INTRODUCTION
Crohn's disease (CD) is a chronic disorder characterized by segmental and transmural inflammation that can affect the entire gastrointestinal tract. Approximately half of patients with CD develop stricturing or penetrating complications within 10 years of diagnosis.1 In the presence of chronic and severe inflammation, as is seen in CD, mesenchymal cells accumulate in the area of the defect and secrete excessive extracellular matrix components to repair tissue damage, resulting in a reduction in the diameter of the lumen and obstruction.2,3 Fistulizing disease is often found in conjunction with stricture, probably due to the progression of disease in regions of full-thickness bowel wall inflammation in a high-pressure region upstream of an underlying stenosis.4,5 The most common locations of clinically apparent strictures are the ileum and ileocolic region, presumably due to the smaller diameter of the ileum relative to the colon.6,7
Up to 75% of patients with CD require surgery during their lifetime, with an overall surgical recurrence risk of 36%.8,9 Extensive small bowel disease or multiple surgeries can result in short bowel syndrome.10 The main indications for surgery are enteric stricture or obstruction.9 According to the Vienna and Montreal classifications, stricturing behaviour is defined as the occurrence of constant luminal narrowing, demonstrated by radiologic, endoscopic, or surgical examination, combined with pre-stenotic dilatation and/or obstructive signs or symptoms without evidence of penetrating disease.11,12 Clinical symptoms are not highly correlated with the presence and severity of small bowel strictures on cross-sectional imaging or endoscopy.13 The management of fibrotic strictures includes medical treatment, surgical resection, or bowel length preserving procedures such as strictureplasty and endoscopic balloon dilatation (EBD). Early resection in ileocecal stricturing CD was found to be associated with longer clinical remission than prolonged medical treatment14-16 and 50% of symptomatic small-bowel stenosis treated with anti-TNF╬▒ will require surgical resection within four years.17 In the last two decades, EBD has emerged as a reasonable treatment option for short strictures (length <5 cm) accessible with an endoscope, with a technical success of 86% to 95%, major complication rate of 2% to 10% and long-term clinical efficacy of 58% to 70%. EBD delays the need for surgery, reduces the risk of short bowel syndrome, and has a lower rate of complications than surgery. About 40% of patients need two or more EBDs, and ultimately 43% need surgery, within a mean period of 15 months.18-20 To avoid this high risk of recurrence, other endoscopic modalities have been evaluated, such as stent insertion, needle-knife stricturotomy, and intralesional steroid or anti-TNF╬▒ injection; however, these cannot be recommended for routine practice given limited evidence.
Endoscopic metallic stents have been successfully used for strictures in other conditions, such as esophageal and colonic malignancies21 or anastomotic stenosis.22 Japanese authors first proposed the use of self-expandable metallic stents (SEMS), which allow a persistent effect overtime with a longer dilatation of the stenosis than with EBD.23 The insertion of self-expanding stents in CD strictures was first studied in single case reports and case series to delay the time to surgical resection,24-27 with a high technical and clinical success but also a high rate of complications (63%), and overall migrations of fully covered stents placed and maintained in situ in the long-term. Interestingly, recent studies have suggested the use of partially covered stents and their retrieval after a short period (seven days).25 The aim of this study was to systematically review the available evidence in terms of efficacy and safety of the use of stents in stricturing CD.
