HOME
ABOUT
Aims and Scope
About the Journal
Editorial Board
Open Access
Best Practice
Subscription
Management Team and Credential
Editorial Office
BROWSE ARTICLES
All issues
Ahead-of Print Articles
Current Issue
Most Read Articles
Most Cited Articles
Guidelines in CE
Review Articles
Systematic Review, Meta-Analysis
Articles with Video
Boost Your Learning with Quiz
Funded Articles
Advanced Search
Author Index
CURRENT ISSUE
EDITORIAL POLICY
Research and Publication Ethics
Peer Review Policy
Advertising Policy
Data Sharing Policy
Data Archiving Policy
Preprint Policy
FOR AUTHORS AND REVIEWERS
Instructions for Authors
Instructions for Reviewers
Checklist
E-Submission
Copyright Transfer Form
Permission for Reproduction
Article Processing Charge
Epub Ahead-of Print Articles
> Browse Articles > Epub Ahead-of Print Articles
Reviews
Clinical meaning of sarcopenia in patients undergoing endoscopic treatment
(View : 1,576 times)
Hiroyuki Hisada, Yosuke Tsuji, Hikaru Kuribara, et al.
Received July 26, 2023 Accepted August 18, 2023 Published online March 22, 2024
[Epub ahead of print]
Full text
PubReader
ePub
PDF
Colon stenting as a bridge to surgery in obstructive colorectal cancer management
(View : 1,501 times)
Dong Hyun Kim, Han Hee Lee
Received May 23, 2023 Accepted July 29, 2023 Published online March 8, 2024
[Epub ahead of print]
Full text
PubReader
ePub
PDF
As how artificial intelligence is revolutionizing endoscopy
(View : 1,478 times)
Jean-Francois Rey
Received September 13, 2023 Accepted October 15, 2023 Published online March 8, 2024
[Epub ahead of print]
Full text
PubReader
ePub
PDF
Potassium-competitive acid blocker-associated gastric mucosal lesions
(View : 2,607 times)
Kimitoshi Kubo, Noriko Kimura, Mototsugu Kato
Received November 2, 2023 Accepted November 27, 2023 Published online February 29, 2024
[Epub ahead of print]
Crossref 1
Full text
PubReader
ePub
PDF
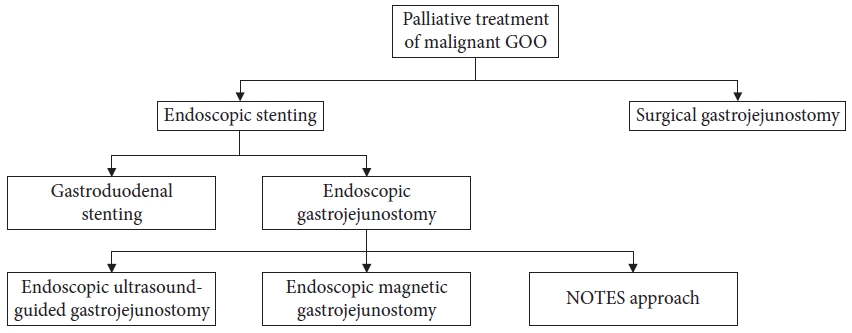
Endoscopic stenting for malignant gastric outlet obstruction: focusing on comparison of endoscopic stenting and surgical gastrojejunostomy
(View : 1,359 times)
Sun Gyo Lim, Chan Gyoo Kim
Received June 30, 2023 Accepted September 11, 2023 Published online February 23, 2024
[Epub ahead of print]
Full text
PubReader
ePub
PDF
Role of endoscopic duodenojejunal bypass liner in obesity management and glycemic control
(View : 1,656 times)
Willian Ferreira Igi, Victor Lira de Oliveira, Ayah Matar, Diogo Turiani Hourneaux de Moura
Received August 31, 2023 Accepted October 10, 2023 Published online February 15, 2024
[Epub ahead of print]
Crossref 1
Full text
PubReader
ePub
PDF
The role of cap-assisted endoscopy and its future implications
(View : 1,544 times)
Sol Kim, Bo-In Lee
Received February 13, 2023 Accepted May 12, 2023 Published online February 7, 2024
[Epub ahead of print]
Full text
PubReader
ePub
PDF
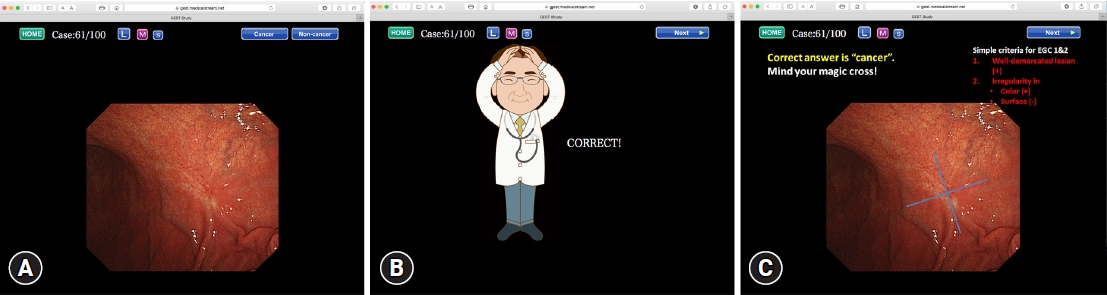
E-learning system to improve the endoscopic diagnosis of early gastric cancer
(View : 1,459 times)
Kenshi Yao, Takashi Yao, Noriya Uedo, et al.
