INTRODUCTION
Malignant gastric outlet obstruction (GOO) refers to a condition in which there is a blockage or narrowing at the point where the stomach empties its contents into the small intestine by primary malignant tumors or metastatic diseases. Symptoms caused by malignant GOO include nausea, vomiting, early satiety, abdominal pain or discomfort, loss of appetite, and weight loss. Dehydration, electrolyte imbalances, malnutrition, or gastroparesis can also be complicated.1,2 To resolve and manage clinical problems complicated by malignant GOO, several treatment options have been applied clinically. Surgical gastrojejunostomy (SGJ) was initially applied for the resolution of malignant GOO. Then, gastroduodenal stenting (GDS) with self-expandable metallic stents (SEMS) was popular as an alternative option for malignant GOO. Recently, endoscopic ultrasound-guided gastrojejunostomy (EUS-GJ) was introduced with the rapid development of interventional endoscopic ultrasound.3-5 Herein, we reviewed clinical outcomes of endoscopic stenting (ES) such as GDS and EUS-GJ and compared them with SGJ for the treatment of malignant GOO.
THE CLASSIFICATION OF TREATMENT MODALITIES FOR PALLIATION OF MALIGNANT GOO
The treatment modalities for the resolution of symptomatic malignant GOO are shown in Figure 1. Palliative approaches for malignant GOO are divided into ES and SGJ. ES includes GDS and endoscopic gastrojejunostomy. GDS is the conventional endoscopic placement of SEMS at the obstruction site in malignant GOO. Endoscopic gastrojejunostomy has been performed in the following three ways: endoscopic ultrasound (EUS-GJ), forward-viewing endoscopy (endoscopic magnetic gastrojejunostomy), and the natural orifice transluminal endoscopic surgery (NOTES) approach. In the following sections, we will focus on GDS and SGJ, which are currently being actively implemented clinically; and EUS-GJ, which has been started relatively recently but is being tried by several groups.
GASTRODUODENAL STENTING
The SGJ, which involved creating a connection between the stomach and the jejunum, had been selected for a conventional treatment of malignant GOO. However, this procedure is invasive and carries a higher risk of complications.6-10 Gastroduodenal stent placement using a SEMS (Fig. 2) has shown comparable clinical outcomes and safety for palliation of obstructive symptoms complicated by malignant GOO.11-14 Initially, SEMS in the early developmental stages of the procedure were uncovered. The uncovered SEMS inevitably developed tumor ingrowth over time, which covered SEMS were developed to overcome. However, because the SEMS in the early developmental stages had high axial force with poor conformability, covered SEMS resulted in frequent stent migration.15 The covered stents used in esophageal obstruction are full-covered types, but covered stents for malignant GOO are mostly partially covered and uncovered at both ends to reduce migration. The clinical studies about the efficacy of SEMS on malignant GOO are summarized in Table 1.15-27 Previous studies reported stent malfunction due to stent migration in 0ŌĆō8.3% of patients with malignant gastroduodenal obstruction with uncovered stents16,19,24 and 8.8% to 28% of patients with malignant GOO with covered stents.28-30 A meta-analysis of 61 articles analyzing the clinical results of GDS for malignant GOO published from January 2015 to February 2021 showed that technical and clinical successes were 99.4% (95% confidence interval [CI], 98.9%ŌĆō99.8ŌĆŖ%) and 88.9% (95% CI, 86.7%ŌĆō90.9%). The recurrence rates were 28.7% (95% CI, 19.7%ŌĆō38.6%), and the reintervention rate was 20.3% (95% CI, 16.9%ŌĆō23.9%).6
THE COMPARISON OF CLINICAL EFFICACY AND SAFETY BETWEEN COVERED AND UNCOVERED SEMS
According to the results of a meta-analysis, which analyzed studies on the clinical performance and safety of covered and uncovered SEMS in malignant GOO, technical and clinical success were not statistically different between the two SEMS (odds ratio [OR], 0.69; 95% CI, 0.21ŌĆō2.3 and OR ,1.1; 95% CI, 0.76ŌĆō1.61, respectively). Stent survival, defined as the time between stent deployment and stent dysfunction was higher in covered than in uncovered SEMS (hazard ratio, 0.68; 95% CI, 0.48ŌĆō0.96). Covered SEMS were associated with higher stent migration (OR, 4.28; 95% CI, 2.79ŌĆō6.57). Uncovered SEMS were associated with a higher rate of stent occlusion (OR, 0.34; 95% CI, 2.79ŌĆō6.57). However, there were no differences in terms of overall adverse events, reintervention, and dysfunction rates. In addition, patient survival was similar in covered and uncovered stent groups (hazard ratio, 0.96; 95% CI, 0.75ŌĆō1.23).31
