INTRODUCTION
Achalasia, a disorder of esophageal dysmotility, is characterized by failure of the lower esophageal sphincter (LES) to relax and the lack of functional peristalsis in the esophageal body because of progressive degeneration of ganglion cells in the myenteric plexus of the esophageal wall. Clinically, patients develop dysphagia, regurgitation, heartburn, chest pain, and/or weight loss. Although the severity of symptoms may vary, the disease burden is high, and achalasia can have a significant impact on patientŌĆÖs health-related quality of life.
Peroral endoscopic myotomy (POEM) is an endoscopic procedure, which combines the minimally invasive benefit of endoscopy with the durability of a surgical myotomy. POEM involves endoscopic submucosal tunneling, followed by dissection and division of the circular muscle fibers of the esophagus and LES. Although the steps of the procedure are generally performed similarly in institutions across the world, there is some variability with regard to the equipment used to perform POEM [1,2]. Previous studies have investigated the use of conventional versus hybrid knife in POEM [1]; however, little is known about the safety and efficacy of electrocautery enhanced scissors (EES) in esophageal myotomy. Although the use of an additional device may increase procedure time and cost, the benefits of using this device, including improved accuracy and precision of myotomy, ability to provide hemostasis without the need to exchange devices, and improved safety in training fellows, make this a viable tool for POEM. Thus, this study aimed to analyze the safety and efficacy of the use of EES in POEM at an academic institution with a fellowship training program.
MATERIALS AND METHODS
In this retrospective cohort study, the data of adult patients aged Ōēź18 years with normal foregut anatomy who underwent POEM using EES between September 2017 and November 2018 at a large academic institution in Boston, MA, USA were prospectively collected. This study was approved by the Institutional Review Board. During this prospective series, all myotomy procedures were performed by our group using EES. PatientsŌĆÖ baseline characteristics, including indications for intervention, and procedure details (procedure time, tunnel length, myotomy length and depth, and myotomy location) were recorded.
Peroral endoscopic myotomy procedure
POEM procedures were performed in a manner similar to that initially described by Inoue et al. [3], and further details on the endoscopic myotomy using the EES device are described below. A forward-viewing upper endoscope (GIF-HQ190; Olympus America, Center Valley, PA, USA) and an electrosurgical generator (VIO 300 D; Erbe USA, Marietta, GA, USA) were used for all POEM procedures. A tapered-tip distal attachment cap (ST Hood; Fujifilm Medical Systems, Stamford, CT, USA) and DualKnife J (Olympus) or Flush-Knife (Fujifilm) were used for submucosal tunneling (Endocut [Effect 2, Cut Duration 2, Cut Interval 2], Spray Coag effect 2, 50 W), and a regular attachment cap (Olympus) and EES (SB Knife Jr; Olympus; Fig. 1) were used for the myotomy (Endocut [Effect 2, Cut Duration 2, Cut Interval 2], Soft Coag effect 5, 50 W). The EES device can be used through a standard upper diagnostic endoscopic channel and is operated by both the endoscopist and an assistant. EES is a fully rotatable knife that can be maneuvered independently by the physician, which allows cutting in a horizontal or vertical axis [4]. It has an insulated scissor-type blade that is lined with a cutting electrode and allows the endoscopist to pull the tissue backward toward the scope prior to cutting to minimize the risk of tissue damage or perforation [4]. Hemostatic forceps (Coagrasper; Olympus) was used for sealing of larger vessels and hemostasis (Soft Coag effect 5, 50 W). A carbon dioxide insufflator was used in all cases. For final closure of the mucosal entry site, hemostatic clips (DuraClip; CONMED, Utica, NY, USA) or endoscopic suturing device (OverStitchTM; Apollo Endosurgery, Austin, TX, USA) was used. Patients fasted for >12 hours prior to the POEM, which was performed under general anesthesia with endotracheal intubation. All procedures were supervised or performed by a senior endoscopist (HA or CCT) with either a general gastroenterology or an advanced endoscopy fellow. All patients were admitted to the inpatient ward following the procedure for observation. Patients were kept nil per os and received intravenous (IV) proton-pump-inhibitor (PPI) and IV ciprofloxacin and metronidazole overnight. On post-operative day 1, patients underwent a barium swallow to assess for perforation or leak. PatientsŌĆÖ diet was then advanced to a clear liquid diet for 2 days, followed by a full liquid diet for 12 days, and then a soft diet with advancement as tolerated. Patients continued oral PPI for 8 weeks and completed a total of a 5-day course of ciprofloxacin and metronidazole.
