
Articles
- Page Path
- HOME > Clin Endosc > Volume 53(4); 2020 > Article
- Review Endoscopic Ultrasound-Guided Fine Needle Aspiration and Endoscopic Retrograde Cholangiopancreatography-Based Tissue Sampling in Suspected Malignant Biliary Strictures: A Meta-Analysis of Same-Session Procedures
-
Diogo Turiani Hourneax de Moura1,2, Marvin Ryou1, Eduardo Guimarães Hourneaux de Moura2, Igor Braga Ribeiro2, Wanderlei Marques Bernardo2, Christopher C. Thompson1,

-
Clinical Endoscopy 2020;53(4):417-428.
DOI: https://doi.org/10.5946/ce.2019.053
Published online: November 5, 2019
1Division of Gastroenterology, Hepatology and Endoscopy, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA, USA
2Endoscopy Unit, Department of Gastroenterology, Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo, Brazil
- Correspondence: Christopher C. Thompson Division of Gastroenterology, Hepatology and Endoscopy, Brigham and Women’s Hospital, Harvard Medical School, 75 Francis St., Thorn 1404 Boston, MA 02115, USA Tel: +1-617-525-8266, Fax: +1-617-264-6342, E-mail: cthompson@hms.harvard.edu
• Received: February 21, 2019 • Revised: March 30, 2019 • Accepted: April 25, 2019
Copyright © 2020 Korean Society of Gastrointestinal Endoscopy
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Background/Aims:
- The diagnosis of biliary strictures can be challenging. There are no systematic reviews studying same-session endoscopic retrograde cholangiopancreatography (ERCP)-based tissue sampling and endoscopic ultrasound-guided fine needle aspiration (EUS-FNA) for the diagnosis of biliary strictures.
-
Methods:
- A systematic review was conducted on studies analyzing same-session EUS and ERCP for tissue diagnosis of suspected malignant biliary strictures. The primary outcome was the accuracy of each method individually compared to the two methods combined. The secondary outcome was the accuracy of each method in pancreatic and biliary etiologies. In the meta-analysis, we used Forest plots, summary receiver operating characteristic curves, and estimates of the area under the curve for intention-to-treat analysis.
-
Results:
- Of the 12,132 articles identified, six were included, resulting in a total of 497 patients analyzed. The sensitivity, specificity, positive likelihood ratio, negative likelihood ratio, and accuracy of the association between the two methods were: 86%, 98%, 12.50, 0.17, and 96.5%, respectively. For the individual analysis, the sensitivity, specificity and accuracy of EUS-FNA were 76%, 100%, and 94.5%, respectively; for ERCP-based tissue sampling, the sensitivity, specificity, and accuracy were 58%, 98%, and 78.1%, respectively. For pancreatic lesions, EUS-FNA was superior to ERCP-based tissue sampling. However, for biliary lesions, both methods had similar sensitivities.
-
Conclusions:
- Same-session EUS-FNA and ERCP-based tissue sampling is superior to either method alone in the diagnosis of suspected malignant biliary strictures. Considering these results, combination sampling should be performed when possible.
INTRODUCTION
MATERIALS AND METHODS
Search
Study selection
Data collection process
Data items
Risk of bias
Summary measures and synthesis of results
RESULTS
DISCUSSION
CONCLUSIONS
-
Conflicts of Interest: Marvin Ryou is a consultant for Olympus and Medtronic, Eduardo Guimarães Hourneaux de Moura is a consultant for Boston Scientific and Olympus, Christopher C. Thompson is consultant for Boston Scientific, Olympus and Medtronic. The other authors have no financial conflicts of interest.
-
Author Contributions
Conceptualization: Diogo Turiani Hourneax de Moura
Data curation: DTHM, Igor Braga Ribeiro
Formal analysis: Wanderlei Marques Bernardo
Methodology: DTHM, WMB, Eduardo Guimarães Hourneaux de Moura
Project administration: EGHM, WMB
Supervision: EGHM, Christopher C. Thompson
Writing-original draft: DTHM
Writing-review&editing: Marvin Ryou, CCT
NOTES
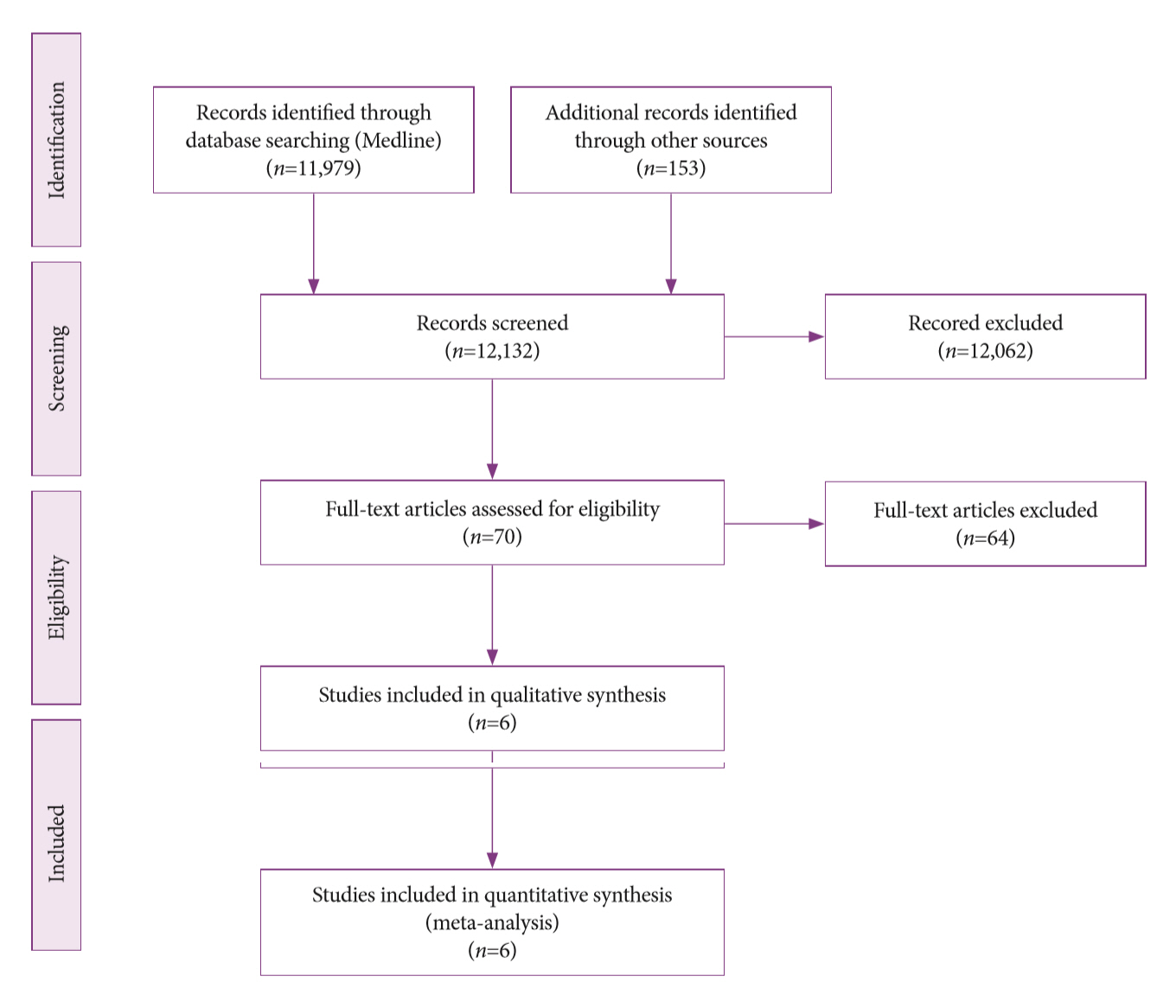
Fig. 2.Forest plots of the sensitivity, specificity, positive likelihood ratio (LR) and negative LR of the association of endoscopic ultrasound-guided fine needle aspiration and endoscopic retrograde cholangiopancreatography-based tissue sampling in the diagnosis of suspected malignant biliary strictures. CI, confidence interval.