Received March 14, 2023 Accepted April 23, 2023 Published online August 3, 2023
[Epub ahead of print]
Full text
PubReader
ePub
PDF
Systematic Review and Meta-analysises
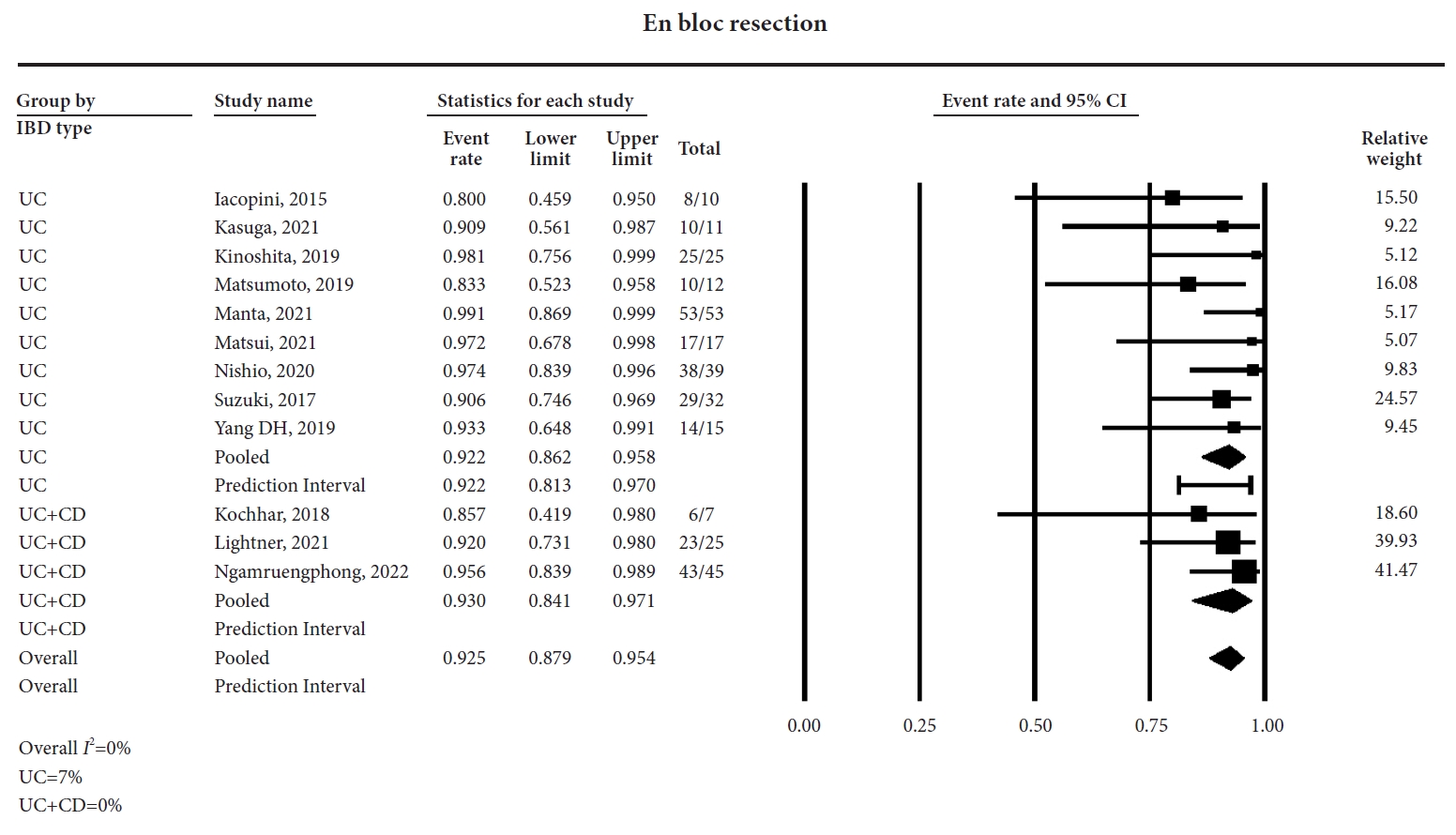
Efficacy and safety of endoscopic submucosal dissection for colorectal dysplasia in patients with inflammatory bowel disease: a systematic review and meta-analysis
(View : 1,728 times)
Talia F. Malik, Vaishnavi Sabesan, Babu P. Mohan, et al.
Received August 11, 2023 Accepted September 27, 2023 Published online February 29, 2024
[Epub ahead of print]
Full text
PubReader
ePub
PDF
Supplementary Material
Editorials
Is your endoscopist qualified enough to detect
Helicobacter pylori
-naive status?
(View : 1,193 times)
Sun-Young Lee
Received February 14, 2024 Accepted February 22, 2024 Published online April 12, 2024
[Epub ahead of print]
Full text
PubReader
ePub
PDF
Original Articles
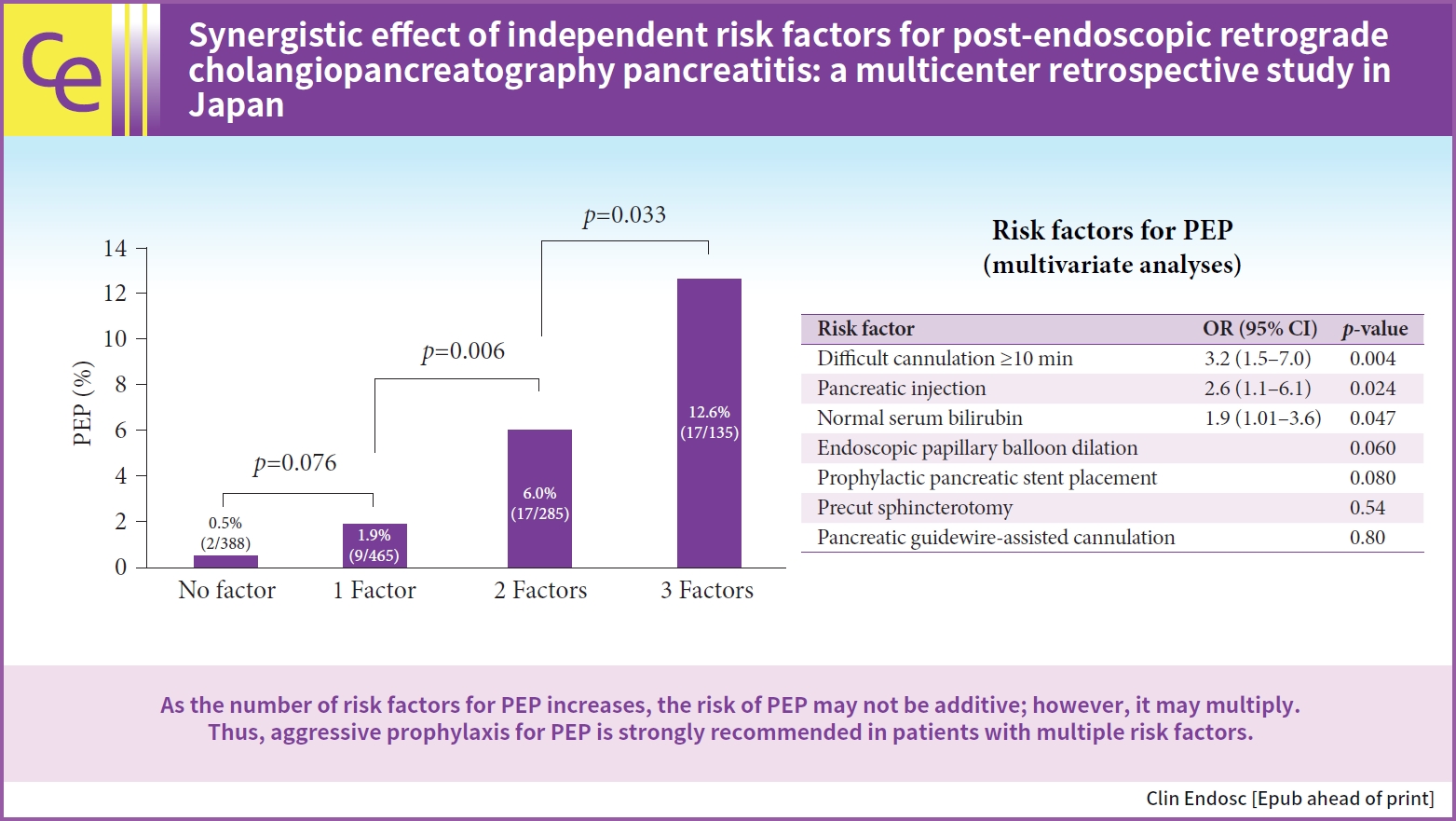
Synergistic effect of independent risk factors for post-endoscopic retrograde cholangiopancreatography pancreatitis: a multicenter retrospective study in Japan
(View : 1,019 times)
Hirokazu Saito, Yoshihiro Kadono, Takashi Shono, et al.
