CME for
KSGE members
Chang and Park: A rare colonoscopic finding in a renal transplant recipient
Quiz
A 50-year-old male visited Severance Hospital for colonoscopy screening without any specific symptoms. He received an allogeneic renal transplantation 20 years prior and had no associated complications. He had undergone a colonoscopy three years previously, and there were no abnormal findings. Physical examination revealed no remarkable findings. Blood test results were within normal ranges. Colonoscopy revealed multiple whitish, flat, or slightly elevated mucosal lesions measuring 10 to 20 mm in diameter in the ascending colon. The pit pattern of these lesions was not compatible with that of typical adenomas, and forceps biopsies were preformed at each portion ( Fig. 1). Histological findings and immunostaining results for CD68 (PG-M1), are shown in Figure 2. What is the most likely diagnosis?
Answer 
The patient was diagnosed with asymptomatic colon malakoplakia, and third-generation cephalosporins were prescribed for 30 days. Colonoscopy performed after six months showed complete resolution of all lesions ( Fig. 3). Malakoplakia is a rare chronic granulomatous disease of uncertain etiology that shows a high incidence in immunocompromised patients with human immunodeficiency virus infection, malignancy, and post-organ transplantation status. 1 Though commonly seen in the urinary tract, it is also reported in other sites, including the gastrointestinal tract, pancreas, liver, lymph nodes, skin, and respiratory tract. 2 Malakoplakia is associated with dysfunctional bacterial clearance by neutrophils and macrophages, and is thus closely related to immunodeficiency. The most commonly reported microorganisms in patients with malakoplakia are Escherichia coli, Proteus, Mycobacterium tuberculosis, and Staphylococcus aureus. 3 Clinical manifestations are very diverse and not specific for this disease. 3 Endoscopic findings could be categorized as three different patterns: (1) isolated sessile/polypoid masses in the rectosigmoid colon, (2) diffuse serpiginous lesions or ulcers of the colon, (3) mass occurring in association with cancer of the colon. 4 Diagnosis can be made by histology with the presence of the large granular, eosinophilic histocytes (von Hansemann cells) and more specifically by the laminated, basophilic, targetoid inclusions (Michaelis-Gutmann bodies), which are stained with periodic acid-Schiff, Von Kossa, and Prussian blue. 2 Immunohistochemically, the cells are positive for CD68, CD163 and alpha-chymotrypsin, confirming their histiocytic nature. 1 Medical treatment strategies are based on antibiotics to eradicate microorganisms and cholinergic agonists to enhance macrophage function. 5 Rifampicin and ciprofloxacin have been used for their ability to enter the macrophage. Although their efficacy remains controversial, long-term treatments are recommended. 2
Physicians should consider malakoplakia when diverse and atypical mucosal lesions are detected on colonoscopy, particularly in immunocompromised patients.
Fig.┬Ā1.
Colonoscopy with the use of (A, B) white light and (C, D) narrow-band imaging revealed multiple whitish flat or slightly elevated mucosal lesions measured 10 to 20 mm in diameter at the ascending colon. 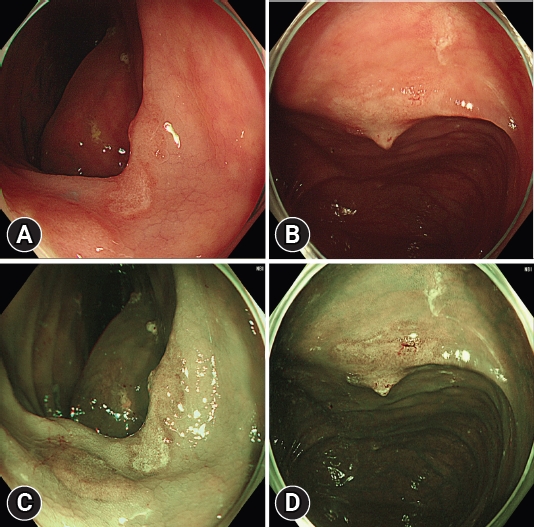
Fig.┬Ā2.
Histopathologic findings. (A) The lesions consisted predominantly of histiocytes with eosinophilic granular cytoplasm (von Hansemann cells) (arrow) (hematoxylin and eosin stain, ├Ś200). (B) The lesion was positive for CD68 (PG-M1, ├Ś400). 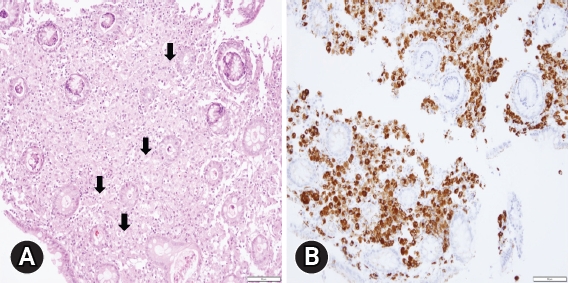
Fig.┬Ā3.
(A, B) Colonoscopy following after 6 months of antibiotics treatment shows complete resolution of all lesions. 
REFERENCES
2. Ajabnoor R, Mawardi M, Almutawa A. Colonic malakoplakia in a liver transplant recipient: a case report. Hum Pathol Case Rep 2019;18:200323.  4. Mousa OY, Corral JE, Nassar A, et al. Colonic mass and chronic diarrhea in a renal transplant patient: an uncommon case of malakoplakia: 1441. Am J Gastroenterol 2017;112:S783. S785. 5. Haq K. Malakoplakia in kidney transplant recipients. Kidney News 2023;15:10.
|
|