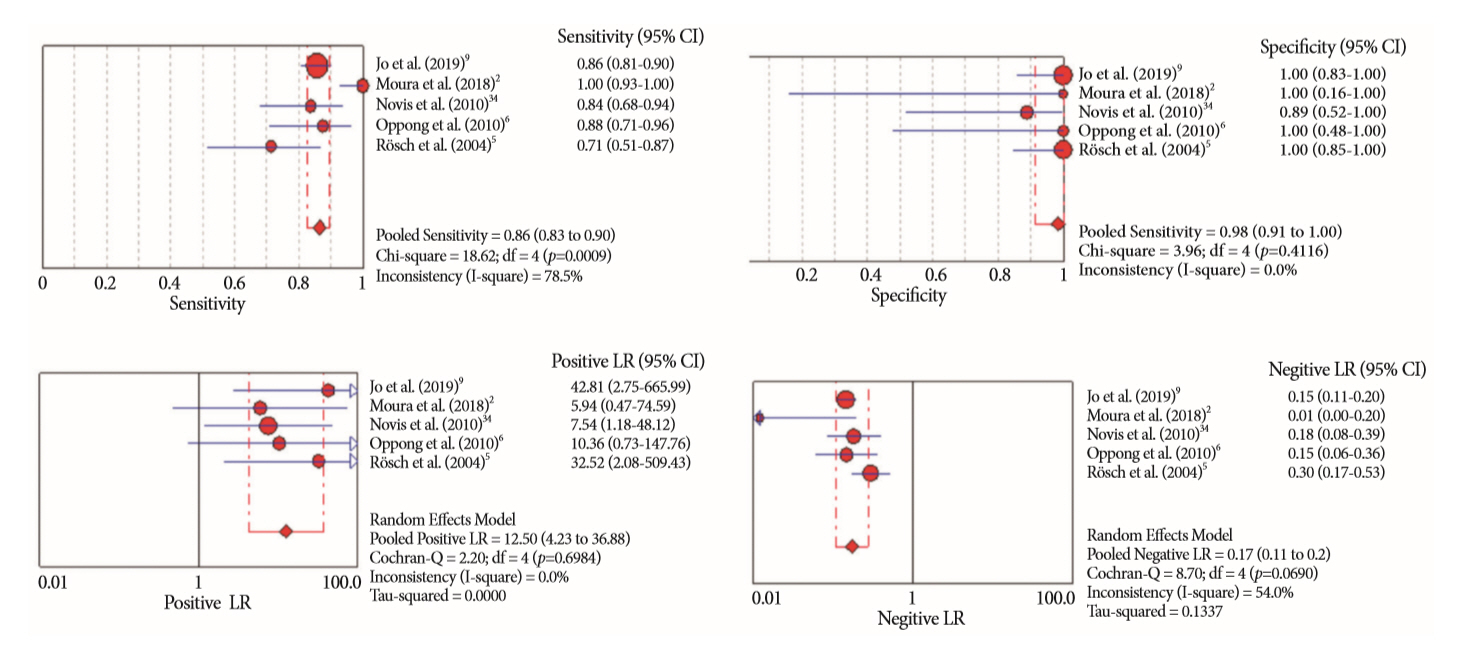
Fig. 3.Summary receiver operating characteristic (sROC) curve of the association of endoscopic ultrasound-guided fine needle aspiration and endoscopic retrograde cholangiopancreatography-based tissue sampling in the diagnosis of suspected malignant biliary strictures. AUC, area under the curve; SE, standard error.
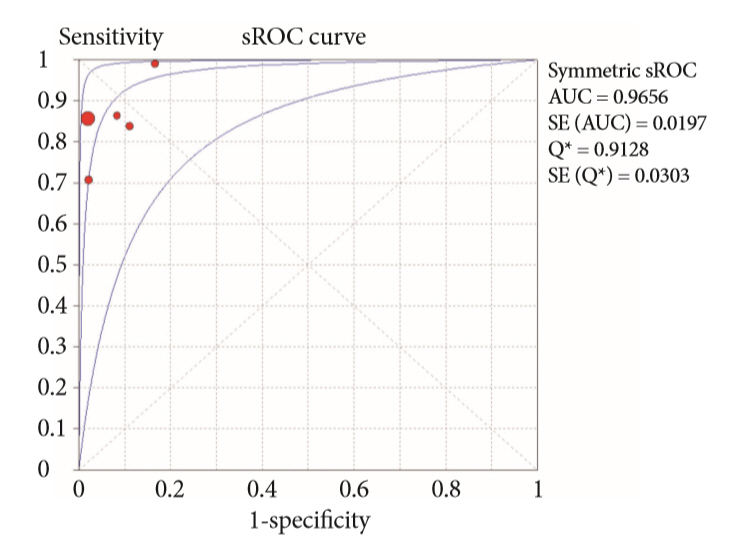
Fig. 4.Forest plots of the sensitivity, specificity, positive likelihood ratio (LR) and negative LR of endoscopic ultrasound-guided fine needle aspiration in the diagnosis of suspected malignant biliary strictures. CI, confidence interval.
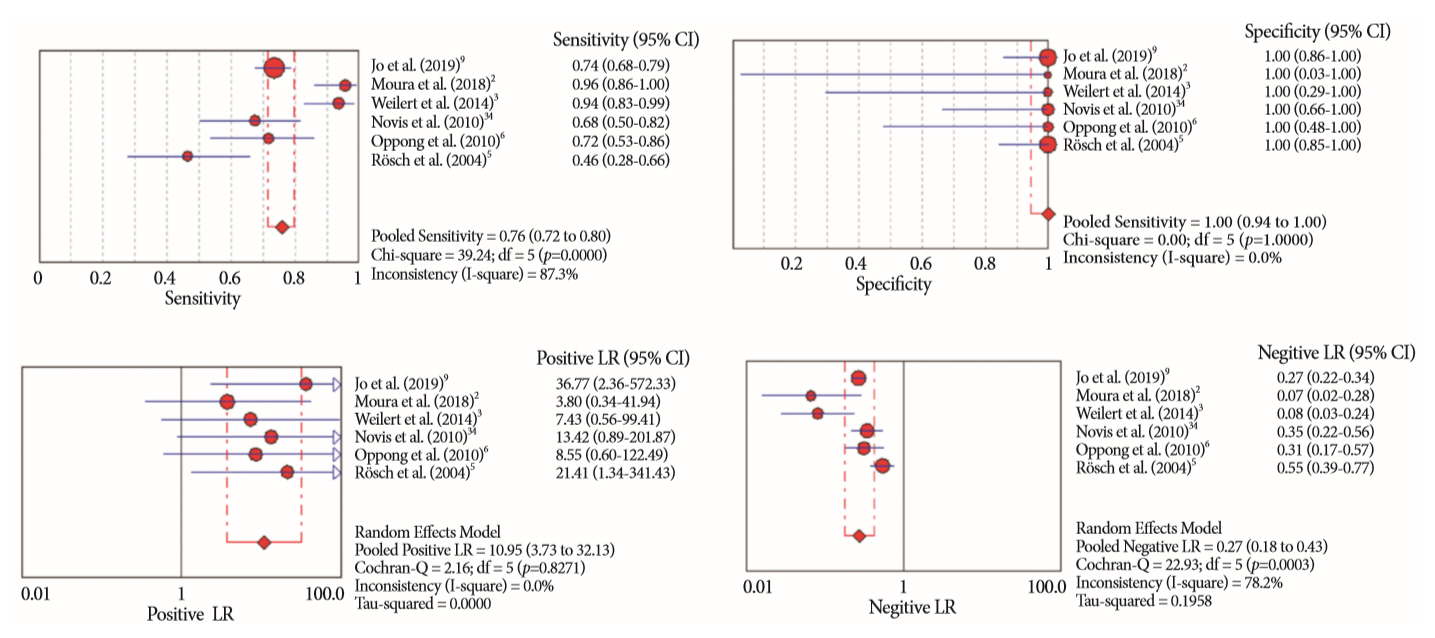
Fig. 5.Forest plots of the sensitivity, specificity, positive likelihood ratio (LR) and negative LR of endoscopic retrograde cholangiopancreatography-based tissue sampling in the diagnosis of suspected malignant biliary strictures. CI, confidence interval.