Endoscopic myotomy
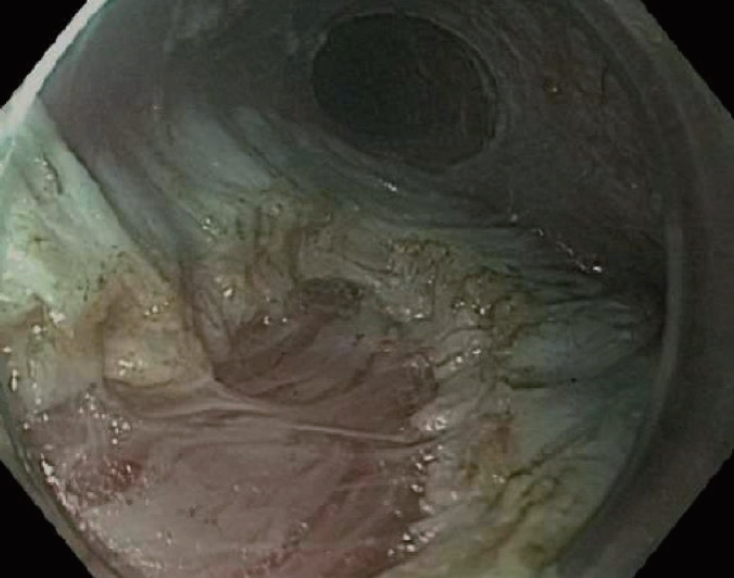
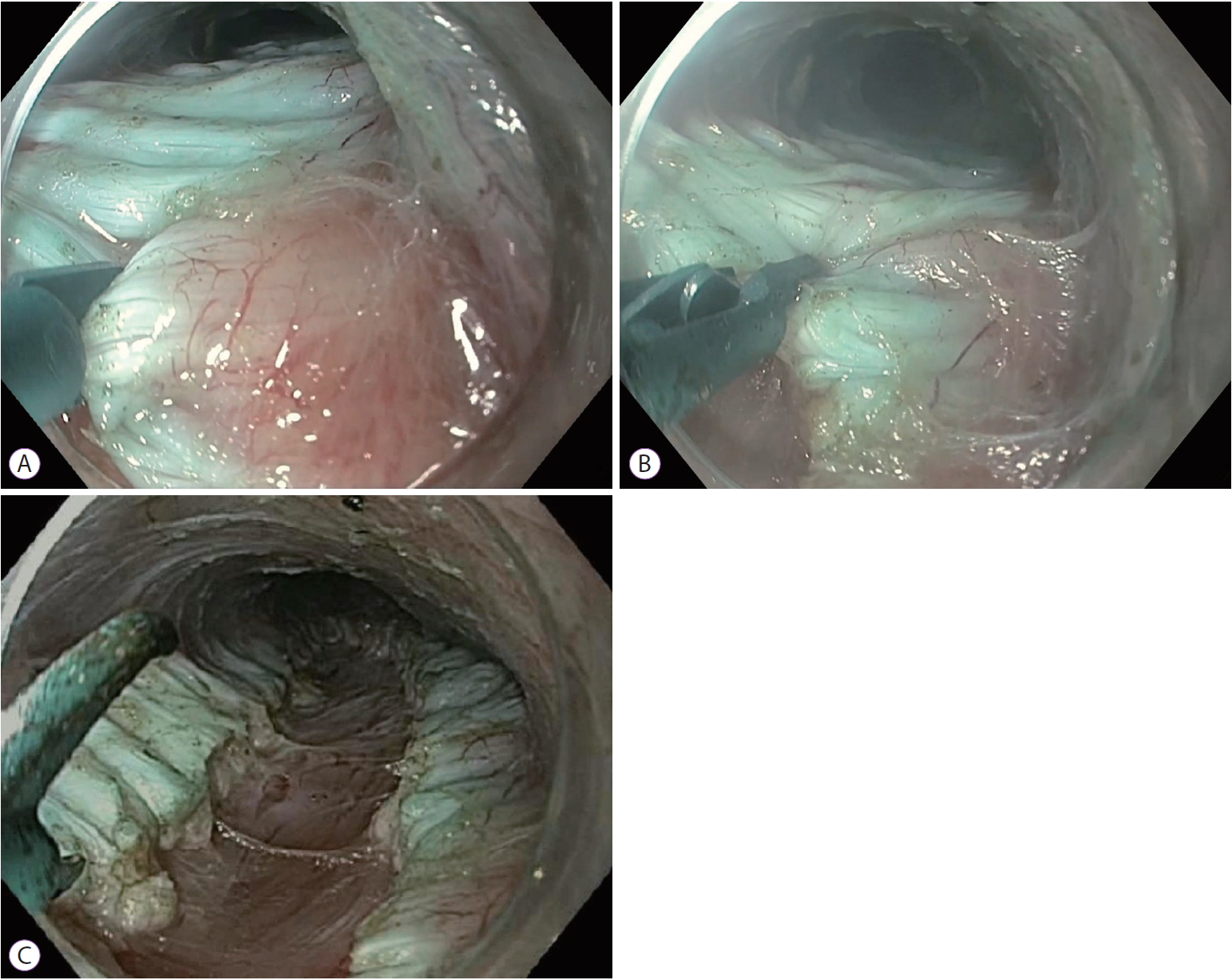
First, the internal circular muscle bundle at approximately 2 cm distal to the mucosal entry was cut using EES (Endocut [Effect 2, Cut Duration 2, Cut Interval 2]) until the external longitudinal muscle bundle was exposed (Fig. 2). Then, selective internal circular myotomy was performed. Possible blood vessels were preemptively cauterized using the EES with Soft Coag mode (effect 5, 50 W) before cutting the muscle fibers. The myotomy was then continued step by step distally until it extended approximately 2 cm distal to the gastroesophageal junction (GEJ) (Fig. 3). After completion of the myotomy, the endoscope was reinserted into the esophagus to confirm smooth passage through the GEJ (Supplementary video 1).
Outcome parameters, efficacy, and safety
All patients were scheduled for follow-up visits at 1, 3, and 6 months after the POEM procedure. The primary outcome of this study was clinical success, defined as a 3-month post-procedure Eckardt score of Ōēż3. The secondary outcomes were technical success, defined as successful completion of the myotomy, and treatment-related adverse events, separated into mild, moderate, or severe events, adapted from previous American Society of Gastrointestinal Endoscopy (ASGE) recommendations [5]. Mild complications were defined as those that required post-procedure medical consultation or unplanned prolongation of hospital stay for Ōēż3 nights. Moderate complications were defined as those that need additional monitoring but required a hospital stay of only 4ŌĆō10 nights and/or an intensive care unit (ICU) admission of 1 night. Severe complications were defined as those that were potentially life-threatening, requiring a hospital stay of >10 nights and/or ICU monitoring of >1 night, and/or requiring surgical or re-intervention for adverse events.
