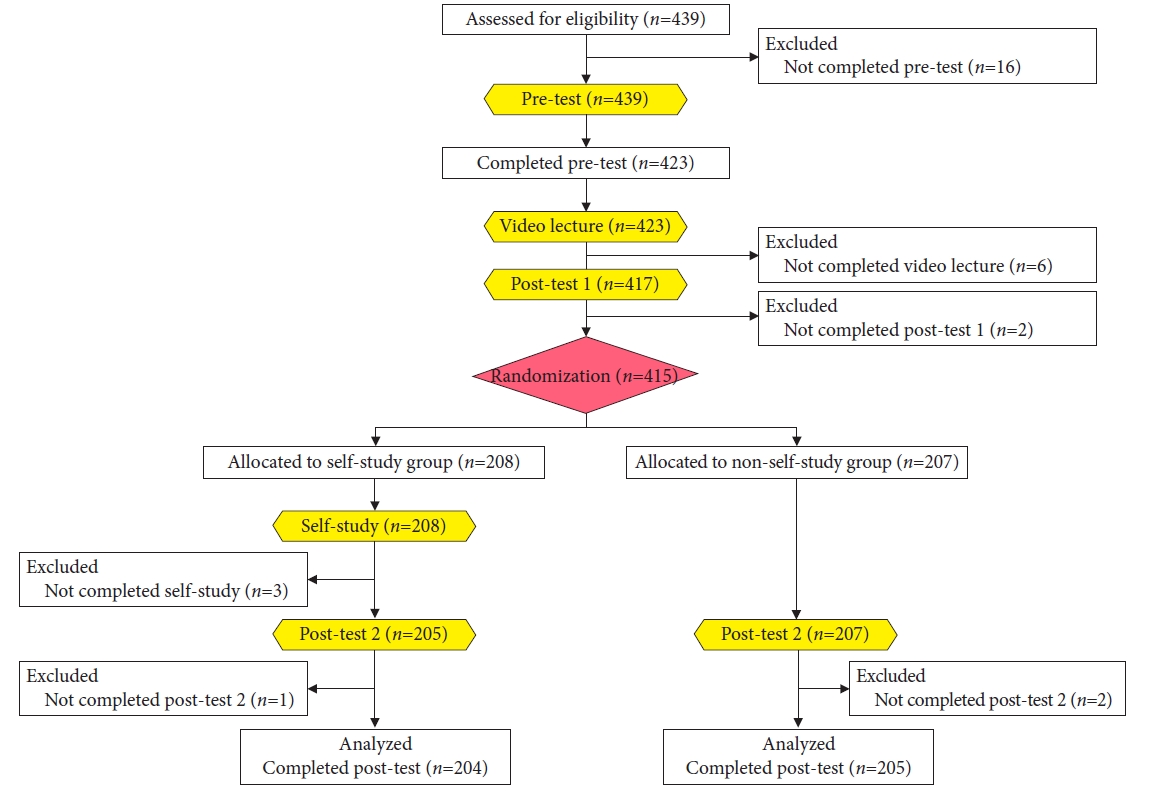
Accordingly, in contrast to the two previous RCTs, the purpose of the third study was to investigate whether this ŌĆ£accumulation of experienceŌĆØ is independently affected in improving the ability of the endoscopist to predict submucosal EGC.7 We carried out an RCT that included 423 endoscopists from 93 institutions all over Japan. After the participants took a pretest, they learned the ŌĆ£techniqueŌĆØ and ŌĆ£knowledgeŌĆØ by watching recorded videos and the received posttest 1. After posttest 1, we randomly assigned the participants to either the self-study group (SSG) or non-self-study group (NSSG). Only participants in the SSG could log on to the self-study training system, where they practiced 100 case quizzes. After completing the self-study, participants in the SSG and NSSG received posttest 2. The primary endpoint was the difference in the mean scores of posttest 2 between the SSG and NSSG. The maximum score was 100.