METHODS
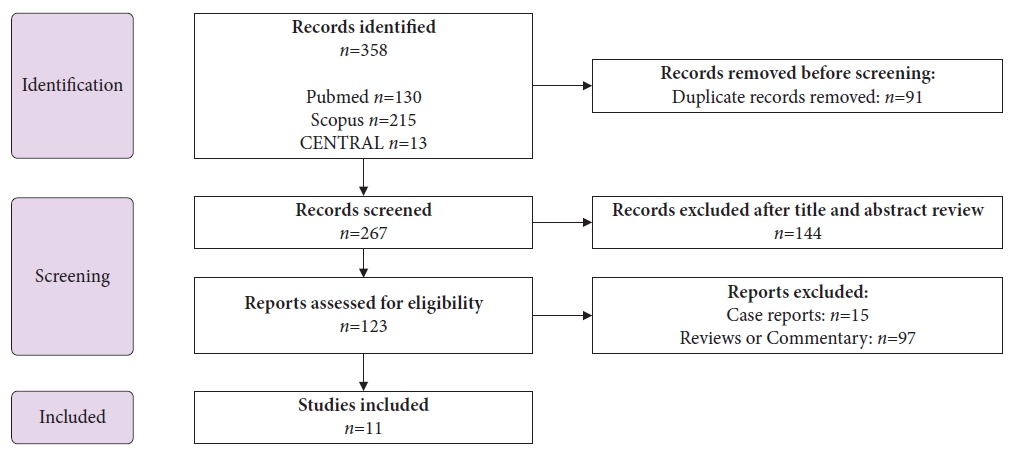
This systematic review was performed following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.28 We used a predetermined protocol (PROSPERO; no. CRD42022308033, April 2022). A systematic electronic literature search was conducted using the PubMed, Scopus, and CENTRAL databases. The final study was performed in November 2022, with no restrictions. The keywords used in the research process were: ŌĆ£CrohnŌĆÖs diseaseŌĆØ or ŌĆ£inflammato┬Łry bowel diseaseŌĆØ; ŌĆ£obstructionŌĆØ, ŌĆ£stenosis", or ŌĆ£stricture"; and ŌĆ£SEMS", ŌĆ£stent", or ŌĆ£self-expandable metallic stentŌĆØ. The search was supplemented with the bibliographic section of each article and other published reviews. The articles were independently scanned for eligibility by two reviewers (GBS and RL) (Fig. 1).
The inclusion criteria were as follows: (1) patients with CD undergoing colic, ileocolic, or ileal stenting due to anastomotic strictures, that is, post-surgical, or no anastomotic strictures, namely de novo strictures occurring in non-operated patients as a result of chronic transmural inflammation in the natural history of CD; and (2) randomized controlled trial (RCT), prospective or retrospective studies. The exclusion criteria were as follows: (1) patients with causes of obstruction other than CD; (2) patients with upper gastrointestinal stenosis; and (3) case reports.
The primary outcomes were: (1) technical success; (2) short-term efficacy (relief of obstructive symptoms immediately after stenting); (3) long-term efficacy (relief of obstructive symptoms within 1 year or at the last follow-up); (4) complication and major complication rates; and (5) the need for surgical or endoscopic intervention due to recurrence of obstruction. Complications were considered as medical problems that occur during or after a procedure, caused by the procedure itself, and characterized by pain, perforation, bleeding, reobstruction, or stent migration. Major complications were defined as the need for hospitalization, surgical, or endoscopic intervention, not considering asymptomatic migrations. The recurrence of obstruction per se was not determined directly to avoid heterogeneity of data due to the type, duration, or severity of symptoms, but was determined indirectly by analyzing the need for surgical or endoscopic intervention.
The secondary outcomes were the safety and efficacy of partially covered stents with scheduled retrieval after seven days compared to other types of stenting.