RESULTS
Patient baseline characteristics
Fifteen patients with normal foregut anatomy underwent POEM with EES knife for myotomy and were included in our analysis. The patientsŌĆÖ characteristics are listed in Table 1. The patientsŌĆÖ mean age was 51┬▒19.4 years (range, 29ŌĆō84 years), mean body mass index was 28┬▒8.9 kg/m2, and mean Charlson Comorbidity Index was 2.1┬▒2.9 (range, 0ŌĆō8). Six of the fifteen patients (40%) had type 1 achalasia, six (40%) had type 2 achalasia, one (6.7%) had type 3 achalasia, one had an achalasia diagnosis not otherwise specified (6.7%), and one had esophagogastric junction outflow obstruction (6.7%). Twelve of the fifteen patients (80%) received alternative therapy prior to POEM, including balloon dilation (5/15 patients, 33.3%), pneumatic dilation (4/15 patients, 26.7%), and/or botulinum toxin injection (6/15 patients, 40%). None of the patients had history of Heller myotomy or POEM procedure.
Procedure details
Fourteen of the fifteen (93.3%) myotomy procedures were performed in the posterior location, and all were selective partial-thickness myotomy procedures. Fourteen of the fifteen (93.3%) myotomies were closed with endoscopic clips (range, 4ŌĆō9 clips), and one of the fifteen (6.7%) was closed with endoscopic suturing. Given that many other centers use an endoscopic suturing device for closure, we tested this in one of our earlier cases; however, it was our preference to perform all other cases with endoscopic clips. The mean length of myotomy was 11.6┬▒3.7 cm, with a mean tunnel length of 13.2┬▒3.3 cm. The mean length of procedure was 84┬▒29 minutes.
