INTRODUCTION
Xanthoma is an uncommon nonneoplastic lesion resulting from the accumulation of foamy histiocytes. It predominantly shows cutaneous manifestations associated with hyperlipidemia. Verruciform xanthoma (VX), which has almost similar histologic features, is also a rare lesion usually found on the oral mucosa or the genital area. It is presumably associated with the inflammatory response to mucosal damage.1 However, xanthoma and VX of the esophagus are extremely rare. Since the first report by Remmele and Engelsing2 only 13 cases of esophageal xanthoma have been reported,1,2,3,4,5,6,7,8,9 and since the report by Herrera-Goepfert et al.,10 only four cases of VX of the esophagus have been reported.10,11,12,13 The etiologies of both lesions are not understood. The authors recently encountered a new case of esophageal xanthoma. Besides its rarity, the confusing descriptions of these two lesions have made distinguishing between them difficult. We describe herein a new case, including a review of all reported cases of xanthoma and VX of the esophagus.
CASE REPORT
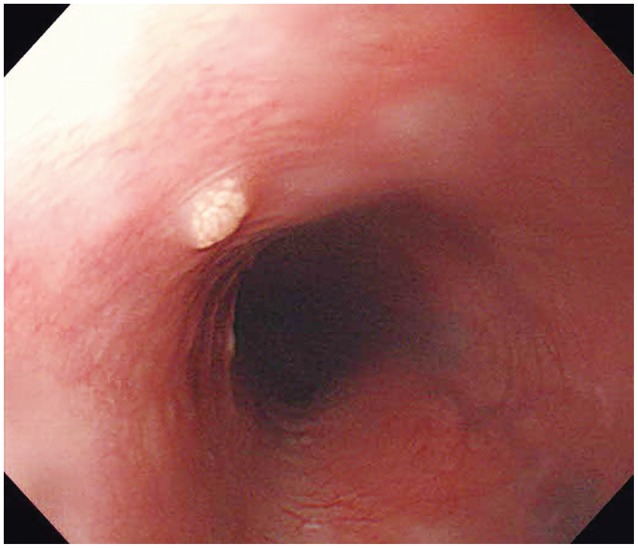
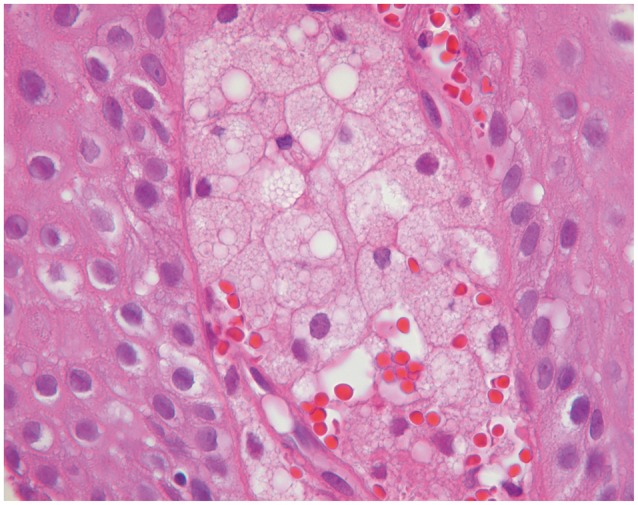
A 70-year-old man with an unremarkable medical history was hospitalized with a complaint of epigastric pain. Physical examination revealed epigastric tenderness; however, other examination findings were normal. No abnormal findings were detected on laboratory and radiologic examinations. Serum total cholesterol, triglyceride, high density lipoprotein cholesterol, and low density lipoprotein cholesterol levels were 151, 215, 33, and 102 mg/dL, respectively. Endoscopic examination was performed to find the cause of the epigastric pain. Multiple shallow gastric ulcers and a duodenal ulcer were detected and suspected to be the cause of the pain. Aspirin medication was the suspected cause of the multiple ulcers. Besides the ulcers, in the upper esophagus 20 cm from the incisors, a 3-mm yellowish granular elevated mucosal lesion was found and a biopsy was performed (Fig. 1). Microscopically, large round cells were aggregated in the lamina propria immediately beneath the squamous epithelium. The cells had small nuclei that were centrally or eccentrically located. The cytoplasm was sparse and contained vacuoles (Fig. 2). The lesion was diagnosed histologically as xanthoma of the esophagus.
DISCUSSION
Xanthoma and VX are usually considered different diseases. The etiologies are different, as xanthoma is caused by hyperlipidemia and VX arises presumably as a result of an inflammatory response to continuous mucosal damage.1 However, the etiologies of the two lesions arising in the esophagus are not understood. The characteristics of all reported cases of xanthoma and VX of the esophagus are summarized in Table 1.
Fourteen cases of xanthoma and four cases of VX of the esophagus have been reported. However, some reports loosely stratified VX into esophageal xanthoma, whereas others have excluded it.6,8 In terms of clinical data, both diseases were found predominantly in men than in women: 9 versus 3 in xanthoma and 3 versus 1 in VX. The median age was 59 years (range, 37 to 74) in xanthoma and. 65.5 years (range, 49 to 74) in VX. The predominant location was the lower esophagus for xanthoma (lower, 7; middle, 2; upper, 3), whereas VX was not reported in the lower esophagus (upper, 2; middle, 2). The median size was not different: 3 mm (range, 2 to 10) for xanthoma and 4 mm (range, 3 to 20) for VX.
The associated medical conditions were diverse; however, two patients with malignant tumors were included in each group: hepatocellular carcinoma and ileocecal lymphoma in xanthoma, and gastric cancer and multifocal cancer (cancer of the glottis, liver, and trachea) in VX, although there was no definite association.
VX is characterized by its histologic features, including papillomatosis, acanthosis, and hyperparakeratosis.11 Also, the external morphology is verrucoid. Nevertheless, findings of large round foam cells in the lamina propria under the squamous epithelium are the same as those in xanthoma. It is difficult to differentiate between the two lesions on the basis of gross examination when they arise on the esophagus. Exophytic and verrucoid features seen in VX of the skin were not observed in the esophagus because most of the reported cases were small in size.10,12
Considering that xanthoma and VX are nonneoplastic lesions, differentiating between them could be a waste of effort. However, these lesions have to be grossly distinguished from ectopic sebaceous glands and small subepithelial tumors such as carcinoid and granular cell tumor because most of the reported esophageal xanthomas are yellowish or white mucosal elevated lesions. In terms of microscopic findings, signet ring cell carcinoma, which contains round cells with abundant cytoplasm, should be distinguished. While signet ring cell carcinoma has an eccentrically located nucleus because of the intracellularly abundant mucin, xanthoma has a centrally located and small nucleus. Accumulation of foamy histiocytes of xanthoma could be a clue for the differential diagnosis. Positive immunohistochemical staining for CD68, which indicates a histiocytic origin, is another characteristic finding of xanthoma.5 Moreover, esophageal cancer and ectopic sebaceous glands do not commonly stain with Lugol's solution; thus, endoscopists need to be aware of these lesions for the differential diagnosis.6,14 With more case reports of esophageal xanthoma and VX of the esophagus, the characteristics of both lesions will be more clearly elucidated.