Received August 14, 2023 Accepted October 10, 2023 Published online April 18, 2024
[Epub ahead of print]
Full text
PubReader
ePub
PDF
Development of a predictive model for hypoxia due to sedatives in gastrointestinal endoscopy: a prospective clinical study in Korea
(View : 1,471 times)
Jung Wan Choe, Jong Jin Hyun, Seong-Jin Son, Seung-Hak Lee
Received August 4, 2023 Accepted December 5, 2023 Published online April 12, 2024
[Epub ahead of print]
Full text
PubReader
ePub
PDF
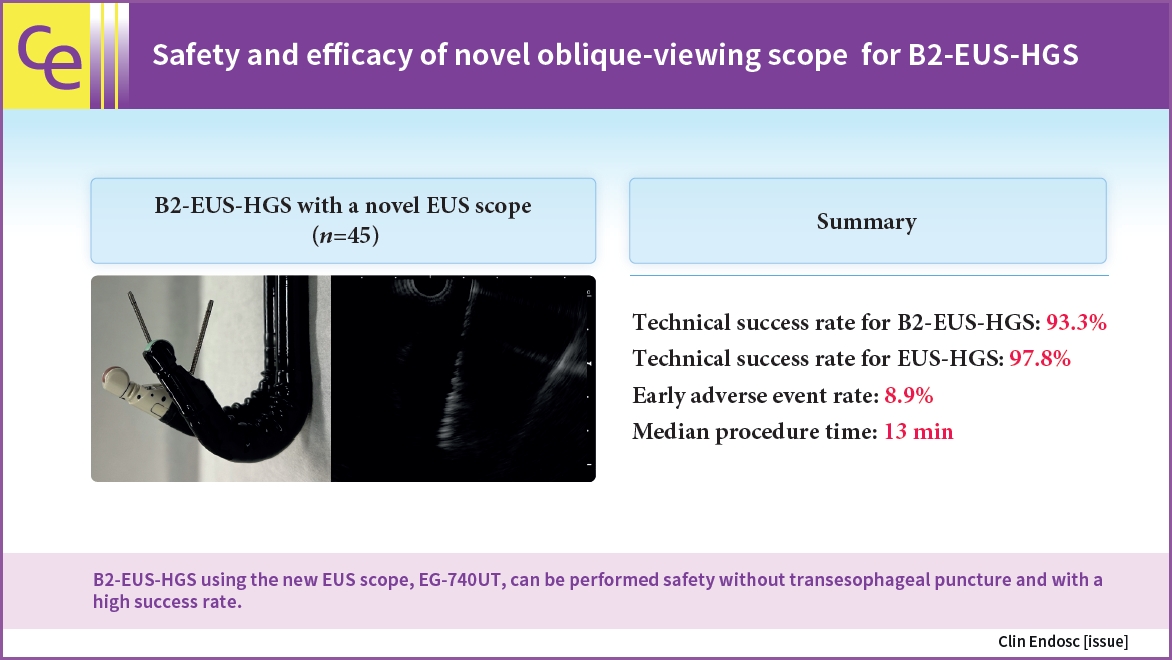
Safety and efficacy of novel oblique-viewing scope for B2-endoscopic ultrasound-guided hepaticogastrostomy
(View : 1,596 times)
Sho Ishikawa, Kazuo Hara, Nozomi Okuno, et al.
Received May 16, 2023 Accepted July 7, 2023 Published online March 29, 2024
[Epub ahead of print]
Full text
PubReader
ePub
PDF
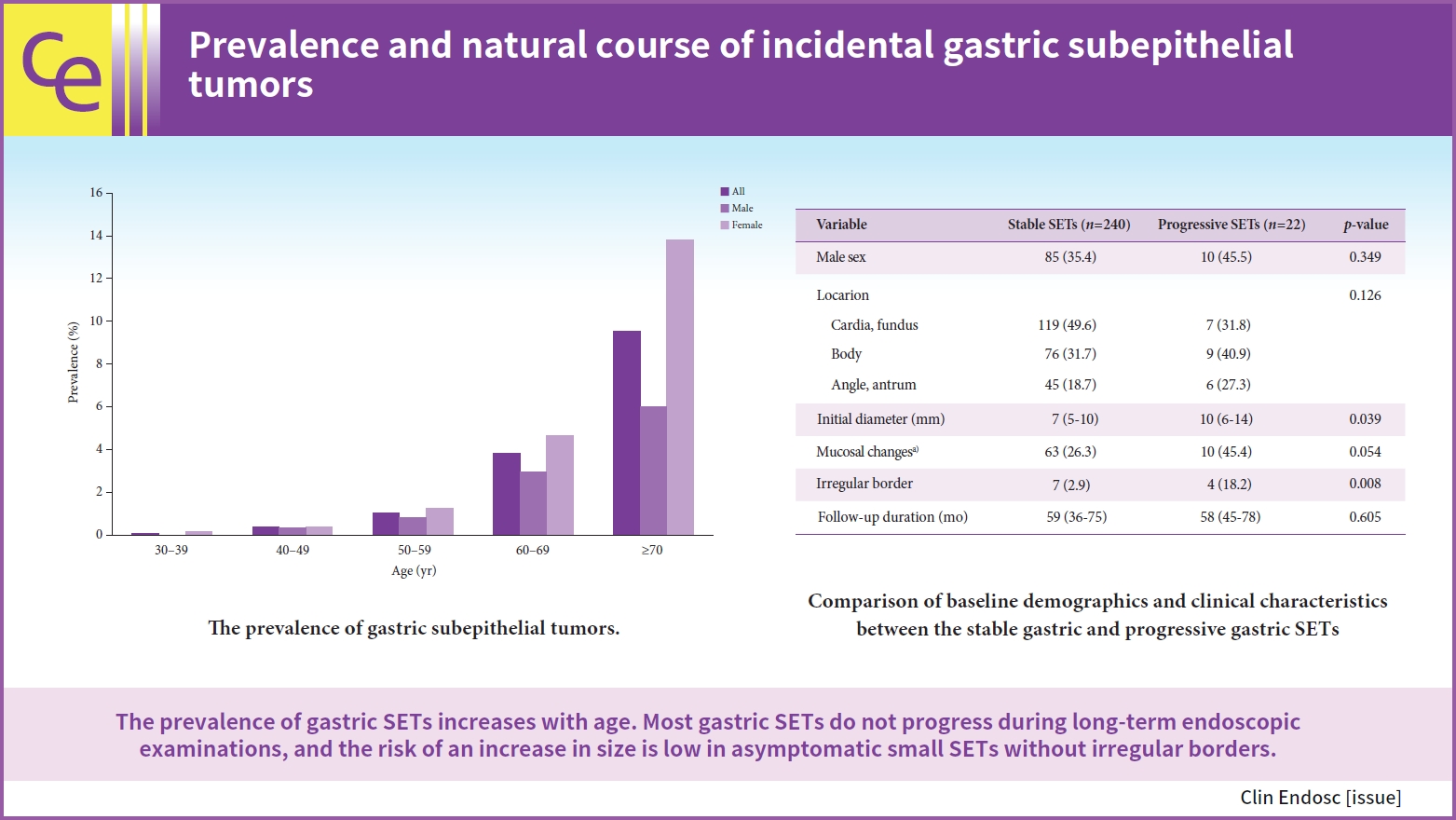
Prevalence and natural course of incidental gastric subepithelial tumors
(View : 1,234 times)
Dae-Hyuk Heo, Min A Yang, Jae Sun Song, Won Dong Lee, Jin Woong Cho
Received May 4, 2023 Accepted July 16, 2023 Published online March 29, 2024
[Epub ahead of print]
Full text
PubReader
ePub
PDF
Clinicopathological and endoscopic features of
Helicobacter pylori
infection-negative gastric cancer in Japan: a retrospective study
(View : 1,998 times)
Kentaro Imamura, Kenshi Yao, Satoshi Nimura, et al.