Primary outcome
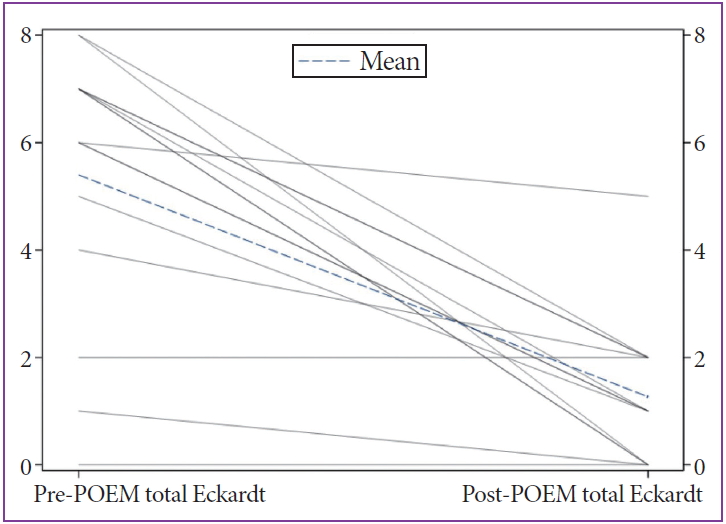
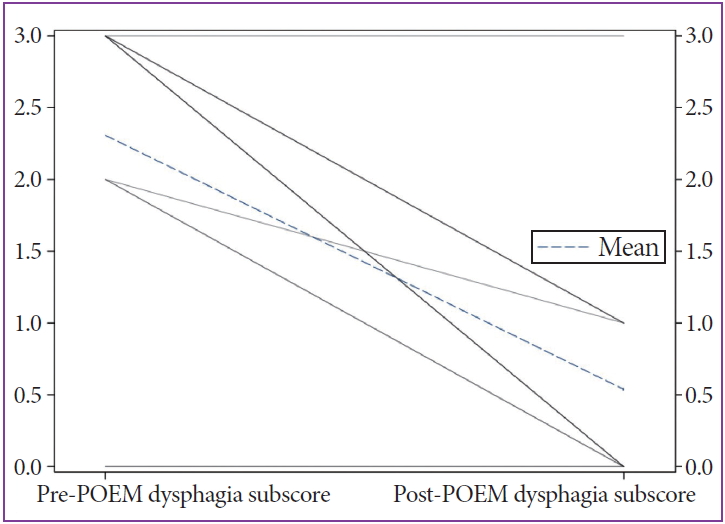
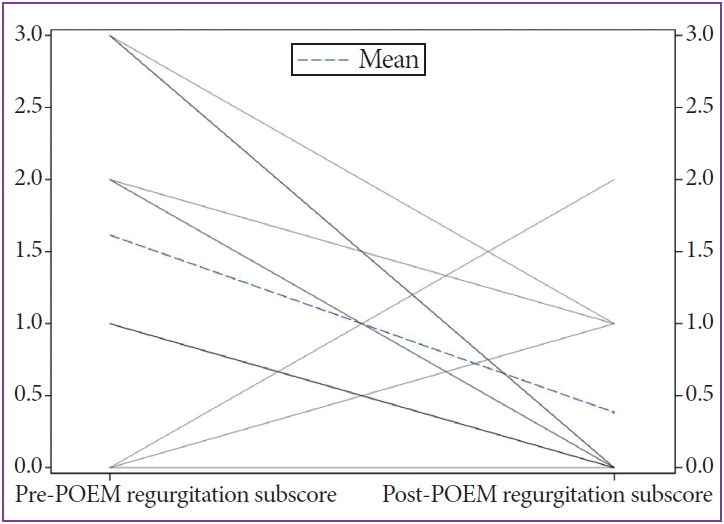
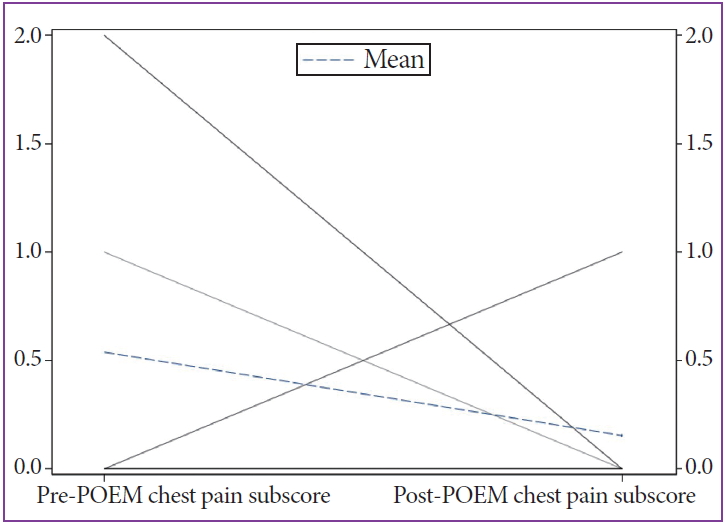
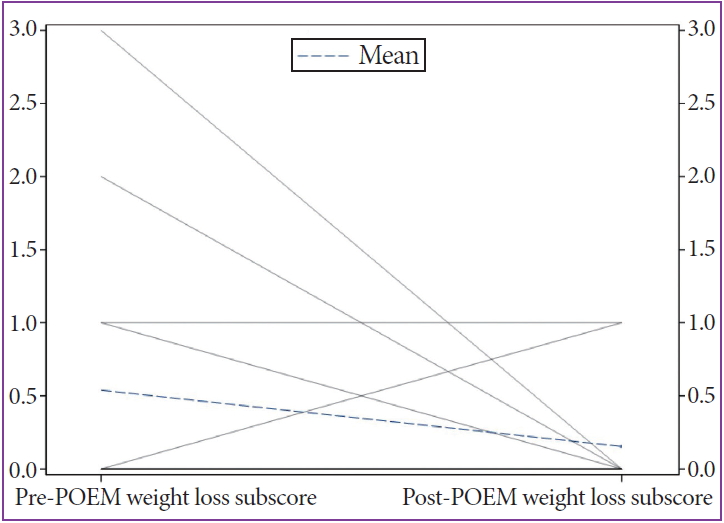
POEM was clinically successful in fourteen of the fifteen patients (93.3%) at 3-month follow-up. The mean pre-Eckardt score was 5.4┬▒2.5, and the mean post-Eckardt score was 1.3 ┬▒1.3, with a mean improvement of 4.1 ┬▒2.7 (pŌēż0.0001; Fig. 4). On Eckardt sub-score analysis, there was a statistically significant improvement in dysphagia (pre-POEM: 2.4┬▒1.1 vs. post-POEM: 0.5 ┬▒0.8, mean improvement 1.8 ┬▒1.2, p=0.0001; Fig. 5) and regurgitation (pre-POEM: 1.7┬▒1.2 vs. post-POEM: 0.3┬▒0.6, mean improvement 1.2┬▒1.5, p=0.0136; Fig. 6), but not chest pain (pre-POEM: 0.6┬▒0.9 vs. post-POEM: 0.2┬▒0.4, mean improvement 0.4┬▒1.0, p=0.2087; Fig. 7) or weight loss (pre-POEM: 0.5┬▒1.0 vs. post-POEM: 0.1┬▒0.3, mean improvement 0.4┬▒1.0, p=0.2087; Fig. 8).
Secondary outcomes
Myotomy was technically successful in all fifteen patients (100%). All patients were admitted to the hospital for observation following the procedure. The mean length of hospital stay post-procedure was 1.8 ┬▒2.4 days. Seven of the fifteen patients (46.7%) did not experience any treatment-related adverse events. Six patients (40%) experienced a mild adverse event, and two (13.3%) experienced a moderate adverse event. None of the patients experienced a severe adverse event (Table 2). The most common treatment-related adverse events were post-procedure pain requiring medical team evaluation in the immediate 24ŌĆō48 hours after the procedure (4/15 patients, 26.7%) and symptomatic reflux requiring >8 weeks of PPI therapy and/or additional over-the-counter medications (4/15 patients, 26.7%). One patient (6.7%) experienced a capnoperitoneum that required placement of an angiocatheter for decompression but did not experience any further complication nor hemodynamic instability. Two patients (13.3%) experienced post-procedure pulmonary instability. Of them, one required intubation for laryngeal edema, while the second experienced hypercarbia due to oversedation, but did not require intubation. None of the patients required blood transfusion, chest tube placement, or enteral nutrition.