Thus far, four randomized, controlled studies in which clinical efficacy and safety of endoscopic placement of covered vs. uncovered SEMS were sufficiently demonstrated, have been conducted worldwide, three in Korea and one in Japan. In terms of clinical efficacy, the two randomized trials showed similar results in stent malfunction caused by stent migration and restenosis in covered and uncovered SEMS.15,16 However, in the two other studies, the clinical outcomes of covered SEMS were better than those of uncovered SEMS.17,18
When looking at the results of these meta-analyses and comparative studies, it seems difficult to draw any conclusions about which type of stent should be chosen as a first option between covered and uncovered SEMS. However, we must consider the following several points. Firstly, it is highly likely that the performance of the stents used in previous studies was not the same. The manufacturing methods and stent designs are different in the various companies that produce SEMS and they could cause differences in the clinical performance of SEMS. Secondly, the causative diseases of malignant GOO were different in the prior studies. The patient cohorts of many studies consisted of various cancers, such as pancreatic, gastric, duodenal, bile duct, gallbladder, and metastatic cancers, and some conducted studies on patients with a single cancer type, such as gastric cancer.16,32,33 Thirdly, the cancer progression and the clinical disease severity during the follow-up period were different among studies. These factors could affect the clinical outcome and prognosis of SEMS placement in malignant GOO. In addition, whether chemotherapy is administered can also affect the clinical outcomes of SEMS placement. Several retrospective studies have shown that chemotherapy is associated with prolonged uncovered stent patency in patients with malignant pyloric obstruction.34-36 A long time-to-progression and first-line chemotherapy were substantial protective factors against re-stenosis.37 Chemotherapy has been associated with stent migration.15,35,36 In a study conducted by Lim et al.,15 the rate of stent migration in the covered SEMS group was higher in the patients who underwent chemotherapy than in those who did not undergo chemotherapy. However, in most studies, it is difficult to find statistically significant results analyzing the influence of chemotherapy on SEMS placed endoscopically.
Innovations in the design of SEMS should be made to improve clinical efficacy in malignant GOO. Two of the above-mentioned randomized, controlled trials indicated a triple-layered design for covered SEMS; clinical outcomes in the covered SEMS group were superior to the uncovered SEMS group. This warrants attention. It is speculated that this innovative design substantially influenced the decrease in the rate of stent migration. The superiority of triple-layered, covered SEMS must be validated in more clinical prospective studies.
ENDOSCOPIC GASTROJEJUNOSTOMY
Since endoscopic gastrojejunostomy has advantages of both SGJ and endoscopic metal stent placement, such as a short length of anastomosis and less invasiveness, endoscopic gastrojejunostomy may be an ideal treatment for malignant GOO. Endoscopic approaches can be divided into two: (1) using flexible forward-view endoscopy, and (2) using endoscopic ultrasound (Fig. 3).
Using flexible forward-view endoscopy
Studies with animal models on endoscopic gastrojejunostomy began to be reported in the early 1990s and early 2000s.38-40 Later, endoscopic magnetic gastrojejunostomy41-43 and the NOTES approach44,45 were suggested. However, all of these were small-scale studies with insufficient progress to merit successful implementation in a clinical situation, for the following reasons. Firstly, flexible forward-view endoscopy is very difficult to perform with only a conventional endoscope. Secondly, in the case of the magnetic method, it takes approximately 10 days after magnet installation until a gastroenteric fistula is formed. Thirdly, the safety of the procedure has not been sufficiently proven. Therefore, the concept of endoscopic gastrojejunostomy has evolved into an approach using endoscopic ultrasound.