Received October 7, 2023 Accepted November 25, 2023 Published online March 22, 2024
[Epub ahead of print]
Full text
PubReader
ePub
PDF
Current status and clinical outcome of endoscopic hemostatic powder in gastrointestinal bleeding: a retrospective multicenter study
(View : 1,446 times)
Zie Hae Lim, Seung In Seo, Dae-Seong Myung, et al.
Received July 14, 2023 Accepted October 12, 2023 Published online March 8, 2024
[Epub ahead of print]
Full text
PubReader
ePub
PDF
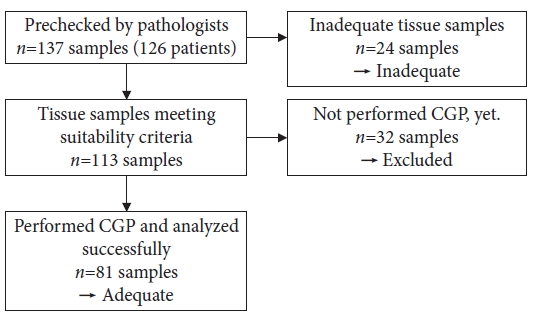
Clinical utility of endoscopic ultrasound-guided tissue acquisition for comprehensive genomic profiling of patients with biliary tract cancer, especially with intrahepatic cholangiocarcinoma
(View : 1,442 times)
Takafumi Yanaidani, Kazuo Hara, Nozomi Okuno, et al.
Received May 27, 2023 Accepted August 26, 2023 Published online February 15, 2024
[Epub ahead of print]
Full text
PubReader
ePub
PDF
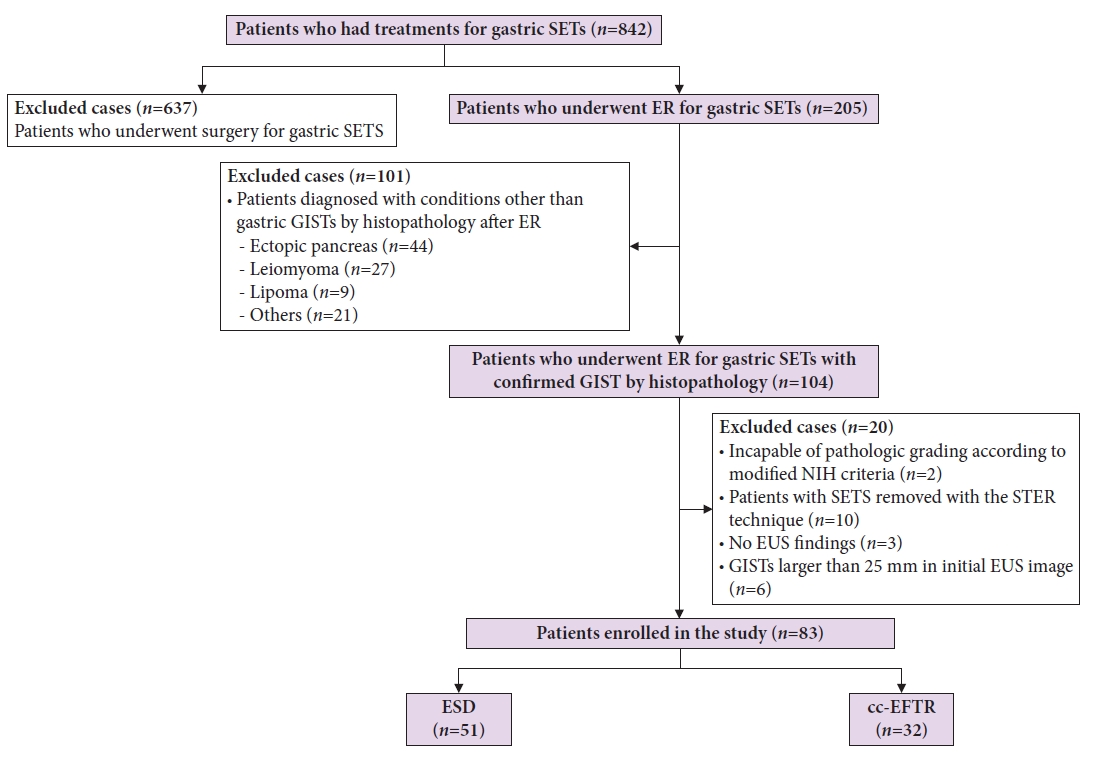
Endoscopic resection of gastric gastrointestinal stromal tumor using clip-and-cut endoscopic full-thickness resection: a single-center, retrospective cohort in Korea
(View : 1,645 times)
Yuri Kim, Ji Yong Ahn, Hwoon-Yong Jung, et al.
Received May 31, 2023 Accepted November 19, 2023 Published online February 15, 2024
[Epub ahead of print]
Full text
PubReader
ePub
PDF
Supplementary Material
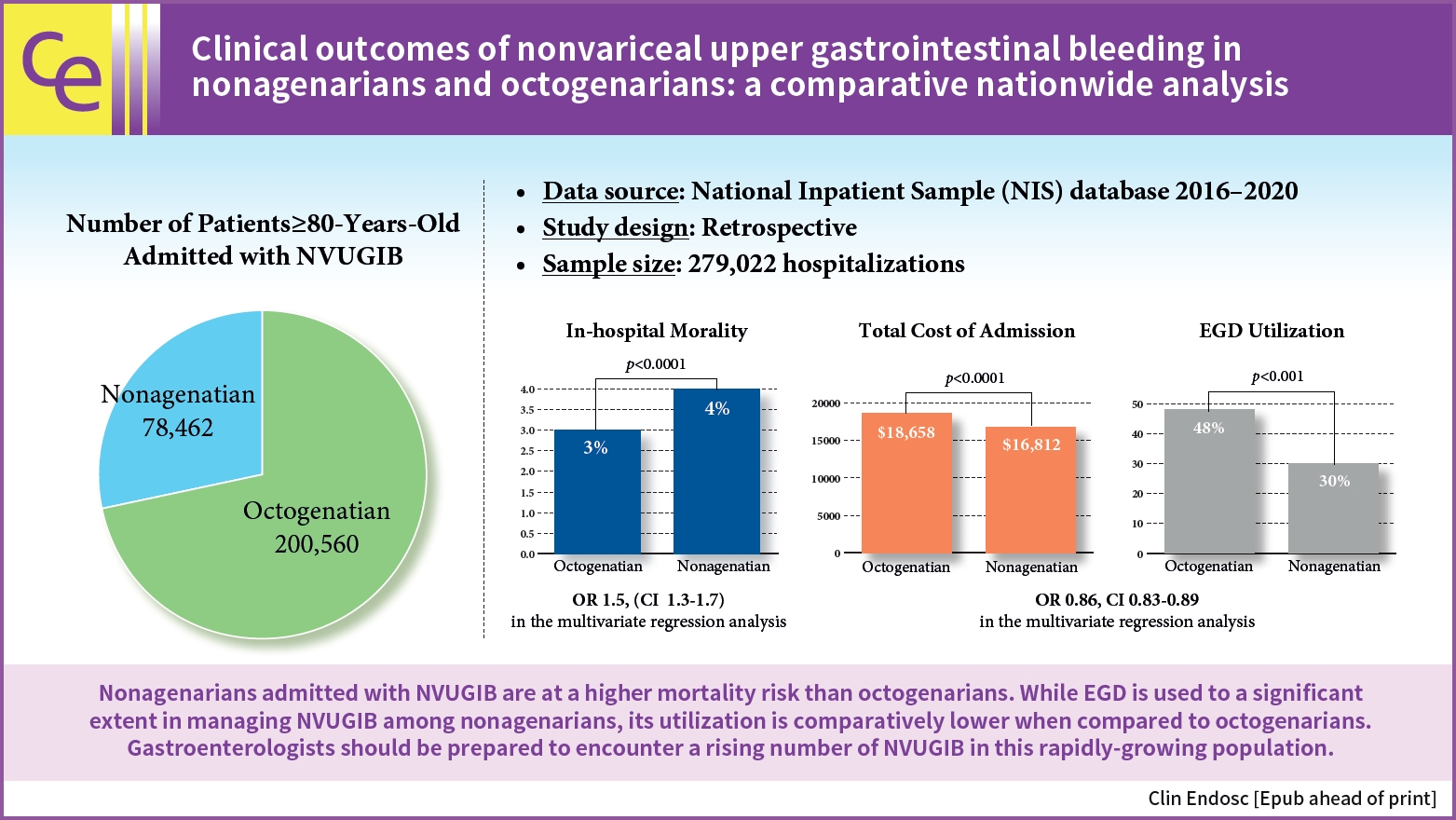
Clinical outcomes of nonvariceal upper gastrointestinal bleeding in nonagenarians and octogenarians: a comparative nationwide analysis
(View : 1,472 times)
Khaled Elfert, James Love, Esraa Elromisy, et al.