RESULTS
Baseline characteristics
Eleven studies were considered for this review: two were prospective,24,27 two were randomized control trials comparing stenting with EBD,30,31 six were retrospective 25,26,32-35 and one was both prospective and retrospective (85%)36 (Table 2).24-27,30-36
A total of 173 patients with CD were observed, with a mean number of 16 patients (range, 4ŌĆō46) per study; 47% were female. The mean age of the patients at the time of stenting was 47 years (range, 43ŌĆō54 years). The mean duration of CD was 22 years (range, 11ŌĆō46 years). Each patient underwent a single stent placement. In all studies, the clinical indication for stenting was the presence of obstructive symptoms, and five studies also considered refractoriness to medical therapy and/or endoscopic dilatation.25,26,32,33,35 Attar et al.27 and Loras et al.32 used the CD obstructive symptom scale to define intensity and duration of symptoms. The main contraindications to stenting were length of the stricture >5 or 6 cm, and multiple, inflammatory, or fistulizing strictures, and the need for urgent surgery and inflammatory stenosis were also reported as contraindications in two studies.27,34 Disease activity at the time of stenting according to a clinical or endoscopic score was reported only in Loras et al.32 Overall, 87% of patients had undergone previous surgery and 78% had undergone at least one previous EBD. The mean time between the last surgery and stenting was 11.7 years.25-27 The mean length of the stricture was 3.4 cm (range, 2.7ŌĆō4.8 cm), and 64% of strictures were anastomotic, 93% of which were ileocolic, while 84% of de novo stenosis were localized in the colon. At the time of stenting, 48% of the patients were receiving biologic therapy (with or without concomitant immunosuppressants) and 10% were receiving steroid therapy. Mucosal biopsy of the stricture to rule out malignancy was never mentioned, probably because stenosis had already been studied when EBD was performed (before stenting).
Stenting technique
The type of stent used was biodegradable in two studies24,33 and metallic in the other nine; partially covered stents (Hanarostent) were used in four studies,25,30,34,36 fully or partially covered stents (Hanarostent, Niti-S colonic stent, Microtech) were used in four studies,27,31,32,35 and uncovered stents (Wallstent/Wallflex) were used in one study.26 The biodegradable stents were placed via an overtube, and metallic stents were placed through an endoscope. All procedures were performed under fluoroscopic guidance. The mean length of the stents used was 7.5 cm (range, 6ŌĆō8 cm). Stent retrieval was scheduled after seven days in four studies,25,30,34,36 with successful extraction in all patients. In the study by Attar et al.,27 stent extraction was scheduled after 28 days, but only 1/11 patients had planned stent extraction and disappearance of obstructive symptoms. In the RCT by Loras et al.,31 the time for stent removal was set at 4 weeks, but in 97% of patients, the stent migrated after a median time of 2 days (interquartile range, 2ŌĆō7). Biodegradable stents were expected to ensure integrity and radial force for 6-8 weeks before degradation.33 In two studies, metallic stents were maintained for a mean duration of 28 days (range, 1ŌĆō112 days) and 28 months (range, 3 weeksŌĆō109 months), respectively.26,32
The mean time of the stenting procedure was reported by Loras et al.31 to be 42 minutes. Conscious sedation was used in two studies,24,26 deep sedation in two studies,27,32 and general anesthesia in two studies,25,36 while sedation was not reported in five studies. EBD during the stenting procedure was possible in all studies, although it was not reported in five studies.25,31,34-36 Stenting was performed in an inpatient27 or outpatient setting,26,30 when reported.