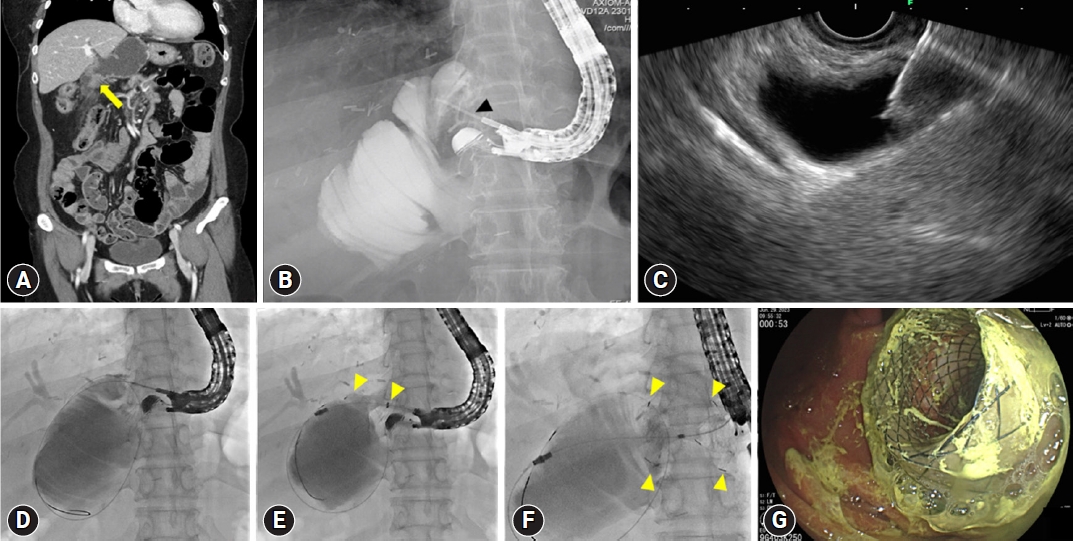
Using endoscopic ultrasound
Endoscopic ultrasound-guided drainage therapy has been consistently published since the early 2000s.41 EUS-GJ is usually proceeded with the following steps. (1) The patient is placed under conscious sedation or general anesthesia to ensure comfort during the procedure. (2) An endoscope with an integrated ultrasound probe is inserted into the patient's mouth and guided down the esophagus into the stomach. (3) Under ultrasound guidance, a needle is advanced through the stomach wall and into the jejunum, creating a tract. (4) A guidewire is then threaded through the needle and into the jejunum. (5) Over the guidewire, a stent or a balloon catheter is placed to create a connection (anastomosis) between the stomach and the jejunum. (6) The stent is deployed, expanding and securing the connection. (7) The endoscope is withdrawn, and the procedure is completed.
Recent studies and case reports have shown comparable efficacy and safety of EUS-GJ in managing malignant GOO, contributing to its increasing adoption as a minimally invasive therapeutic option.3,46-55 There have also been studies on ES in cases of both malignant biliary obstruction and GOO. The extent of GOO can be divided into three types: (1) invasion of only the duodenal bulb; (2) invasion to the second part of the duodenum, to the main papilla; and (3) invasion of the third part of the duodenum, without the involvement of the papilla. According to a study analyzing the results of 11 studies examining the treatment results of endoscopic treatment in patients with both malignant biliary and GOO, stenting was performed on the GOO site in 10 studies, and EUS-GJ was used to treat malignant GOO in one study.56 Endoscopic ultrasound-guided biliary drainage (EUS-BD) therapies therapies were performed at the same time or within seven days. The clinical outcomes of EUS-BD were very good (a mean technical success of 96.4%; 95% CI, 92.2%ŌĆō99.0%) and a mean clinical success of 85.0% (95% CI, 68.0%ŌĆō96.3%). And, clinical success of duodenal stenting and EUS-GJ for malignant GOO was 90% and 100%, respectively.56 Therefore, when malignant biliary obstruction and malignant GOO occur at the same time, GOO is not a problem at all even if it is solved by conventional ES or relatively recently introduced EUS-GJ. However, it is still too early to say that EUS-GJ can be applied as a primary treatment of choice for malignant GOO. A randomized trial comparing the method with conventional SEMS placement should be conducted to verify the efficacy and safety of EUS-GJ.
COMPARISON OF CLINICAL OUTCOMES OF GDS, EUS-GJ, AND SGJ
In a meta-analysis comparing the clinical results of GDS, EUS-GJ, and SGJ in the studies published between January 2015 and February 2021, the technical success was lowest in EUS-GJ (95.3% [95% CI, 89.3%ŌĆō98.9%] in EUS-GJ, 99.4 % [95% CI, 98.9%ŌĆō99.8%] in GDS, and 99.9% [95% CI, 99.5%ŌĆō100%] in SGJ, p=0.0048). In addition, the recurrence and reintervention rates of GDS were higher than those of EUS-GJ and SGJ; the recurrence rates were 28.7% (95% CI, 19.7%ŌĆō38.6%) in GDS, 4.0% (95% CI, 0%ŌĆō15.0%) in EUS-GJ, and 16.9% (95% CI, 11.6%ŌĆō23.0%) in SGJ, respectively (p=0.0036), and the reintervention rates were 20.3% (95% CI, 16.9%ŌĆō23.9%) in GDS, 11.2% (95% CI, 4.9%ŌĆō19.6%) in EUS-GJ, and 12.6% (95% CI, 6.6%ŌĆō20.1%) in SGJ, respectively (p=0.041).