DISCUSSION
In 2010, Inoue et al. first reported POEM as a safe and effective treatment option for the treatment of achalasia [3]. Since that time, multiple other retrospective and prospective trials have reported on the efficacy and safety of POEM [1,6-24]. Although the steps of the procedure are generally the same worldwide, there is some variability with regard to the equipment used to perform POEM [1,2]. In the previous years, the two knives that were used by all POEM operators were the triangle tip (TT) knife (Olympus) and the T-type hybrid knife (Erbe) [25]. The conventional knife had been the TT knife. However, some endoscopists prefer the hybrid knife as its usage is associated with shorter operative time, lower bleeding rate, and lower frequency of usage of coagulation forceps [10,25]. Tang et al. conducted a case-control analysis in 31 achalasia patients who underwent POEM using the hybrid knife and matched them by age, gender, symptom duration, American Society of Anesthesiologists (ASA) Class, Eckardt score, Chicago Classification of achalasia, and LES pressure to 36 patients who underwent POEM using the TT knife [1]. This group confirmed that the use of the hybrid knife decreased the procedure time, decreased the mean frequency of device exchanges, and the mean frequency of coagulation forceps use [1]. Additionally, they demonstrated no significant difference in the intraoperative or postoperative complications between the two groups [1].
In recent years, a novel scissor-type knife has been approved for use in the United States. The EES device was initially developed by Honma et al. in 2010 for endoscopic submucosal dissection (ESD) [26,27]. These knives have a curved, insulated tip with an internal cutting mechanism that allows the endoscopist to keep the proper dissecting layer and prevent unexpected muscular layer injuries during submucosal dissection [26]. Furthermore, Yamashina et al. demonstrated in a single-center phase II trial that the use of the scissor-type knife significantly improved the traineesŌĆÖ self-completion rates for colorectal ESD, without an increase in procedure time or adverse events [28]. Thus, given the stability and ease of use of the device, it allows for safe handling by both expert level clinicians and fellowship trainees [28,29]. Although previous studies have investigated the role of EES device in ESD, no original studies have evaluated the efficacy and safety of the device in POEM. In addition to the improved accuracy and precision for dissection, as well as the improved safety in training fellows, the EES device also provides hemostasis without the need for device exchanges. In our study, we investigated the technical and clinical efficacy, as well as the safety of EES device in POEM at an academic institution with a fellowship training program.
We demonstrated a 100% technical success rate of myotomy (15/15 patients) and a clinical success rate of 93% (14/15 patients), which is comparable to those of previous studies [1,30]. The patient in whom we did not achieve clinical success had a previous history of lung adenocarcinoma. She previously underwent surgical resection, chemotherapy, and radiation therapy, and had higher risk of disease recurrence. Although the patientŌĆÖs manometry results were possibly consistent with type 1 achalasia, the report also indicated that there was absence of contractility, which was evidenced by the setting of malignancy and/or a paraneoplastic process (i.e., secondary achalasia). Secondary achalasia in the setting of lung cancer has been previously described [31]. In contrast to primary achalasia in which various treatment options, including POEM, are available, the management of secondary achalasia generally involves treatment of the underlying cause. Although some theories suggest that POEM is less likely to succeed in patients with secondary achalasia, this needs to be further explored.
There was a statistically significant decline in the pre- and post-POEM Eckardt scores 5.4┬▒2.5 and 1.3┬▒1.3, respectively, mean improvement: 4.1┬▒2.7 (pŌēż0.0001). On sub-group analysis, there was a statistically significant improvement in dysphagia (p=0.0001) and regurgitation (p=0.0136). Although we did not observe a statistically significant improvement in chest pain or weight loss, these symptoms did not predominate in the pre-POEM assessment in our patient cohort; thus, there was less room for improvement in the post-POEM scores.