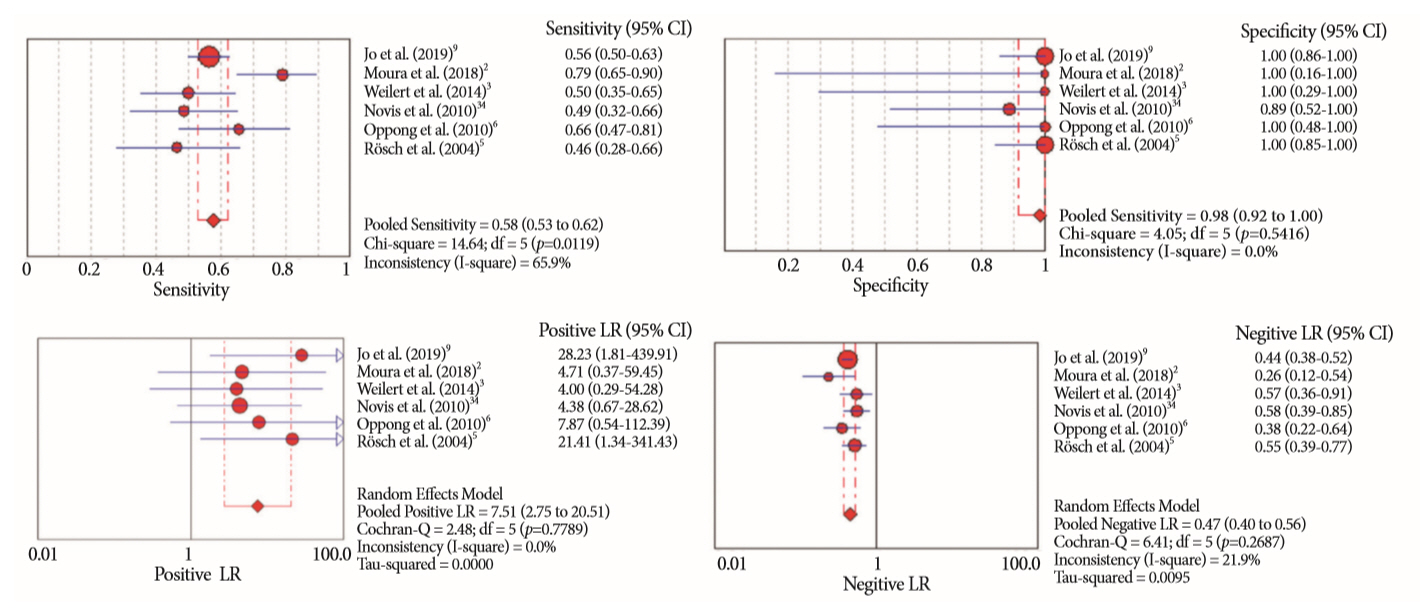
Fig. 6.Forest plots of the sensitivity, specificity, positive likelihood ratio (LR) and negative LR of endoscopic ultrasound-guided fine needle aspiration in the diagnosis of pancreatic lesion causing biliary strictures. CI, confidence interval.
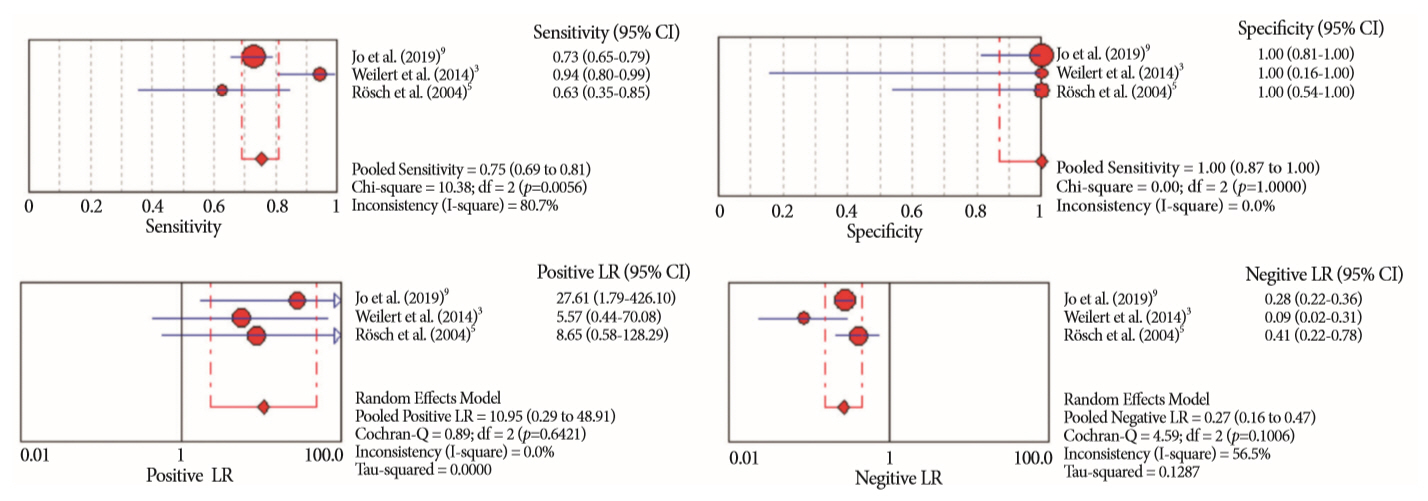
Fig. 7.Forest plots of the sensitivity, specificity, positive likelihood ratio (LR) and negative LR of endoscopic retrograde cholangiopancreatography in the diagnosis of pancreatic lesion causing biliary strictures. CI, confidence interval.
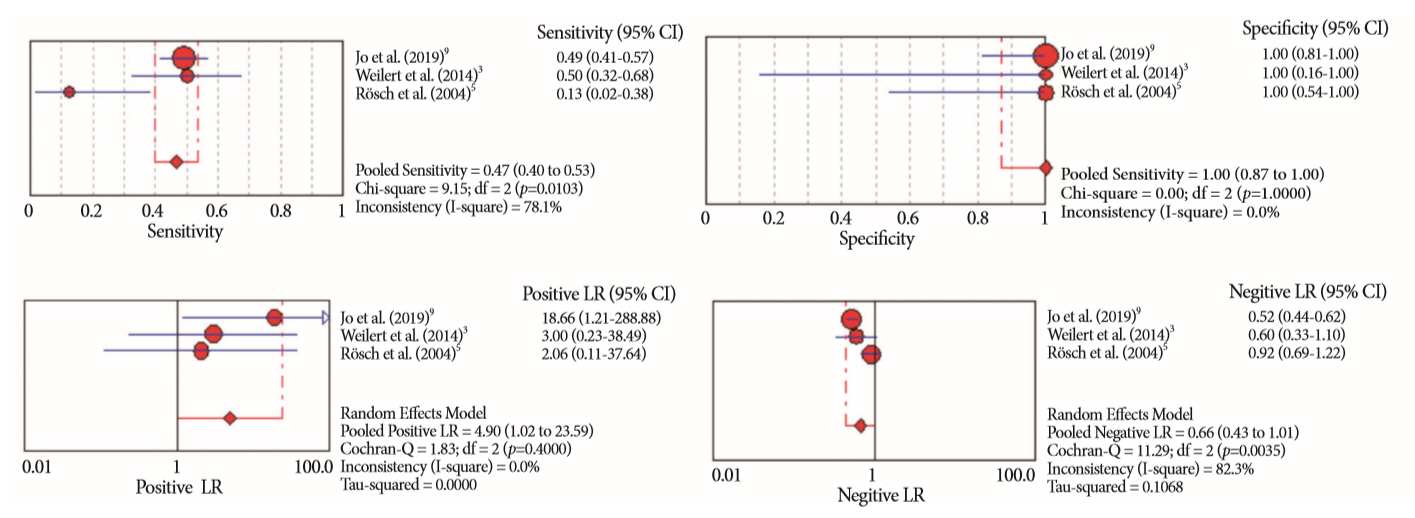
Fig. 8.Forest plots of the sensitivity, specificity, positive likelihood ratio (LR) and negative LR of endoscopic ultrasound-guided fine needle aspiration in the diagnosis of biliary lesions. CI, confidence interval.