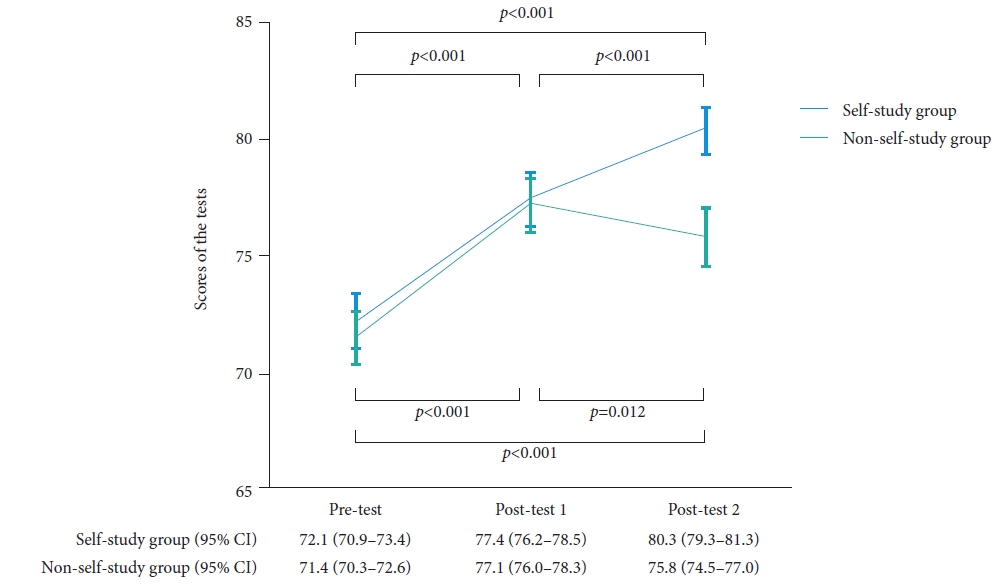
A total of 423 endoscopists who completed the pretest were included in the study. Of these, 415 completed posttest 1 and were randomly allocated to either the SSG (n=208) or NSSG (n=207). Finally, 204 participants from the SSG and 205 from the NSSG were analyzed (Fig. 8). After watching the lecture videos, the mean score increased from 72 points on the pretest to 77 points on posttest 1. The posttest 2 score of the SSG participants was 80 points, which was significantly higher than that (76 points) of the NSSG participants (p<0.001, unpaired t-test) (Fig. 9).7
The third study showed that the ŌĆ£accumulation of experience,ŌĆØ achieved by repeated practice using the 100-case self-study training, consolidated the learning ŌĆ£techniqueŌĆØ and ŌĆ£knowledgeŌĆØ and increased the diagnostic ability of endoscopists of EGC.
DISCUSSION AND FUTURE PLANS
In this article, we introduced three web-based e-learning systems to teach the endoscopic diagnosis of EGC, focusing on ŌĆ£detection,ŌĆØ ŌĆ£characterization,ŌĆØ and ŌĆ£preoperative diagnosis.ŌĆØ We clearly demonstrated that these three e-learning systems are useful as shown by RCTs. Before introducing an e-learning system, we also demonstrated a basic diagnostic system and evidence for each system because an e-learning system should be constructed with concrete diagnostic procedures proven useful in well-designed clinical trials.