Notably, gastroenterology fellows participated in the myotomy in each procedure. As mentioned previously, given the stability and ease of use of the device, it allows for safe handling by both expert level clinicians and fellowship trainees [28,29], and similar outcomes were observed in our POEM cohort. While using the EES device, fellows can grasp the inner circular muscle prior to the incision. Thus, the fellow and attending physician can verbalize agreement in the location of the device prior to the next cut, which improves accuracy and safety of each step as the myotomy progresses distally toward the stomach. In addition, the EES device can be used for empiric vessel sealing and hemostasis, which precludes the need to exchange devices for similar treatment. These are not possible with the needle-knife devices, the unprotected tip of which can often result in inadvertent mucosal injury, arterial bleeding, or full-thickness myotomy especially when performed by trainees. Thus, the use of EES device likely increases the safety of the device over more conventional techniques.
Additionally, to further increase safety and efficacy with trainee involvement, we used two attachment caps and two endoscopic knives to perform each POEM procedure. The combination of the tapered tip cap and needle-type knife facilitates safe entry to the submucosal space and effective submucosal tunneling. By contrast, the EES device did not appear to be useful for the submucosal tunneling, due to the narrow working space of the tunnel. The transition to a combination of the regular cap and EES device allowed us to safely and selectively perform the endoscopic myotomy as described. However, the use of more endoscopic tools and devices can be a disadvantage to the use of the EES device for myotomy. Hence, future studies should investigate the cost effectiveness of the use of these multiple devices; however, given the 100% technical success rate and lack of adverse events, our technique may be useful in the ongoing education of trainees despite the potential increase in cost. A second potential disadvantage for use of EES for myotomy is that the use of multiple devices may also increase procedure time. Although our mean procedure time of 84┬▒29 minutes is comparable to that of previous studies [32], it appears slightly longer than other published data. Li et al. reported a mean operative time of 66.7 minutes in 373 POEM procedures [33], while Li et al. reported a median operative time of 45 minutes [34]. However, the Endoflip device was used in three of the fifteen procedures, and we are unfortunately unable to delineate the time spent solely on the POEM procedure; thus, our POEM procedure times for these cases are falsely elevated as we cannot specify the exact time spent on the POEM itself. There was also a learning curve associated with our technique, as these were the first fifteen procedures performed by our endoscopists. Thus, further comparative studies on procedure time are necessary to elucidate whether the use of multiple devices causes a statistically significant prolongation of the POEM procedure.
While eight of the fifteen patients (53%) included in this analysis experienced a treatment-related adverse event, most were either mild (40%), requiring no additional hospital monitoring or procedures, or moderate (13.3%). None of the patients experienced severe adverse events, which led to life-threatening scenarios or led to prolonged hospitalization or re-admission. One potential advantage of the use of EES, as specified above, is that it may reduce muscle damage due to more precise control of the device during myotomy. We only had one patient with capnoperitoneum requiring decompression, and none developed clinically significant pneumomediastinum, pneumothorax, or perforation, or required enteral nutrition. Four patients (26.7%) experienced inadequate pain control post-procedure. One prior study evaluating 234 patients post-POEM cited that 8.4%ŌĆō12.6% of patients had severe postoperative pain (defined as requiring narcotic administration) following POEM [8]. Thus, our results might indicate a higher than expected rate of post-procedure pain; however, our results are limited by the small sample size. Without a formalized definition of post-procedure pain, further follow-up data are needed to clarify the significance of this result. Four patients (26.7%) also experienced symptomatic reflux that required prolonged (>standard 8 weeks) PPI therapy and/or additional over-the-counter antacid medications. Our results are comparable to those of previous data, including a systematic review and meta-analysis in which Repici and colleagues demonstrated a pooled rate of reflux symptoms of 19% (95% confidence interval, 15.7%ŌĆō22.8%) after POEM [35]. Although two patients experienced pulmonary instability post-POEM, both were unrelated to myotomy. One had laryngeal edema due to intubation, while the other had sedation-related hypercarbia, which ultimately resolved without intervention.
Shimizu et al. recently published the results of four patients who underwent POEM with the use of EES; all four procedures were successful, and Shimizu group also deemed it to be a feasible and safe device to use for this procedure [36]. However, to our knowledge, this is the first original study to investigate the clinical efficacy and safety of the use of EES for myotomy in POEM. However, our study has several limitations. As with all retrospective and non-randomized studies, it is subject to bias. Additionally, our sample size is relatively small with short-term follow-up.
In conclusion, this study demonstrated the technical and clinical efficacy, and an excellent safety profile of EES when used to perform a selective myotomy in POEM in the treatment of achalasia. Additionally, this appears to be an effective tool for safely training fellows how to perform the myotomy technique.