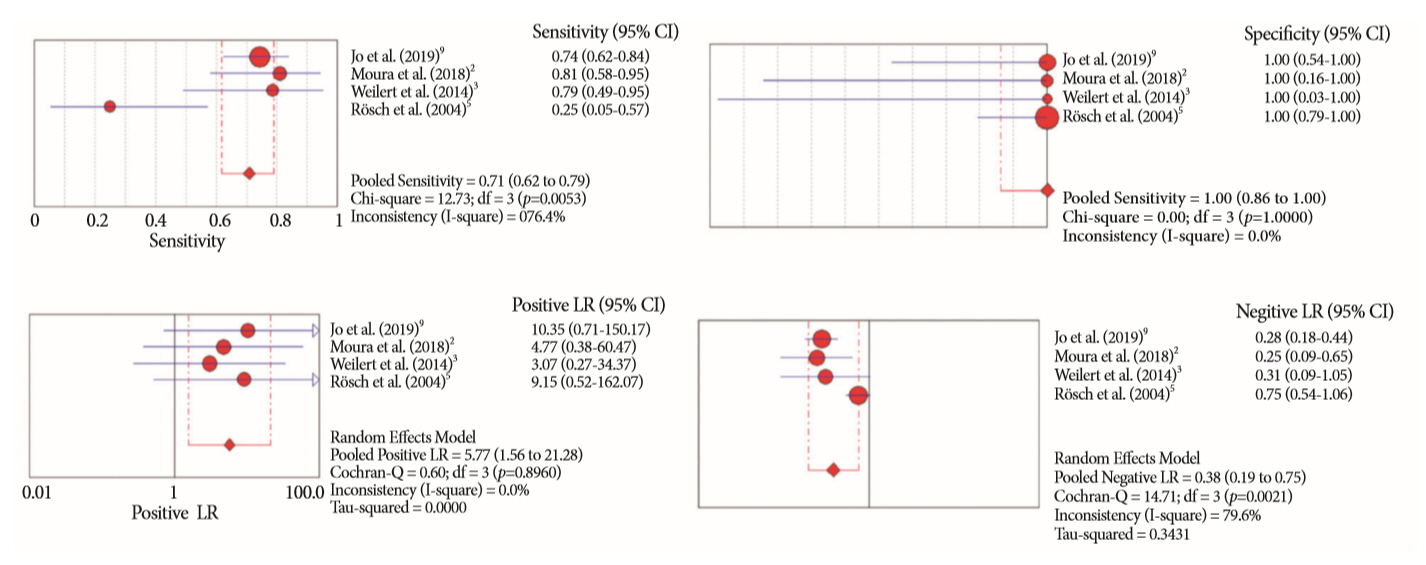
Fig. 9.Forest plots of the sensitivity, specificity, positive likelihood ratio (LR) and negative LR of endoscopic retrograde cholangiopancreatography-based tissue sampling in the diagnosis of biliary lesions. CI, confidence interval.
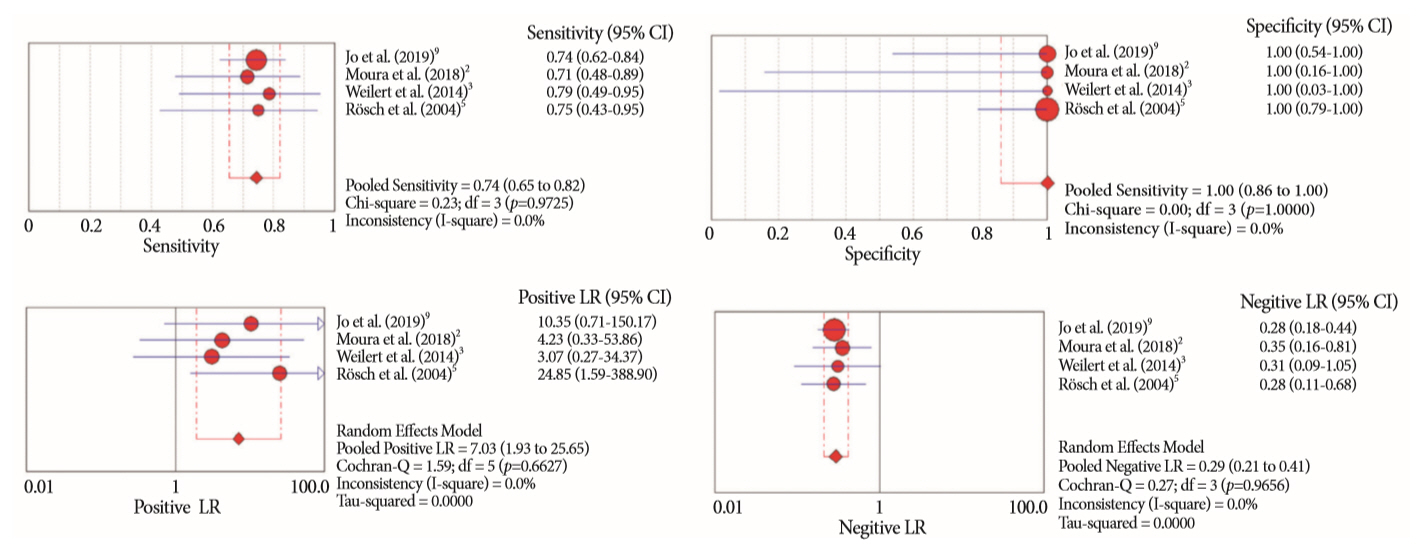
Table 1.Characteristics of Included Studies
| Study | Patients (n) | Age (yr) | Lesion size | Intervention | Gold standard | Final diagnosis |
|---|---|---|---|---|---|---|
| Jo et al. (2019) [9] | 263 | 64.6±10.5 | 26.9±11.6 mm | EUS-FNA (22 G, 25H, 20 G and 19 G): 2.7 (±1.2) passes | 1) Surgical pathology; | Malignant: 239 |
| M: 167 | 2) pathologic diagno- sis made by any tissue acquisition method; 3) follow-up (>6 mo) | - Pancreatic mass: 163 | ||||
| Design: Retrospective | F: 96 | ERCP: 3 (1–7) intraductal biopsy in 246/257 cases and cytology (via endoscopic nasobiliary drainage or brushing in all cases) | - CCA: 53 | |||
| - Gallbladder cancer: 14 | ||||||
| - Other: 9 | ||||||
| Benign: 24 | ||||||
| - Autoimmune pancreatitis: 12 | ||||||
| - Chronic pancreatitis: 5 | ||||||
| - Other: 7 | ||||||
| Moura et al. (2018) [2] | 50 | 63.08 (41–86) | 3.48±1.72 cm | EUS-FNA (22 G): 4 passes | 1) Surgical pathology; | Malignant: 48 |
| M: 24 | 2) clinical follow-up (>6 mo) | - Adenocarcinoma: 36 | ||||
| Design: Prospective | F: 26 | ERCP: 3 intraductal biopsies and 2 brush cytology | - IPMN: 4 | |||
| - Metastases: 3 | ||||||
| - Neuroendocrine tumor: 2 | ||||||
| - Adenosquamous: 1 | ||||||
| Weilert et al. (2014) [3] | 51 | 67 (42–88) | N/A | EUS-FNA (22 G or 25 G)—with ROSE | 1) Surgical findings/pathology; 2) EUS or ERCP sampling with definite evidence for malignancy; and 3) clinical follow-up (>6 mo) | Malignant: 48 |
| - Pancreatic cancer: 34 | ||||||
| Design: Prospective | ERCP: 2 to 3 intraductal biopsies and brush cytology | - CCA: 13 | ||||
| - Gallbladder cancer: 1 | ||||||
| Benign: 3 | ||||||
| - Autoimmune pancreatitis: 1 | ||||||
| - Chronic pancreatitis: 1 | ||||||
| - Autoimmune cholangiopathy: 1 | ||||||
| Novis et al. (2010) [34] | 46 | 56 (40–87) | N/A | EUS-FNA (22 G): at least 3 passes-with ROSE (by the endoscopist) | 1) Surgical pathology; 2) EUS or ERCP sampling with evidence for malignancy; and 3) clinical follow-up (>6 mo for malignance and 24 mo for benign) | Malignant: 37 |
| M: 21 | - Pancreatic cancer: 26 | |||||
| Design: Prospective | F: 25 | ERCP brush cytology | - Biliary: 11 | |||
| - Common bile duct: 8 | ||||||
| - Hilar tumors: 3 | ||||||
| Benign: 9 | ||||||
| - Chronic pancreatitis: 8 | ||||||
| - Fibrosis: 2 | ||||||
| Oppong et al. (2010) [6] | 37 | 62.4 (26–87) | N/A | EUS-FNA (22 G and 25 G): 2.7 (1–6) passes | 1) Surgical histology or other biopsy methods; | Malignant: 32 |
| - Pancreatic tumor: 29 | ||||||
| Design: Retrospective | ERCP brush cytology: at least 3 brushings | 2) any positive cytology result combined with clinical follow-up with evidence of malignancy; 3) follow-up until death or for at least two years if there was no evidence of malignancy | - Neuroendocrine tumor: 2 | |||
| - CCA: 1 | ||||||
| Benign: 5 | ||||||
| - Chronic pancreatitis: 2 | ||||||
| - Primary sclerosing cholangitis: 1 | ||||||
| - Serous cyst adenoma: 1 | ||||||
| - GIST: 1 | ||||||
| Rösch et al. (2004) [5] | 50 | N/A | N/A | EUS-FNA (22 G): at least 2 passes | 1) Surgery pathology | Malignant: 28 |
| M: 29 | ERCP: 6 intraductal biopsies and brush cytology (2 types of brush, 2 passes with each) | 2) Biopsy specimens obtained by other methods | - Pancreatic tumors: 16 | |||
| Design: Prospective | F: 21 | 3) A positive result for any tissue acquisition method being evaluated, plus clinical follow-up that provided further evidence of malignancy | - Biliary tumors: 12 (8 common bile duct and 4 hilar) | |||
| 4) Further evidence of malignancy (e.g., distant metastases) | Benign: 22 | |||||
| - Chronic pancreatitis 6 | ||||||
| 5) 6-mo follow-up | - CBD stricture: 16 (9 common bile duct and 7 hilar) |
Table 2.Quality Assessment of Diagnostic Accuracy Studies-2. Risk of Bias Across the Included Studies
| Study |
Risk of bias |
Applicability concerns |
|||||
|---|---|---|---|---|---|---|---|
| Patient selection | Index test | Reference standard | Flow and timing | Patient selection | Index test | Reference standard | |
| Jo et al. (2019) [9] |

|
|
|
|
|
|
|
| Moura et al. (2018) [2] |
|
|
|
|
|
|
|
| Weilert et al. (2014) [3] |
|
|
|
|
|
|
|
| Novis et al. (2010) [34] |
|
|
|
|
|
|
|
| Oppong et al. (2010) [6] |
|
|
|
|
|
|
|
| Rösch et al. (2004) [5] |
|
|
|
|
|
|
|
 High risk
High risk
Table 3.Summary of the Meta-Analysis Results
Table 4.Adverse Events Related to Combined Procedures of Each Included Study
| Study | Patients, n | Adverse events, n(%) | Adverse events |
|---|---|---|---|
| Jo et al. (2019) [9] | 263 | 24 (9.12) | - 8 bleedings |