The e-learning included three components: ŌĆ£technique,ŌĆØ ŌĆ£knowledge,ŌĆØ and ŌĆ£experience.ŌĆØ The endoscopist can learn ŌĆ£techniqueŌĆØ and ŌĆ£knowledgeŌĆØ by viewing lecture videos; however, it is difficult for the endoscopist to acquire ŌĆ£experience.ŌĆØ Accordingly, we developed a 100-case self-training program. The efficacies of the first and second e-learning systems were assessed after participants, who were allocated to the ELG, studied ŌĆ£technique,ŌĆØ ŌĆ£knowledge,ŌĆØ and ŌĆ£experienceŌĆØ altogether. The third e-learning system trial was designed differently from the previous trials because we speculated that 100-case self-training could increase the learning effect. Accordingly, we randomized the participants after completing the video lectures to independently assess the efficacy of the 100-case self-training program. Interestingly, the video lectures significantly improved the test scores; however, this learning effect did not last long without experience. The participants who completed the 100-case self-training program showed significantly greater improvement in the test scores. These results indicated that acquiring ŌĆ£techniqueŌĆØ and ŌĆ£knowledgeŌĆØ is not enough to achieve improved diagnostic ability and that accumulating ŌĆ£experienceŌĆØ is mandatory.18
Conventional instruction, such as teaching in clinical practice by a senior endoscopist, hands-on training using models or patients, attending lectures, and reading papers or books, is useful for imparting ŌĆ£knowledgeŌĆØ and ŌĆ£technique.ŌĆØ However, the number of learners is limited, and these forms of instruction cannot provide an accumulation of ŌĆ£experience.ŌĆØ As described previously, e-learning offers several advantages over conventional instruction. It can provide ŌĆ£techniqueŌĆØ and ŌĆ£knowledgeŌĆØ by watching video clips that are easy for endoscopists to understand, and repeated training programs can be helpful for endoscopists to accumulate ŌĆ£experience,ŌĆØ which is similar to machine learning. Moreover, the number of learners is not limited, and they can access e-learning whenever and wherever they prefer.
One of the limitations of these trials is that outcome measurement was carried out using test scores on the Internet. We have not yet assessed the improvements in clinical practice after e-learning. We aimed to plan clinical trials to assess the improvement in endoscopic diagnosis in clinical practice after participants completed e-learning.
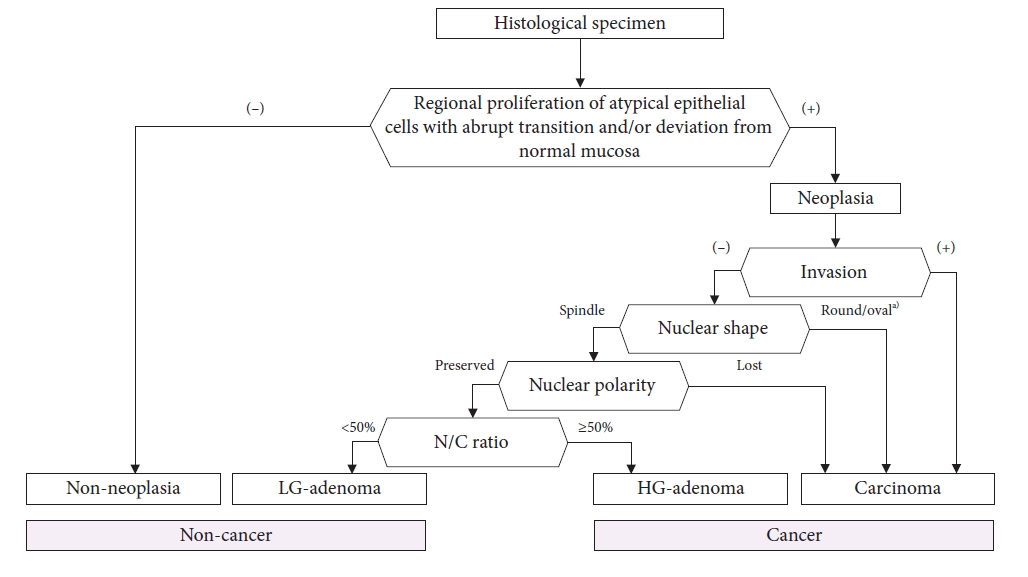
We will consider investigating the efficacy of an e-learning system to improve the histopathological diagnosis of EGC, as this is the gold standard for endoscopic diagnosis. As previously mentioned, a diagnostic system should first be constructed. To date, no standardized diagnostic systems have been established. We developed a comprehensive algorithm for making a histological diagnosis of gastric cancer (Fig. 10). We tested whether the algorithm can function as a standard diagnostic system for e-learning content. In the near future, we will initiate the RCT by inviting international pathologists (UMIN000044545). If this trial is successfully completed, our series of e-learning systems for improving the endoscopic and histopathological diagnosis of EGC can be finalized.