In the mid-90s, endoscopists from Japan developed the technique of performing mucosal incisions around lesions for complex endoscopic mucosal resections (EMRs). Later, in the early 2000s, the concept of mucosal incisions associated with endoscopic submucosal dissection (ESD) was developed.1 Concomitantly, Gotoda et al.2 discovered that T1 cancer subgroups have distinct prognoses. Superficial cancers showed a near-zero risk of metastasis and could be safely managed by endoscopic resection. This scenario set forth a paradigm shift toward ESD treatment for early gastrointestinal cancer.1,2
Since then, a wide range of accessories have been developed and the ESD strategy has been refined. Resections have evolved from those of superficial gastric cancers to the removal of esophageal and colonic lesions.3,4 The technical aspects of colorectal ESD are especially challenging, as endoscopic maneuverability may be poor, imposing a longer procedure time with a higher risk of adverse events.5 An effective and safe alternative for overcoming some of these barriers is combined snare resection after partial submucosal dissection, known as hybrid ESD (H-ESD). However, the limited data on H-ESD renders its comparison with conventional ESD (C-ESD) difficult (Fig. 1).6
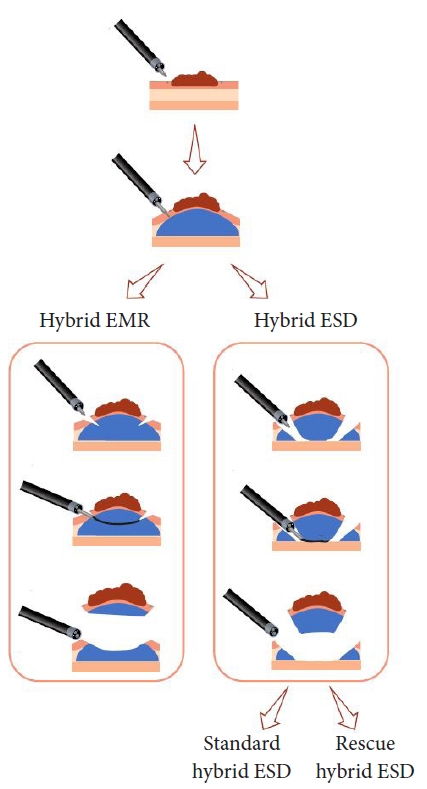
Hybrid endoscopic resections can be perfomed in different ways. Specific terminologies have been previously described and must be used to distinguish the various forms of this approach. When snaring is performed after circumferential mucosal incision of the lesion and without proper trimming and dissection of the submucosal layer, the procedure is known as precut EMR. H-ESD is defined as the technique in which the submucosal layer is consistently dissected and snared after the partial ESD procedure.7
In their study of 137 lesions, Okamoto et al.8 identified a pool of 27 for which planned ESD was switched to a hybrid technique owing to procedural challenges, with the approach classified as rescue treatment. Although the procedures were shorter in the rescue group, the en bloc resection rate dropped significantly from 94.2% to 66.7%.