| - 2 cholangitis | |||
| - 14 pancreatitis | |||
| Moura et al. (2018) [2] | 50 | 3 (6) | - 2 mild pancreatitis |
| - 1 post sphincterotomy bleeding without hemodynamic repercussion, treated endoscopically | |||
| Weilert et al. (2014) [3] | 51 | 0 | No adverse events |
| Novis et al. (2010) [34] | 46 | 5 (10.86) | - 2 cholangitis treated endoscopically |
| - 1 mild pancreatitis | |||
| - 1 biliary peritonitis. Surgical intervention was required. Patient died after surgery | |||
| - 1 mild bleeding. No intervention was required | |||
| Oppong et al. (2010) [6] | 37 | 2 (9.1) | - 1 mild pancreatitis |
| - 1 inadequate biliary drainage after procedures. Stent exchange was required | |||
| Rösch et al. (2004) [5] | 50 | 0 | No adverse events |
- 1. Korc P, Sherman S. ERCP tissue sampling. Gastrointest Endosc 2016;84:557–571.ArticlePubMed
- 2. Moura DTH, de Moura EGH, Matuguma SE, et al. EUS-FNA versus ERCP for tissue diagnosis of suspect malignant biliary strictures: a prospective comparative study. Endosc Int Open 2018;6:E769–E777.ArticlePubMedPMCPDF
- 3. Weilert F, Bhat YM, Binmoeller KF, et al. EUS-FNA is superior to ERCP-based tissue sampling in suspected malignant biliary obstruction: results of a prospective, single-blind, comparative study. Gastrointest Endosc 2014;80:97–104.ArticlePubMed
- 4. American Society for Gastrointestinal Endoscopy (ASGE) Standards of Practice Committee, Anderson MA, Appalaneni V, et al. The role of endoscopy in the evaluation and treatment of patients with biliary neoplasia. Gastrointest Endosc 2013;77:167–174.ArticlePubMed
- 5. Rösch T, Hofrichter K, Frimberger E, et al. ERCP or EUS for tissue diagnosis of biliary strictures? A prospective comparative study. Gastrointest Endosc 2004;60:390–396.ArticlePubMed
- 6. Oppong K, Raine D, Nayar M, Wadehra V, Ramakrishnan S, Charnley RM. EUS-FNA versus biliary brushings and assessment of simultaneous performance in jaundiced patients with suspected malignant obstruction. JOP 2010;11:560–567.PubMed
- 7. Butturini G, Stocken DD, Wente MN, et al. Influence of resection margins and treatment on survival in patients with pancreatic cancer: meta-analysis of randomized controlled trials. Arch Surg 2008;143:75–83; discussion 83.ArticlePubMed
- 8. Mansfield SD, Barakat O, Charnley RM, et al. Management of hilar cholangiocarcinoma in the North of England: pathology, treatment, and outcome. World J Gastroenterol 2005;11:7625–7630.ArticlePubMedPMC
- 9. Jo JH, Cho CM, Jun JH, et al. Same-session endoscopic ultrasound-guided fine needle aspiration and endoscopic retrograde cholangiopancreatography-based tissue sampling in suspected malignant biliary obstruction: a multicenter experience. J Gastroenterol Hepatol 2019;34:799–805.ArticlePubMed
- 10. Jailwala J, Fogel EL, Sherman S, et al. Triple-tissue sampling at ERCP in malignant biliary obstruction. Gastrointest Endosc 2000;51(4 Pt 1):383–390.ArticlePubMed
- 11. Shieh FK, Luong-Player A, Khara HS, et al. Improved endoscopic retrograde cholangiopancreatography brush increases diagnostic yield of malignant biliary strictures. World J Gastrointest Endosc 2014;6:312–317.ArticlePubMedPMC
- 12. Ponchon T, Gagnon P, Berger F, et al. Value of endobiliary brush cytology and biopsies for the diagnosis of malignant bile duct stenosis: results of a prospective study. Gastrointest Endosc 1995;42:565–572.ArticlePubMed
- 13. Pugliese V, Conio M, Nicolò G, Saccomanno S, Gatteschi B. Endoscopic retrograde forceps biopsy and brush cytology of biliary strictures: a prospective study. Gastrointest Endosc 1995;42:520–526.ArticlePubMed
- 14. Draganov PV, Chauhan S, Wagh MS, et al. Diagnostic accuracy of conventional and cholangioscopy-guided sampling of indeterminate biliary lesions at the time of ERCP: a prospective, long-term follow-up study. Gastrointest Endosc 2012;75:347–353.ArticlePubMed
- 15. Glasbrenner B, Ardan M, Boeck W, Preclik G, Möller P, Adler G. Prospective evaluation of brush cytology of biliary strictures during endoscopic retrograde cholangiopancreatography. Endoscopy 1999;31:712–717.ArticlePubMedPDF
- 16. Sugiyama M, Atomi Y, Wada N, Kuroda A, Muto T. Endoscopic transpapillary bile duct biopsy without sphincterotomy for diagnosing biliary strictures: a prospective comparative study with bile and brush cytology. Am J Gastroenterol 1996;91:465–467.PubMed
- 17. Farrell RJ, Jain AK, Brandwein SL, Wang H, Chuttani R, Pleskow DK. The combination of stricture dilation, endoscopic needle aspiration, and biliary brushings significantly improves diagnostic yield from malignant bile duct strictures. Gastrointest Endosc 2001;54:587–594.ArticlePubMed
- 18. Wiersema M, Lehman G, Hawes R. Improvement of diagnostic yield of brush cytology in malignant strictures by the use of supplemental tissue sampling technique. Gastrointest Endosc 1992;35:265A.