Outcomes
Technical success of stenting was reported in all studies but was defined in only three cases as stent deployment across the entire stricture length. Mean percentage of technical success was 95% (range, 80%ŌĆō100%). The reported reasons for failure were angulation of the colon, making it impossible to deliver the biodegradable stent through the overtube,24,33 or cannulation of the stricture using a guidewire under fluoroscopy.27
Short-term efficacy, which was considered as relief of obstructive symptoms immediately after stenting, was 100% for the successfully inserted stents. Long-term efficacy, which was considered as resolution of obstructive symptoms within 1 year or at the last follow-up, was 56% (range, 25%ŌĆō90%). The mean follow-up period was 27 months (range, 6ŌĆō69 months). Thirty-eight percent (range, 10%ŌĆō75%) of patients required further endoscopic or surgical interventions within a mean period of 5.4 months. Surgical interventions accounted for 20% of cases at the end of follow-up, with a mean interval from stenting of 3 weeks in Levine et al.26 and Attar et al.27 and 14 months in the study by Loras et al.,32 in which more endoscopic interventions were performed before surgery. In addition, 5% of patients required surgery due to stent-related complications. The mean complication rate was 56% (range, 15%ŌĆō97%) and consisted of pain (15%), migrations (29%), obstruction (12%), and others (1%): one patient had a perforation after distal migration of the stent that was trapped in a sigmoidal diverticulum, and there was one case of bleeding after stent extraction that required hospitalization without further interventions.30 The major complication rate, that is, the need for hospitalization, or surgical or endoscopic intervention, was 27% (range, 0%ŌĆō75%), not including asymptomatic migrations. Seven cases of upstream stent migration required EBD or surgical intervention for extraction.27,31,36 Four of the 10 patients with stent migrations in the study of Loras et al.32 (mean time to migration: one month) had no recurrence (mean follow-up of 5.5 months), whereas six needed further endoscopic or surgical interventions after a mean of 10.4 months. Das et al.34 reported three patients with stent migrations without the need of further intervention. In the study of Attar et al.,27 four out of eight patients with stent migration (mean time: five days) did not require any treatment within a mean time to clinical recurrence of obstruction of 29 months, while four patients underwent further interventions after a mean time of 16 days. Twenty of the 75 stents left in situ over time needed to be removed: five stents (25%) required surgical intervention and the others were successfully retrieved endoscopically. In contrast, all 80 stents with scheduled retrieval were successfully removed; only three stents required specific endoscopic removal methods (EBD).
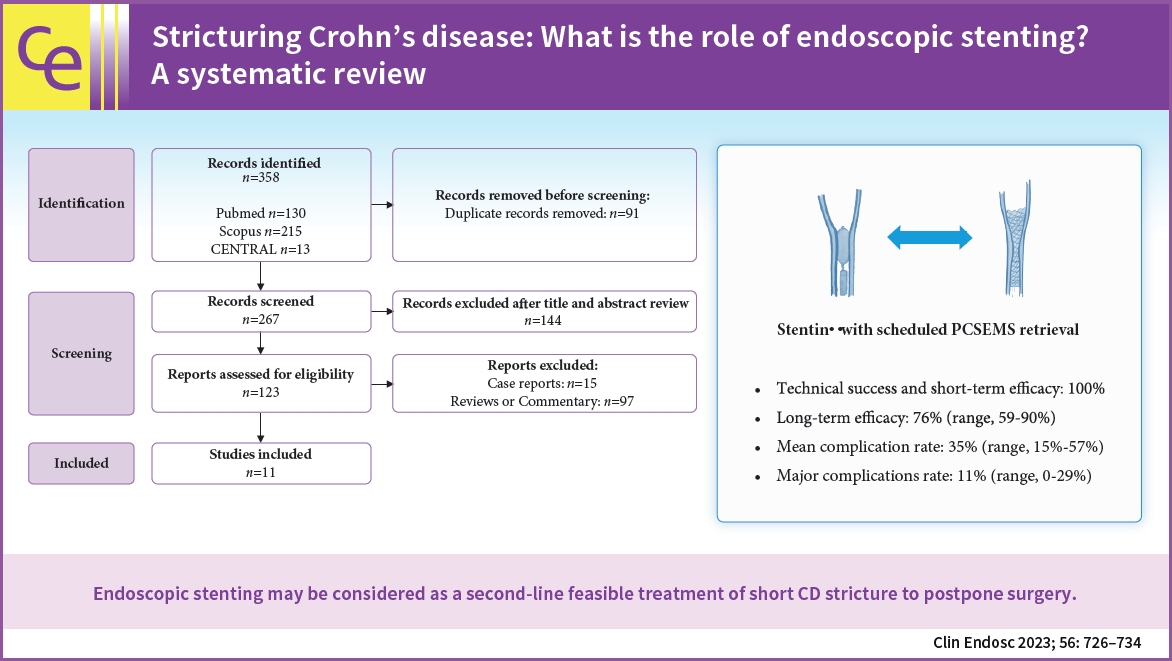
Considering only the four studies with scheduled stent retrieval after seven days (Table 3),25,30,34,36 the technical success and short-term efficacy was 100% in all studies.25,30,34,36 The long-term efficacy was 76% (range, 59%ŌĆō90%), the need for further interventions was 20% (range, 10%ŌĆō41%) with a mean time of 11 months (range, 10ŌĆō12 months), and the need for surgery was 8% (0%ŌĆō17%), never due to stent-related complications (mean follow-up of 40 months). The mean complication rate was 35% (range, 15%ŌĆō57%), 30% pain and 5% migrations, and the major complication rate was 11% (range, 0%ŌĆō29%), with the same percentage of pain requiring stent removal and stent proximal migration with the need for EBD to retrieve it.