Received May 11, 2023 Accepted July 13, 2023 Published online February 7, 2024
[Epub ahead of print]
Full text
PubReader
ePub
PDF
Supplementary Material
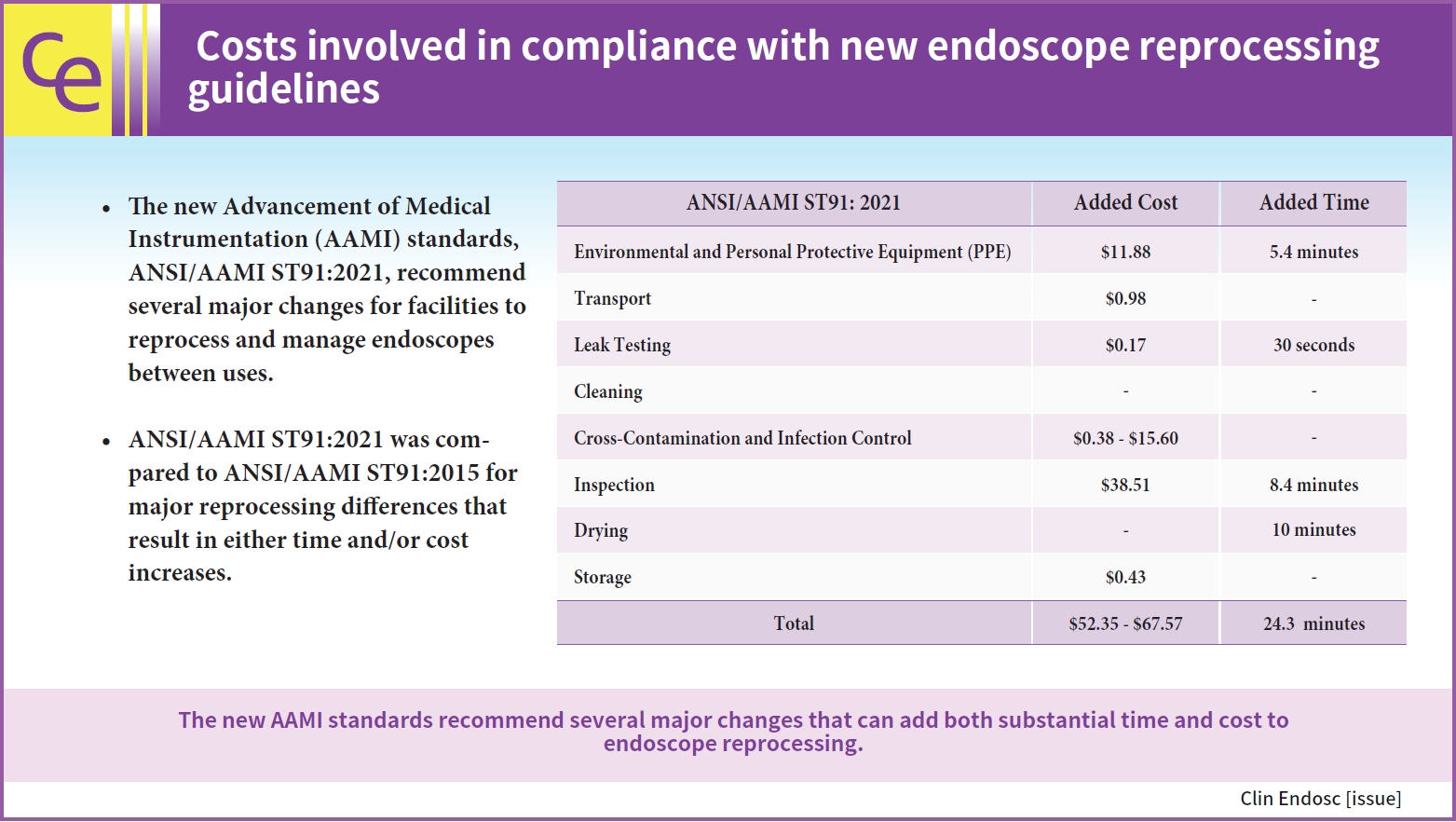
Costs involved in compliance with new endoscope reprocessing guidelines
(View : 1,624 times)
David Hoffman, Christina Cool
Received June 28, 2023 Accepted September 21, 2023 Published online January 26, 2024
[Epub ahead of print]
Full text
PubReader
ePub
PDF
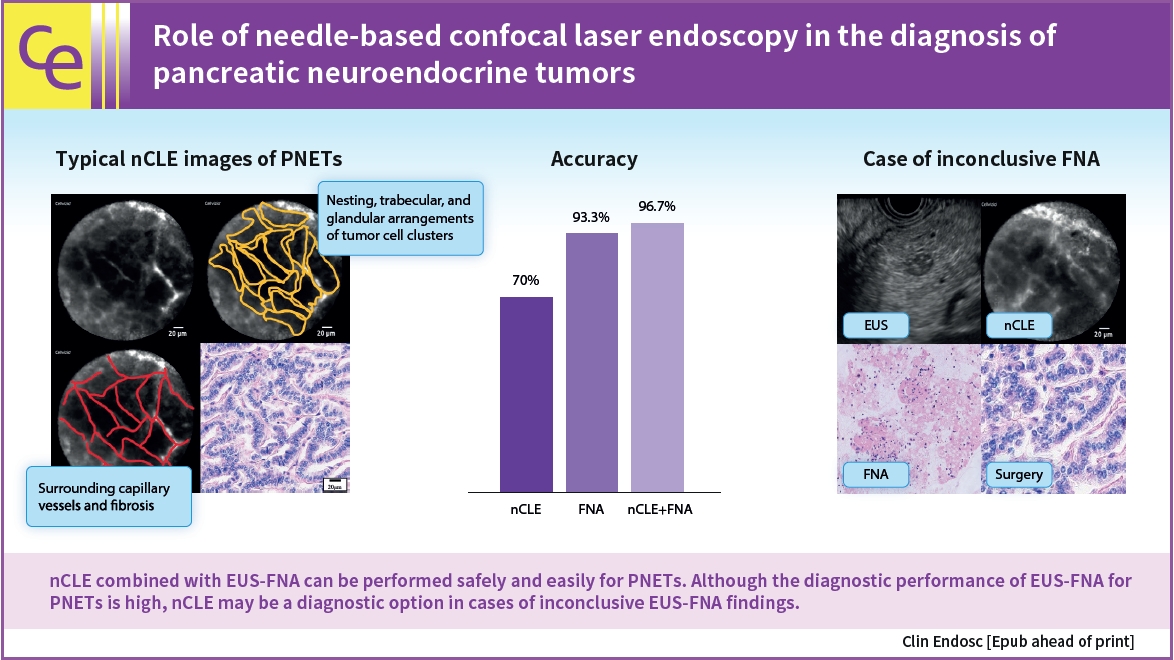
The role of needle-based confocal laser endoscopy in the diagnosis of pancreatic neuroendocrine tumors
(View : 1,835 times)
Masanori Yamada, Kazuo Hara, Nobumasa Mizuno, et al.