- 19. Singh H, Siddiqui AA. Endosonographic workup and preoperative biliary drainage for pancreatic cancer. Semin Oncol 2015;42:59–69.ArticlePubMed
- 20. Harinck F, Konings IC, Kluijt I, et al. A multicentre comparative prospective blinded analysis of EUS and MRI for screening of pancreatic cancer in high-risk individuals. Gut 2016;65:1505–1513.ArticlePubMed
- 21. Dewitt J, Devereaux BM, Lehman GA, Sherman S, Imperiale TF. Comparison of endoscopic ultrasound and computed tomography for the preoperative evaluation of pancreatic cancer: a systematic review. Clin Gastroenterol Hepatol 2006;4:717–725; quiz 664.ArticlePubMed
- 22. Guedes HG, Moura DTH, Duarte RB, et al. A comparison of the efficiency of 22G versus 25G needles in EUS-FNA for solid pancreatic mass assessment: a systematic review and meta-analysis. Clinics (Sao Paulo) 2018;73:e261.ArticlePubMedPMC
- 23. De Moura DT, Chacon DA, Tanigawa R, et al. Pancreatic metastases from ocular malignant melanoma: the use of endoscopic ultrasound-guided fine-needle aspiration to establish a definitive cytologic diagnosis: a case report. J Med Case Rep 2016;10:332.ArticlePubMedPMCPDF
- 24. De Moura DTH, Moura EGH, Bernardo WM, et al. Endoscopic retrograde cholangiopancreatography versus endoscopic ultrasound for tissue diagnosis of malignant biliary stricture: systematic review and meta-analysis. Endosc Ultrasound 2018;7:10–19.ArticlePubMedPMC
- 25. Wang W, Shpaner A, Krishna SG, et al. Use of EUS-FNA in diagnosing pancreatic neoplasm without a definitive mass on CT. Gastrointest Endosc 2013;78:73–80.ArticlePubMed
- 26. Mohamadnejad M, DeWitt JM, Sherman S, et al. Role of EUS for preoperative evaluation of cholangiocarcinoma: a large single-center experience. Gastrointest Endosc 2011;73:71–78.ArticlePubMed
- 27. Fritscher-Ravens A, Broering DC, Knoefel WT, et al. EUS-guided fine-needle aspiration of suspected hilar cholangiocarcinoma in potentially operable patients with negative brush cytology. Am J Gastroenterol 2004;99:45–51.ArticlePubMed
- 28. Eloubeidi MA, Chen VK, Jhala NC, et al. Endoscopic ultrasound-guided fine needle aspiration biopsy of suspected cholangiocarcinoma. Clin Gastroenterol Hepatol 2004;2:209–213.ArticlePubMed
- 29. DeWitt J, Misra VL, Leblanc JK, McHenry L, Sherman S. EUS-guided FNA of proximal biliary strictures after negative ERCP brush cytology results. Gastrointest Endosc 2006;64:325–333.ArticlePubMed
- 30. Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Ann Intern Med 2009;151:W65–W94.ArticlePubMed
- 31. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 2009;6:e1000097.ArticlePubMedPMC
- 32. Whiting PF, Rutjes AW, Westwood ME, et al. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med 2011;155:529–536.ArticlePubMed
- 33. Centre for Evidence-Based Medicine. CATMaker and EBM calculators [Internet]. Oxford; CEBM: c2018 [cited 2018 Dec 7]. Available from: https://www.cebm.net/2014/06/catmaker-ebm-calculators/.
- 34. Novis M, Ardengh JC, Libera ED, et al. [Prospective comparative study of ERCP brush cytology and EUS-FNA for the differential diagnosis of biliary strictures]. Rev Col Bras Cir 2010;37:190–198.ArticlePubMedPDF
- 35. Prat F. Suspected malignant biliary strictures: from inside out or outside in? Endosc Int Open 2018;6:E778–E779.ArticlePubMedPMCPDF
- 36. Navaneethan U, Njei B, Lourdusamy V, Konjeti R, Vargo JJ, Parsi MA. Comparative effectiveness of biliary brush cytology and intraductal biopsy for detection of malignant biliary strictures: a systematic review and meta-analysis. Gastrointest Endosc 2015;81:168–176.ArticlePubMedPMC
- 37. Naitoh I, Nakazawa T, Kato A, et al. Predictive factors for positive diagnosis of malignant biliary strictures by transpapillary brush cytology and forceps biopsy. J Dig Dis 2016;17:44–51.ArticlePubMed
- 38. De Moura DTH, Coronel M, Chacon DA, et al. Primary adenosquamous cell carcinoma of the pancreas: the use of endoscopic ultrasound guided - fine needle aspiration to establish a definitive cytologic diagnosis. Rev Gastroenterol Peru 2017;37:370–373.PubMed
- 39. De Moura DTH, Coronel M, Ribeiro IB, et al. The importance of endoscopic ultrasound fine-needle aspiration in the diagnosis of solid pseudopapillary tumor of the pancreas: two case reports. J Med Case Rep 2018;12:107.ArticlePubMedPMCPDF
- 40. Banales JM, Cardinale V, Carpino G, et al. Expert consensus document: cholangiocarcinoma: current knowledge and future perspectives consensus statement from the European Network for the Study of Cholangiocarcinoma (ENS-CCA). Nat Rev Gastroenterol Hepatol 2016;13:261–280.ArticlePubMedPDF
- 41. Matynia AP, Schmidt RL, Barraza G, Layfield LJ, Siddiqui AA, Adler DG. Impact of rapid on-site evaluation on the adequacy of endoscopic-ultrasound guided fine-needle aspiration of solid pancreatic lesions: a systematic review and meta-analysis. J Gastroenterol Hepatol 2014;29:697–705.ArticlePubMedPDF
- 42. Bang JY, Kirtane S, Krall K, et al. In memoriam: fine-needle aspiration, birth: fine-needle biopsy: the changing trend in endoscopic ultrasound-guided tissue acquisition. Dig Endosc 2019;31:197–202.ArticlePubMed
- 43. Brooks C, Gausman V, Kokoy-Mondragon C, et al. Role of fluorescent in situ hybridization, cholangioscopic biopsies, and EUS-FNA in the evaluation of biliary strictures. Dig Dis Sci 2018;63:636–644.ArticlePubMedPDF
- 44. Navaneethan U, Hasan MK, Lourdusamy V, Njei B, Varadarajulu S, Hawes RH. Single-operator cholangioscopy and targeted biopsies in the diagnosis of indeterminate biliary strictures: a systematic review. Gastrointest Endosc 2015;82:608–614.e2.ArticlePubMedPMC
- 45. Heimbach JK, Sanchez W, Rosen CB, Gores GJ. Trans-peritoneal fine needle aspiration biopsy of hilar cholangiocarcinoma is associated with disease dissemination. HPB (Oxford) 2011;13:356–360.ArticlePubMedPMC
- 46. El Chafic AH, Dewitt J, Leblanc JK, et al. Impact of preoperative endoscopic ultrasound-guided fine needle aspiration on postoperative recurrence and survival in cholangiocarcinoma patients. Endoscopy 2013;45:883–889.ArticlePubMedPDF
- 47. Onda S, Ogura T, Kurisu Y, et al. EUS-guided FNA for biliary disease as first-line modality to obtain histological evidence. Therap Adv Gastroenterol 2016;9:302–312.ArticlePubMedPMC
REFERENCES
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- British Society of Gastroenterology guidelines for the diagnosis and management of cholangiocarcinoma
Simon M Rushbrook, Timothy James Kendall, Yoh Zen, Raneem Albazaz, Prakash Manoharan, Stephen P Pereira, Richard Sturgess, Brian R Davidson, Hassan Z Malik, Derek Manas, Nigel Heaton, K Raj Prasad, John Bridgewater, Juan W Valle, Rebecca Goody, Maria Hawk
Gut.2024; 73(1): 16. CrossRef - Contrast-enhanced guided endoscopic ultrasound procedures
Marcel Ioan Gheorghiu, Andrada Seicean, Cristina Pojoga, Claudia Hagiu, Radu Seicean, Zeno Sparchez
World Journal of Gastroenterology.2024; 30(17): 2311. CrossRef - ACG Clinical Guideline: Diagnosis and Management of Biliary Strictures
B. Joseph Elmunzer, Jennifer L. Maranki, Victoria Gómez, Anna Tavakkoli, Bryan G. Sauer, Berkeley N. Limketkai, Emily A. Brennan, Elaine M. Attridge, Tara J. Brigham, Andrew Y. Wang
American Journal of Gastroenterology.2023; 118(3): 405. CrossRef - Endoscopic Ultrasound in the Diagnosis of Extrahepatic Cholangiocarcinoma: What Do We Know in 2023?
Rares Ilie Orzan, Cristina Pojoga, Renata Agoston, Radu Seicean, Andrada Seicean
Diagnostics.2023; 13(6): 1023. CrossRef - Endoscopic evaluation of indeterminate biliary strictures: Cholangioscopy, endoscopic ultrasound, or both?