DISCUSSION
Evidence of the efficacy and safety of stenting for CD strictures is limited. Only a few case reports and small case series have been published since 1997. Our review showed that endoscopic stenting for CD strictures had a technical success rate of 95%, short-term efficacy of 100%, and long-term efficacy of 56%, with a complication rate of 56% and a major complication rate of 27%; 27% of patients undergoing stenting required subsequent surgery.
These results are comparable with those of EBD, which has a reported technical success of 86% to 95%, and a short-term and long-term efficacy of 70% to 80% and 58% to 70%, respectively; however, a major complication rate of 2% to 10% and surgery requirement of 42% to 75% were also reported.19-21 In our review, approximately 80% of stented patients had a previous EBD, and 87% had undergone surgery, suggesting that most strictures were long-standing and of a more fibrotic nature. However, in recent studies reporting the use of partially covered antimigratory stents with scheduled stent retrieval after seven days, the rate of major complications was 11%, no patient underwent surgery due to complications, and only 20% needed further interventions.25,30,34,36 This approach seems to guarantee a lower risk of symptom recurrence and complications than the use of fully covered stents left in situ over time.
The RCT by Loras et al.31 concluded that EBD was more effective and more cost-effective than SEMS (41 and 39 patients in total, success rate 80% and 51%, severe adverse events 2% and 3%, average cost Ōé¼1365 and Ōé¼1923 per patient, respectively); however, fully covered SEMS were used, and in all but one patient, stent migration occurred within a mean period of 2 days. Two case series (16 patients) also analyzed the use of biodegradable stents with discouraging results in long-term efficacy due to mucosal hypergranulation reaction or stent collapse, resulting in reobstruction.24,33
Interestingly, we reported only one case of perforation, whereas most studies observed a higher perforation rate, especially in benign rather than malignant strictures (18.4% vs. 7.5%). However, most benign colorectal strictures considered in these studies were diverticular and involved more active inflammation, which weakened the bowel wall, whereas anastomotic stenoses and long-standing CrohnŌĆÖs strictures are typically associated with fibrotic enteral wall thickening.37
The limitations of this review were the retrospective nature of most of the studies, the small population sizes, and the heterogeneity of the studies. Therefore, comparable data did not emerge, and performing a meta-analysis, as recently published by Chandan et al.,38 could be misleading. We found a high technical success rate and short-term efficacy, which could be attributed to the selection bias in retrospective studies. An unequivocal definition of stricture and obstructive signs was not reported in these studies, and clinical or technical success, when defined, varied between studies. Furthermore, the meta-analytic estimates of different stenting modalities for type and duration were not methodologically correct or useful.
In conclusion, the heterogeneity and retrospective nature of most of the studies prevented any firm conclusions. The four selected studies based on the new use of antimigratory partially covered stents with scheduled stent retrieval after seven days, thus reducing the risk of complications of a stent left in situ over time, allow only a suggestion of the role of the stent in CD strictures as a feasible second-line treatment. The possible role of the stent may postpone the surgery in short strictures of <5 cm, in which EBD was not effective. However, larger prospective head-to-head studies are required to better understand the role of stenting as an alternative or additional treatment to EBD in CD.