In terms of safety, overall procedural complications were similar (GDS, 18.7% vs. EUS-GE, 21.9% vs. surgical GJ, 23.8%; p=0.32). Although, estimated bleeding rates were similar between GDS and EUS-GJ: 1.7% (95% CI, 0.9%ŌĆō2.7%) and 2.9% (95% CI, 0.2%ŌĆō8.6%), respectively (p=0.999), the bleeding rate for GDS was lower than that for SGJ (5.2%; 95% CI, 3.2%ŌĆō7.5%; p=0.0033 for pairwise comparison).6
There have only been small reports on the comparison between SGJ and GDS.8,9,11,57-59 In a multicenter-based, randomized, controlled trial performed by Jeurnink et al.,11 SGJ was associated with better long-term outcomes. In the study, the majority of enrolled patients had pancreatic cancer and GDS was compared with bypass surgery. Approximately half of the 77 initially enrolled patients refused to participate in the randomization, which was described as a limitation of the study.
SELECTION OF TREATMENT MODALITIES OF GDS, EUS-GJ, AND SGJ IN MALIGNANT GOO
A multidisciplinary, team-based decision-making process including gastroenterologists, surgeons, and oncologists is important to select the most appropriate and personalized treatment option for each patient with malignant GOO. The team has to assess the individual patient's overall health status, tumor characteristics, and potential risks and benefits of each treatment option.
GDS is advantageous in several aspects. It is a minimally invasive procedure, avoiding the need for open surgery. It is associated with shorter procedure time, reduced hospital stay, and faster recovery compared to SGJ. SEMS can be easily removed or exchanged if needed. GDS carries a lower risk of complications compared to SGJ.60,61 GDS can preclude the potential risks associated with open surgery, such as general anesthesia, surgical wound infections, postoperative pain, and longer hospital stay.
However, GDS is not always feasible and is preferred to SGJ. If the sites of GOO show extensive or complex obstruction or an attempt to place a SEMS is unsuccessful, in these cases, SGJ may be preferred. Tumor-related factors should also be considered. If the tumor is bulky, invasive, or associated with a high risk of tumor ingrowth, SGJ could provide more durable relief of obstruction compared to ES. Finally, consideration of clinical factors such as patient preferences for SGJ, life expectancy, anticipated treatment course, and quality of life could inform the decision of SGJ over GDS.
According to a recent guideline released by the American Society for Gastrointestinal Endoscopy, GDS is preferentially recommended in patients who are poor surgical candidates with short life expectancy (<6 months) and want early resumption of oral diet and discharge from the facility. Conversely, SGJ is preferentially recommended in patients with a life expectancy of >6 months and a good performance status.62
More clinical data are required on the circumstances in which EUS-GJ is preferentially selected for patients with malignant GOO. If the procedure is successful, the rates of restenosis and reintervention are lower than those of GDS. However, there is still doubt about the feasibility and safety of the procedure. More randomized clinical trials are needed to validate the feasibility and safety of EUS-GJ.
CONCLUSIONS
Since the early 2000s, ES has shown excellent clinical outcomes and safety, affirming that it can replace surgical bypass. In terms of the difficulty of the endoscopic procedure, ES can be performed if the gastrointestinal endoscopist is familiar with the operation of conventional endoscopic devices, such that clinical implementation of the procedure has succeeded worldwide. More recently, EUS-GJ has shown remarkable clinical results, although only a few studies have been reported.63,64 However, there are still procedural difficulties to be solved and safety issues to determine. Ultimately, non-inferiority compared to conventional endoscopic stent treatment should be demonstrated in a randomized, prospective clinical study, such that the endoscopic ultrasound-based approach can be applied more often in clinical situations. Although ES has optimistic clinical outcomes, there are some potential future directions for ES. Innovation in stent designs has to be attempted to enhance clinical efficacy and reduce complications. Research on anti-migration mechanisms, drug elution to the surface of SEMS in techniques to prevent tumor ingrowth, and modifications of stent design to promote better luminal patency should be done. Advanced endoscopic technology may lead to the development of more minimally invasive approaches for ES. Robotic-assisted endoscopic platforms or endoscopic suturing devices may have a crucial role in improving clinical outcomes and widening the indications of endoscopy while reducing invasiveness. To prove the possibility of these innovative approaches, prospective and randomized clinical trials are warranted.