Raymond S. Y. Tang
Digestive Endoscopy.2023;[Epub] CrossRef - Brush Cytology, Forceps Biopsy, or Endoscopic Ultrasound-Guided Sampling for Diagnosis of Bile Duct Cancer: A Meta-Analysis
Seung Bae Yoon, Sung-Hoon Moon, Sung Woo Ko, Hyun Lim, Ho Suk Kang, Jong Hyeok Kim
Digestive Diseases and Sciences.2022; 67(7): 3284. CrossRef - Managing adverse events after endoscopic ultrasound‐guided drainage of the biliary tract and pancreatic fluid collections: Narrative review (with video)
Mateus Pereira Funari, Igor Braga Ribeiro, Marcos Eduardo Lera dos Santos, Sergio Eiji Matuguma, Eduardo Guimarães Hourneaux de Moura
Digestive Endoscopy.2022; 34(2): 359. CrossRef - Endoscopic Ultrasound for the Diagnosis and Staging of Biliary Malignancy
Martin Coronel, Jeffrey H. Lee, Emmanuel Coronel
Clinics in Liver Disease.2022; 26(1): 115. CrossRef - Endoscopic Management of Pancreatobiliary Malignancies
Dong Wook Lee, Eun Young Kim
Digestive Diseases and Sciences.2022; 67(5): 1635. CrossRef - IgG4-related sclerosing cholangitis involving the gallbladder mimicking a hilar cholangiocarcinoma
Yun Chae Lee, Hyung Ku Chon, Keum Ha Choi
Endoscopy.2022; 54(12): E739. CrossRef - Promising Genomic Testing for Biliary Tract Cancer Using Endoscopic Ultrasound-Guided Fine-Needle Aspiration/Biopsy Specimens
Masaki Kuwatani, Kazumichi Kawakubo, Naoya Sakamoto
Diagnostics.2022; 12(4): 900. CrossRef - Endoscopic Ultrasound Plus Endoscopic Retrograde Cholangiopancreatography Based Tissue Sampling for Diagnosis of Proximal and Distal Biliary Stenosis Due to Cholangiocarcinoma: Results from a Retrospective Single-Center Study
Edoardo Troncone, Fabio Gadaleta, Omero Alessandro Paoluzi, Cristina Maria Gesuale, Vincenzo Formica, Cristina Morelli, Mario Roselli, Luca Savino, Giampiero Palmieri, Giovanni Monteleone, Giovanna Del Vecchio Blanco
Cancers.2022; 14(7): 1730. CrossRef - The Role of Cholangioscopy and EUS in the Evaluation of Indeterminate Biliary Strictures
Wilson Siu, Raymond S. Y. Tang
Gastroenterology Insights.2022; 13(2): 192. CrossRef - Current endoscopic approaches to biliary strictures
Tatsuya Sato, Yousuke Nakai, Mitsuhiro Fujishiro
Current Opinion in Gastroenterology.2022; 38(5): 450. CrossRef - Acute cholecystitis caused by gallbladder metastasis from non-small cell lung cancer: a case report
Kouki Imaoka, Daisuke Satoh, Ko Oshita, Takuya Yano, Tetsushi Kubota, Michihiro Ishida, Yasuhiro Choda, Masanori Yoshimitsu, Kanyu Nakano, Masao Harano, Hiroyoshi Matsukawa, Hitoshi Idani, Shigehiro Shiozaki, Masazumi Okajima
Clinical Journal of Gastroenterology.2021; 14(1): 351. CrossRef - Current Status and Research Progress of ERCP in the Diagnosis and Treatment of Biliary and Pancreatic System Diseases
跃华 李
Advances in Clinical Medicine.2021; 11(07): 3123. CrossRef - Same day endoscopic retrograde cholangio-pancreatography immediately after endoscopic ultrasound for choledocholithiasis is feasible, safe and cost-effective