Received March 1, 2023 Accepted April 19, 2023 Published online September 12, 2023
[Epub ahead of print]
Full text
PubReader
ePub
PDF
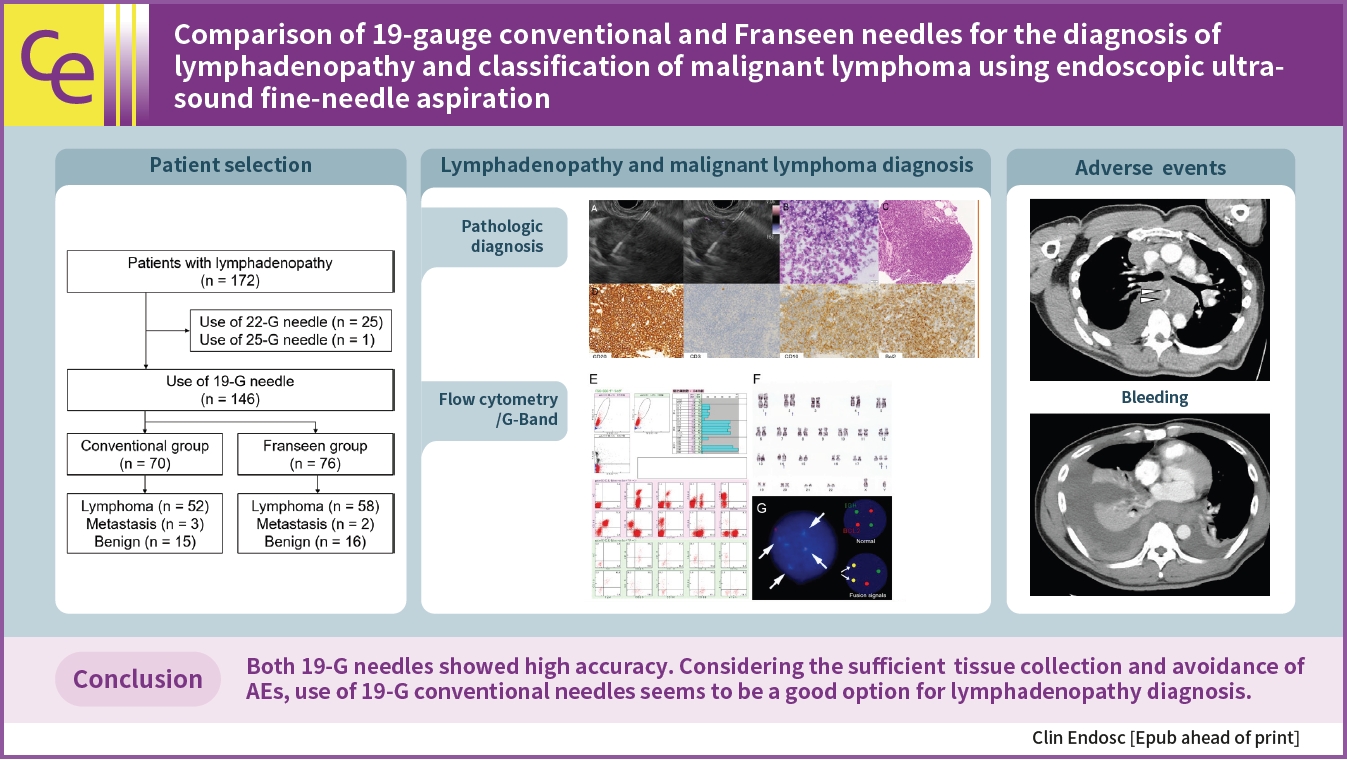
Comparison of 19-gauge conventional and Franseen needles for the diagnosis of lymphadenopathy and classification of malignant lymphoma using endoscopic ultrasound fine-needle aspiration
(View : 1,569 times)
Mitsuru Okuno, Keisuke Iwata, Tsuyoshi Mukai, et al.