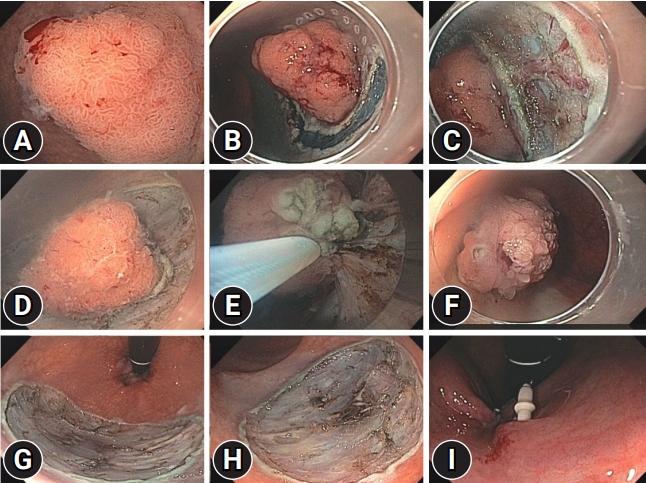
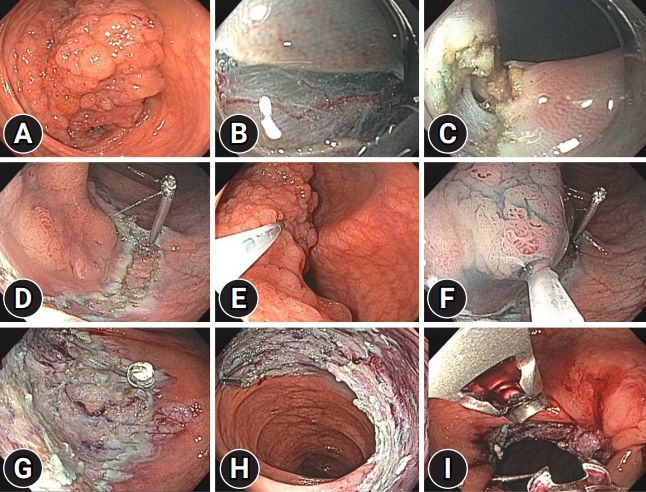
Whether the hybrid approach was planned in advance (Fig. 2) or performed as a rescue therapy appears to be relevant (Fig. 3). However, this information is not stratified in most published data, thus probably interfering negatively with the overall en bloc resection rate of standard H-ESD. Preserved margins are of paramount importance, as they enable a precise histological diagnosis. Additionally, it is well known that the recurrence risk with en bloc resection is significantly lower than that with piecemeal resection (3% vs. 20%, p<0.0001).9
In consideration of this, Yamaguchi et al.10 thoroughly investigated the significance of rescue H-ESD (RH-ESD), standard H-ESD, and C-ESD in their recent article published in this issue of Clinical Endoscopy. Among the total of 364 colorectal ESD procedures, the en bloc resection rate increased significantly in the order of RH-ESD (48.6%) <H-ESD (78.3%) <C-ESD (97.7%) (p<0.001). The proper registration of whether the resection was a rescue or a previous scheduled hybrid approach was essential to better understand the real benefit of the different hybrid resection techniques. Additionally, this article confirmed that the submucosal dissection rate was significantly lower in the piecemeal resection group (25% [20%т30%]) than in the en bloc resection group (40% [20%т60%]).10
When opting for H-ESD, it is important to trim and dissect the submucosal layer as much as possible, allowing proper snaring. Closure should occur without significant distortion of the lesionтs surface. Capturing a too large portion of submucosa may deform attached layers, leading to unplanned cutting levels with a higher risk of damage to the muscularis propria or fragmentation of the lesion.6
When faced with difficult situations, such as severe fibrosis, prolonged procedure time, large perforations, massive bleeding, and unstable vital signs, endoscopists should be ready to shift from the C-ESD technique to RH-ESD for faster resolution of the procedure. Prolonged or complicated endoscopic procedures can influence the physicianтs decision-making process and focus and have a higher physiological impact on the patient. Notwithstanding the advantages, proper indication and timing have yet to be established.6,7
From a practical standpoint, RH-ESD can be used to safely avoid surgical intervention, with a lower en bloc rate than that of the conventional technique. The reported 4.2% recurrence rate can be managed by additional EMR or thermal avulsion.10
H-ESD is faster and less technically demanding than the conventional approach. It is an optimal strategy for endoscopists who are still on the learning curve of submucosal dissection. More experienced endoscopists may overlook H-ESD as a technique for novices. In our opinion, this is a conceptual mistake with an impact on the physicianтs overall success and complication rates. Understanding the strengths, weaknesses, and practical subtleties of H-ESD is paramount in decision making. Choosing the best ESD technique for each case is critical for improving outcomes.
Yamaguchi et al.10 has some key points to help understand the H-ESD techniques: (1) RH-ESD and standard H-ESD are different techniques and thus present different outcomes. (2) Sufficient submucosal dissection is required when performing RH-ESD to avoid piecemeal resection. (3) RH-ESD for difficult or complicated cases is useful for avoiding surgery in cases of unsuccessful C-ESD. (4) The incidence of local recurrence is relatively low. Nonetheless, eventual recurrence may be safely managed by means of endoscopic therapies.