Received March 25, 2023 Accepted May 11, 2023 Published online September 8, 2023
[Epub ahead of print]
Full text
PubReader
ePub
PDF
Supplementary Material
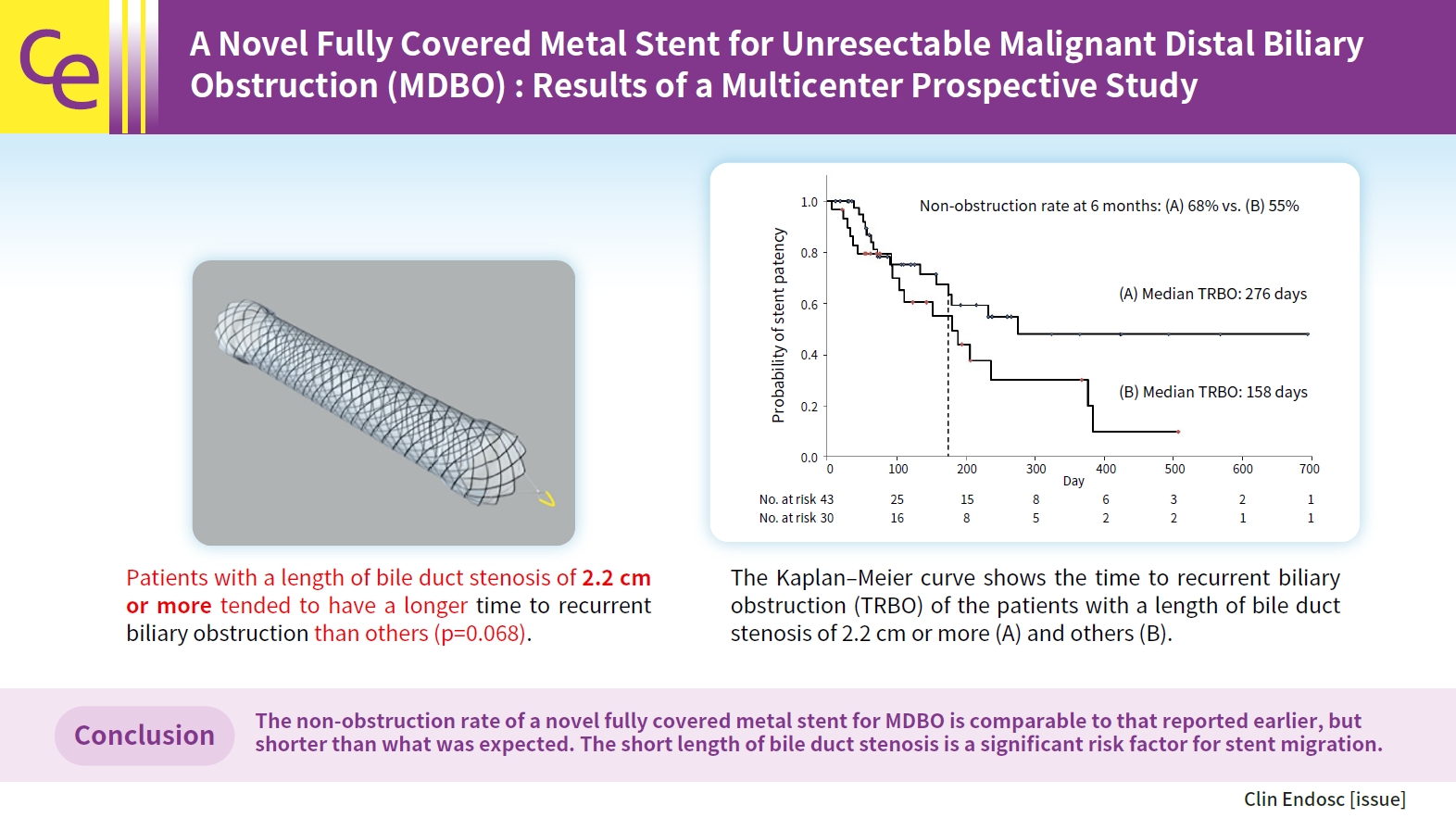
A novel fully covered metal stent for unresectable malignant distal biliary obstruction: results of a multicenter prospective study
(View : 1,962 times)
Arata Sakai, Atsuhiro Masuda, Takaaki Eguchi, et al.
Received January 28, 2023 Accepted April 18, 2023 Published online July 10, 2023
[Epub ahead of print]
Crossref 2
Full text
PubReader
ePub
PDF
Supplementary Material
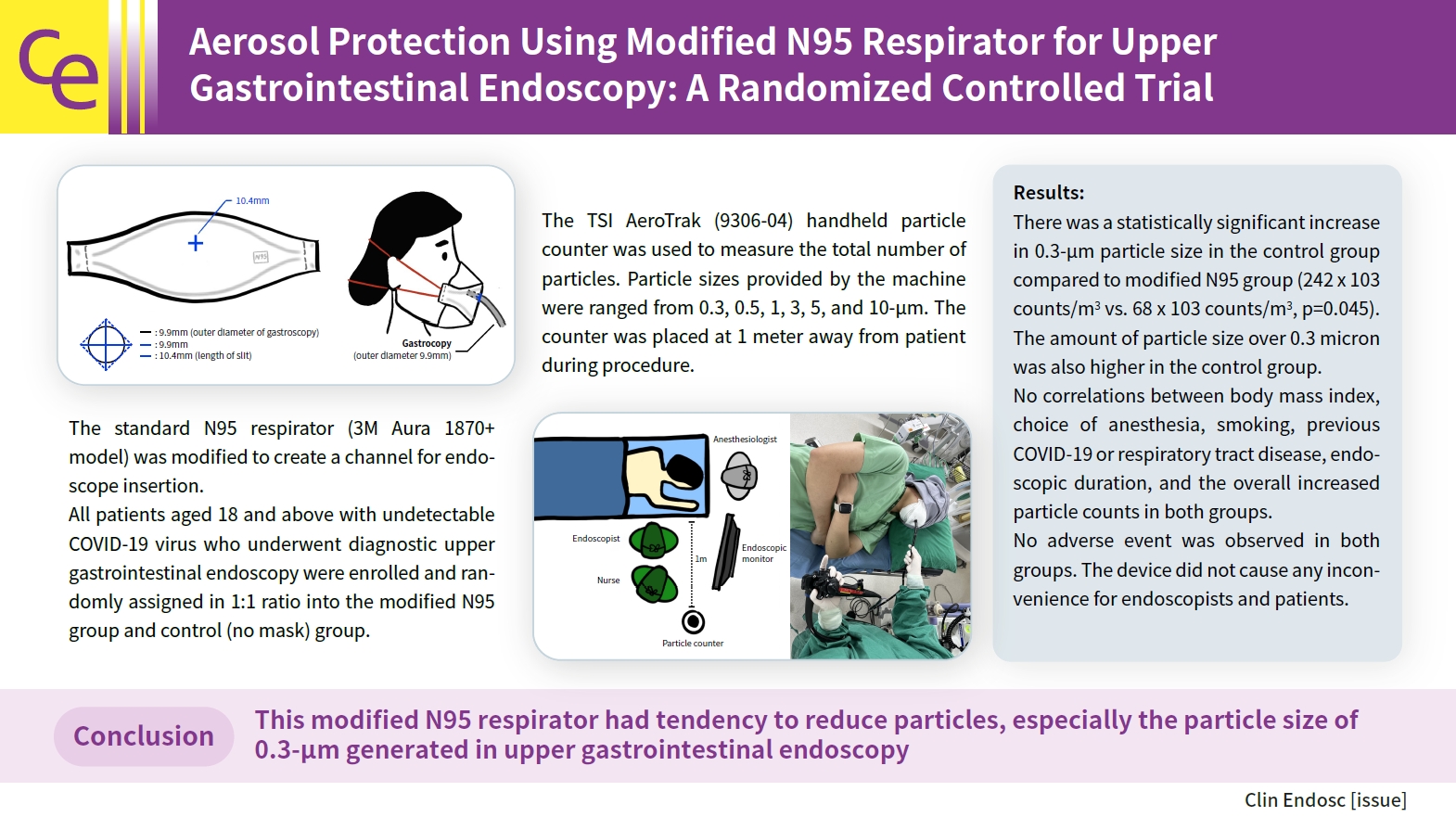
Aerosol protection using modified N95 respirator during upper gastrointestinal endoscopy: a randomized controlled trial
(View : 1,836 times)
Chawisa Nampoolsuksan, Thawatchai Akaraviputh, Asada Methasate, et al.
Received December 27, 2022 Accepted February 22, 2023 Published online June 21, 2023
[Epub ahead of print]
Full text
PubReader
ePub
PDF
Case Reports
Polyposis of gastrointestinal tract after COVID-19 mRNA vaccination: a report of two cases
(View : 1,388 times)
Jun Ho Kim, Eun Hye Oh, Dong Soo Han
Received October 19, 2023 Accepted December 6, 2023 Published online April 12, 2024
[Epub ahead of print]
Full text
PubReader
ePub
PDF
Endoscopic ultrasound-guided hepaticogastrostomy by puncturing both B2 and B3: a single center experience
(View : 1,101 times)
Moaz Elshair, Kazuo Hara, Nozomi Okuno, et al.
Received August 12, 2022 Accepted November 23, 2022 Published online May 3, 2023
[Epub ahead of print]
Full text
PubReader
ePub
PDF
Image of Issue
Aortoduodenal fistula bleeding caused by an aortic stent graft
(View : 1,520 times)
Seunghyun Hong, Gwang Ha Kim
Received November 4, 2023 Accepted November 30, 2023 Published online February 2, 2024
[Epub ahead of print]
Full text
PubReader
ePub
PDF
Brief Reports
Long-term follow-up of patients developing gastric mucosal lesions after initiating the potassium-competitive acid blocker vonoprazan
(View : 1,287 times)
Kimitoshi Kubo, Noriko Kimura
Received July 20, 2023 Accepted August 5, 2023 Published online April 18, 2024
[Epub ahead of print]
Full text
PubReader
ePub
PDF
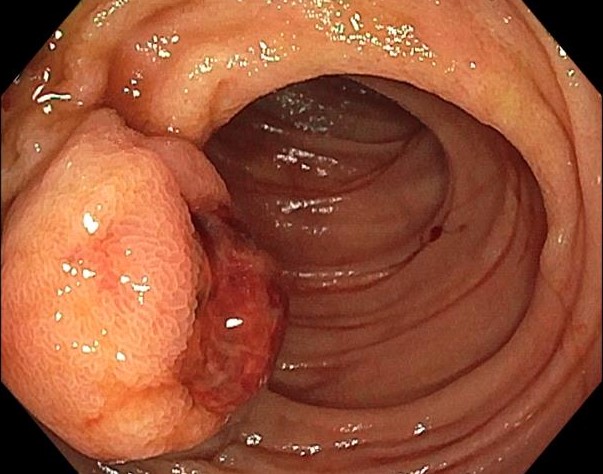
Jejunal DieulafoyвҖҷs lesion resembling subepithelial mass resulting in profound gastrointestinal hemorrhage
(View : 1,532 times)
Thanaboon Chaemsupaphan, Tanawat Geeratragool, Napat Angkathunyakul, Arissa Phothisirisakulwong, Monthira Maneerattanaporn
Received September 14, 2023 Accepted September 30, 2023 Published online March 29, 2024
[Epub ahead of print]
Full text
PubReader
ePub
PDF
Use of an endoscopic powered debridement device for treatment of post-surgical fatty pancreatic necrosis
(View : 1,323 times)
Judy Daboul, Shiab Mussad, Anna Cecilia Amaral, Waleed K. Hussain, Peter J. Lee, Samuel Han
Received May 2, 2023 Accepted May 30, 2023 Published online February 23, 2024
[Epub ahead of print]
Full text
PubReader
ePub
PDF
Supplementary Material
Effective hemostasis under gel immersion endoscopy using inflated balloons on the tip of double balloon endoscope for active bleeding in the small intestine
(View : 1,489 times)
Shunsuke Horitani, Natsuko Saito, Koki Hosoda, et al.
Received May 29, 2023 Accepted July 7, 2023 Published online February 8, 2024
[Epub ahead of print]
Full text
PubReader
ePub
PDF
Supplementary Material
Boost Your Learning with Quiz
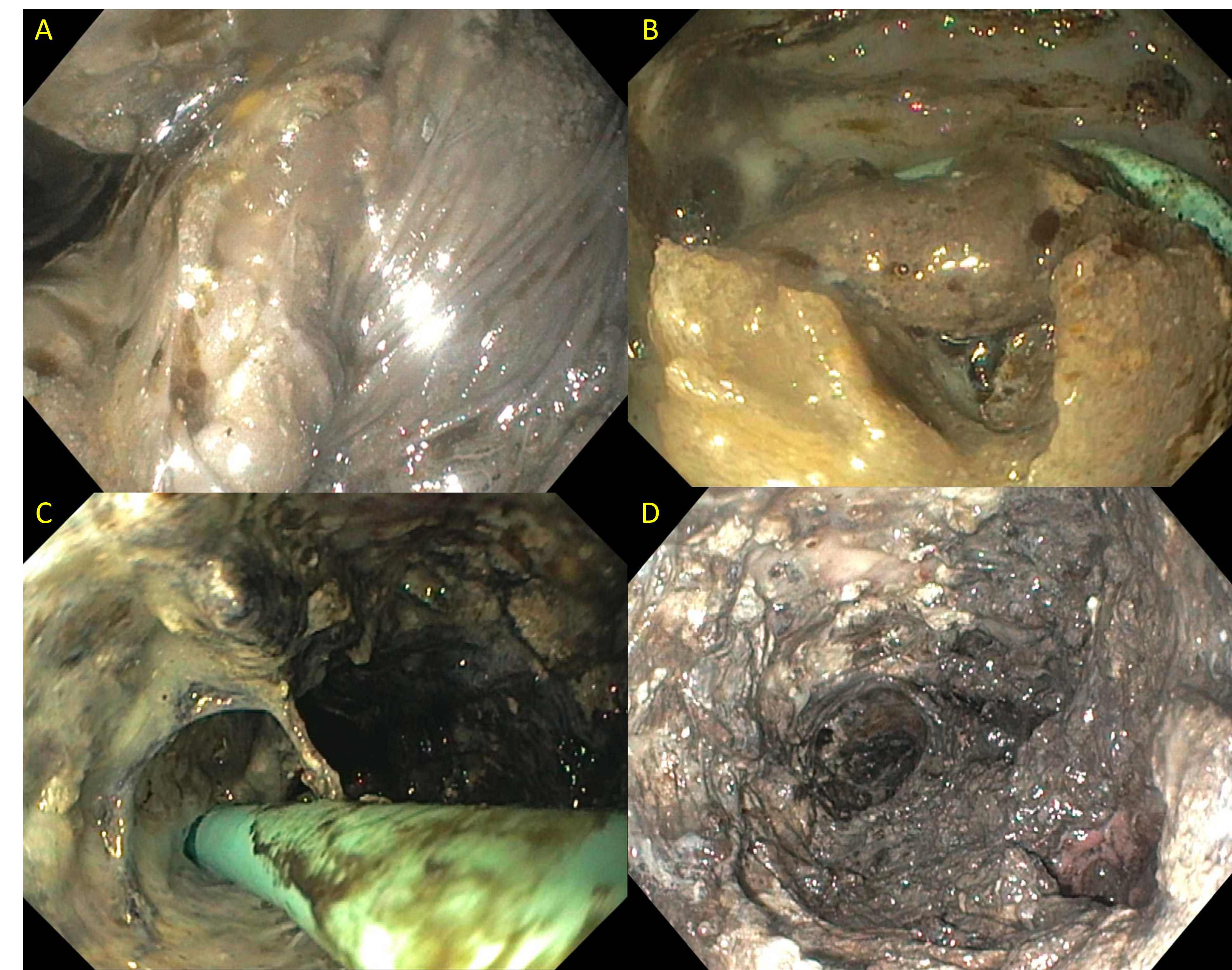
A rare colonoscopic finding in a renal transplant recipient
(View : 1,583 times)
Ji Young Chang, Soo Jung Park
Received January 5, 2024 Accepted January 23, 2024 Published online March 22, 2024
[Epub ahead of print]
Full text
PubReader
ePub
PDF
Journal Impact Factor 2.5
Endoscopic ultrasound-guided gastrojejunostomy with a direct technique without previous intestinal filling using a tubular fully covered self-expandable metallic stent. Clin Endosc. 2024;57:209-216
 > Browse Articles > Epub Ahead-of Print Articles
> Browse Articles > Epub Ahead-of Print Articles