Wisam Sbeit, Anas Kadah, Amir Shahin, Tawfik Khoury
Scandinavian Journal of Gastroenterology.2021; 56(10): 1243. CrossRef - Editors' Choice of Noteworthy Clinical Endoscopy Publications in the First Decade
Gwang Ha Kim, Kwang An Kwon, Do Hyun Park, Jimin Han
Clinical Endoscopy.2021; 54(5): 633. CrossRef - Tips and tricks for the diagnosis and management of biliary stenosis-state of the art review
Giovanna Del Vecchio Blanco, Michelangela Mossa, Edoardo Troncone, Renato Argirò, Andrea Anderloni, Alessandro Repici, Omero Alessandro Paoluzi, Giovanni Monteleone
World Journal of Gastrointestinal Endoscopy.2021; 13(10): 473. CrossRef - Stent versus Balloon Dilation for the Treatment of Dominant Strictures in Primary Sclerosing Cholangitis: A Systematic Review and Meta-Analysis
Marina Tucci Gammaro Baldavira Ferreira, Igor Braga Ribeiro, Diogo Turiani Hourneaux de Moura, Thomas R. McCarty, Alberto Machado da Ponte Neto, Galileu Ferreira Ayala Farias, Antônio Afonso de Miranda Neto, Pedro Victor Aniz Gomes de Oliveira, Wanderley
Clinical Endoscopy.2021; 54(6): 833. CrossRef - Endoscopic ultrasound fine needle aspiration vs fine needle biopsy in solid lesions: A multi-center analysis
Diogo Turiani Hourneaux Moura, Thomas R McCarty, Pichamol Jirapinyo, Igor Braga Ribeiro, Galileu Ferreira Ayala Farias, Antonio Coutinho Madruga-Neto, Marvin Ryou, Christopher C Thompson
World Journal of Clinical Cases.2021; 9(34): 10507. CrossRef - Efficacy of digital single-operator cholangioscopy in the visual interpretation of indeterminate biliary strictures: a systematic review and meta-analysis
Pedro Victor Aniz Gomes de Oliveira, Diogo Turiani Hourneaux de Moura, Igor Braga Ribeiro, Ahmad Najdat Bazarbashi, Tomazo Antonio Prince Franzini, Marcos Eduardo Lera dos Santos, Wanderley Marques Bernardo, Eduardo Guimarães Hourneaux de Moura
Surgical Endoscopy.2020; 34(8): 3321. CrossRef - Role of pancreatography in the endoscopic management of encapsulated pancreatic collections – review and new proposed classification
Igor Mendonça Proença, Marcos Eduardo Lera dos Santos, Diogo Turiani Hourneaux de Moura, Igor Braga Ribeiro, Sergio Eiji Matuguma, Spencer Cheng, Thomas R McCarty, Epifanio Silvino do Monte Junior, Paulo Sakai, Eduardo Guimarães Hourneaux de Moura
World Journal of Gastroenterology.2020; 26(45): 7104. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
CiteEndoscopic Ultrasound-Guided Fine Needle Aspiration and Endoscopic Retrograde Cholangiopancreatography-Based Tissue Sampling in Suspected Malignant Biliary Strictures: A Meta-Analysis of Same-Session Procedures
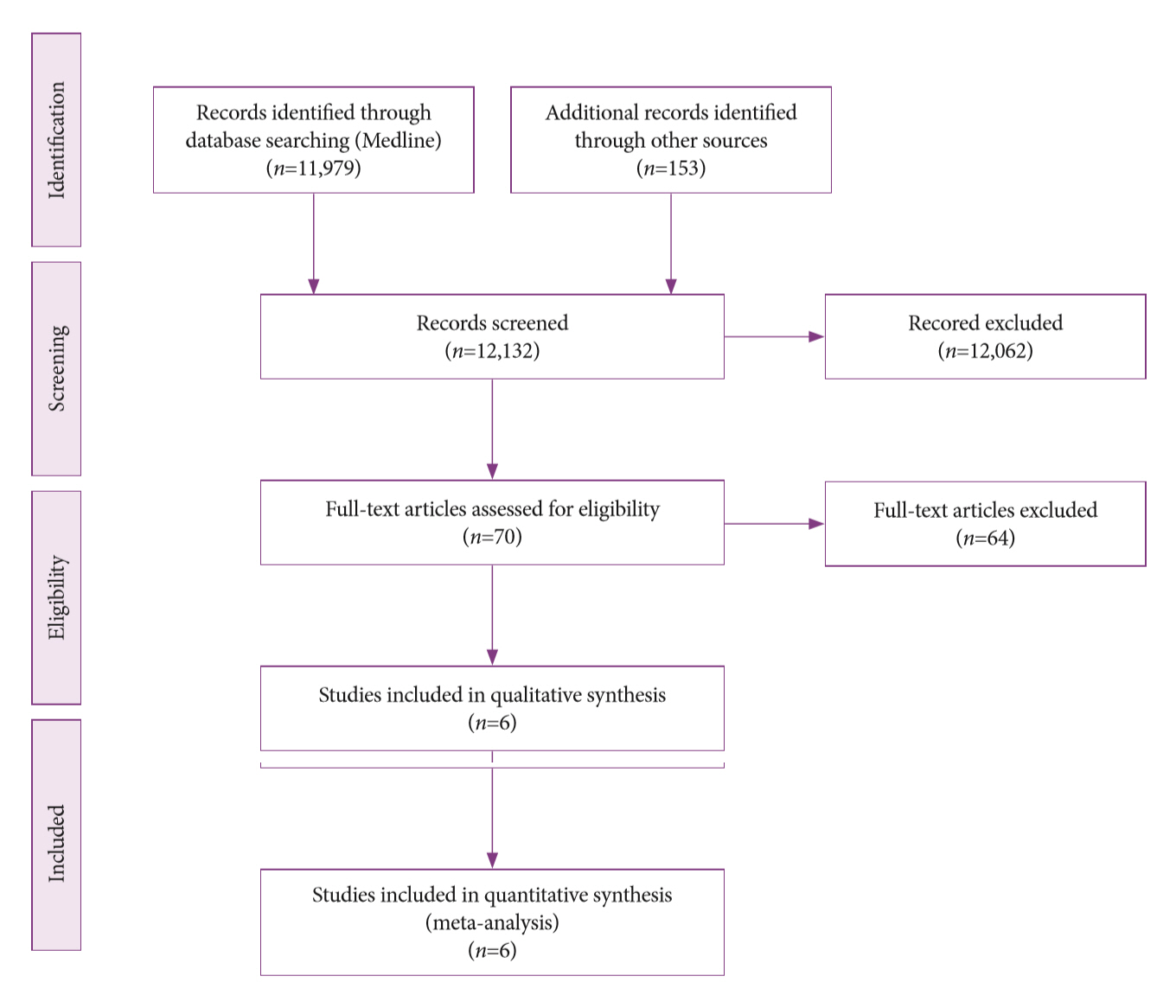
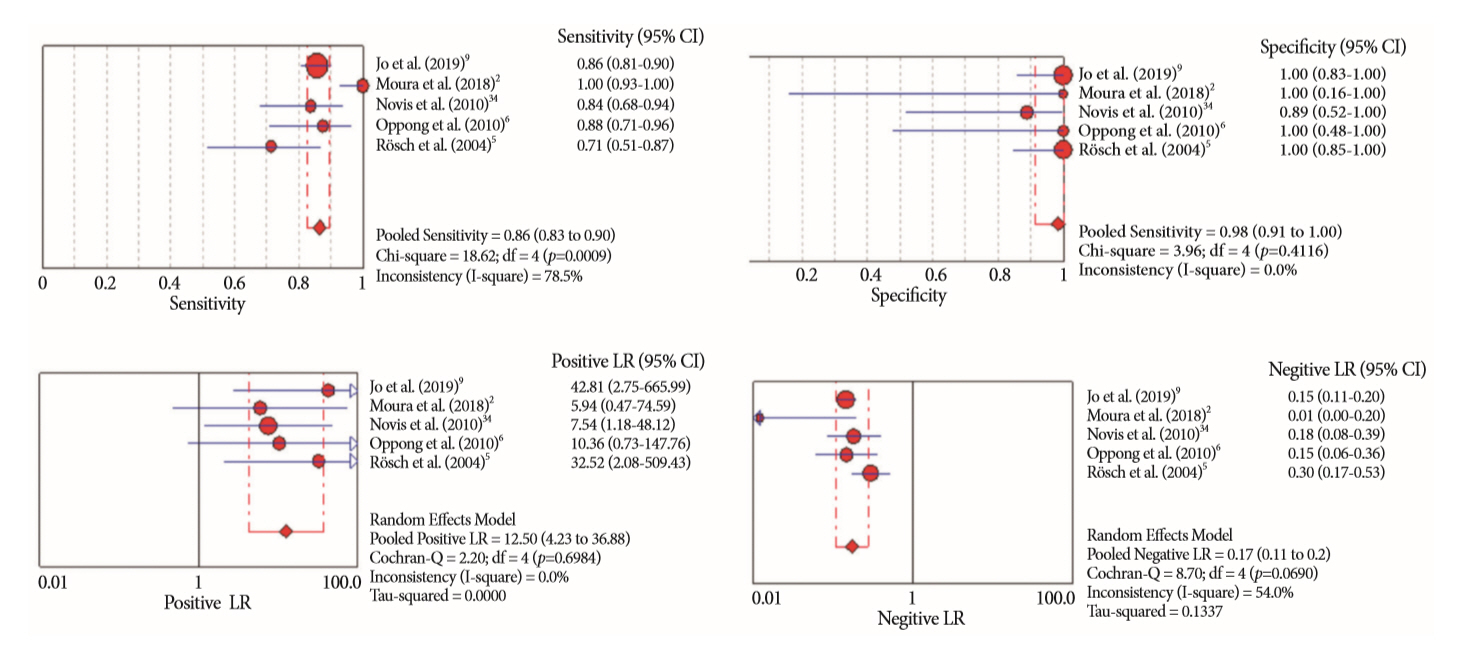
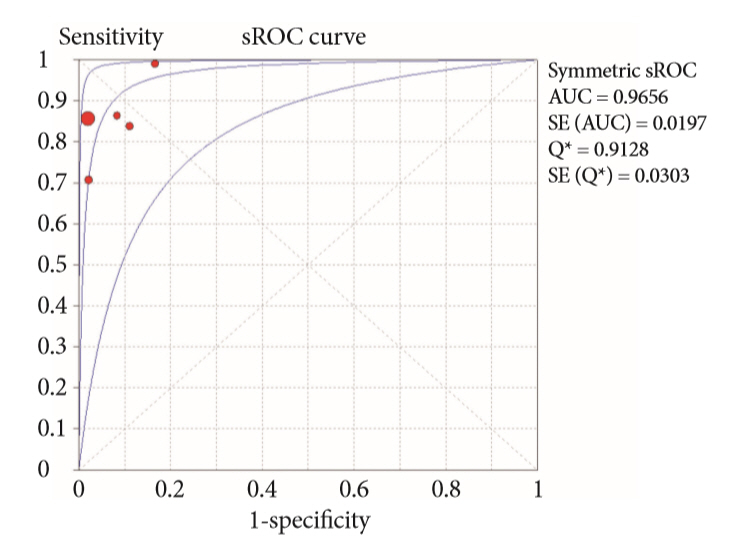
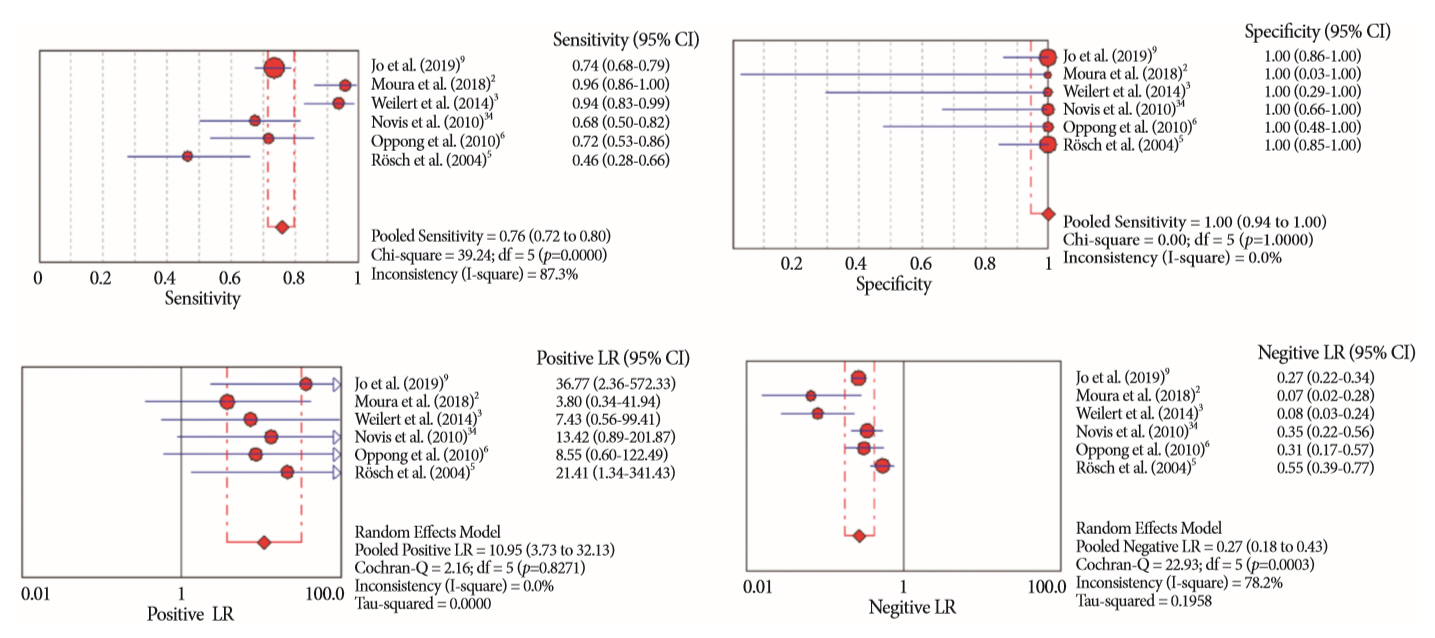
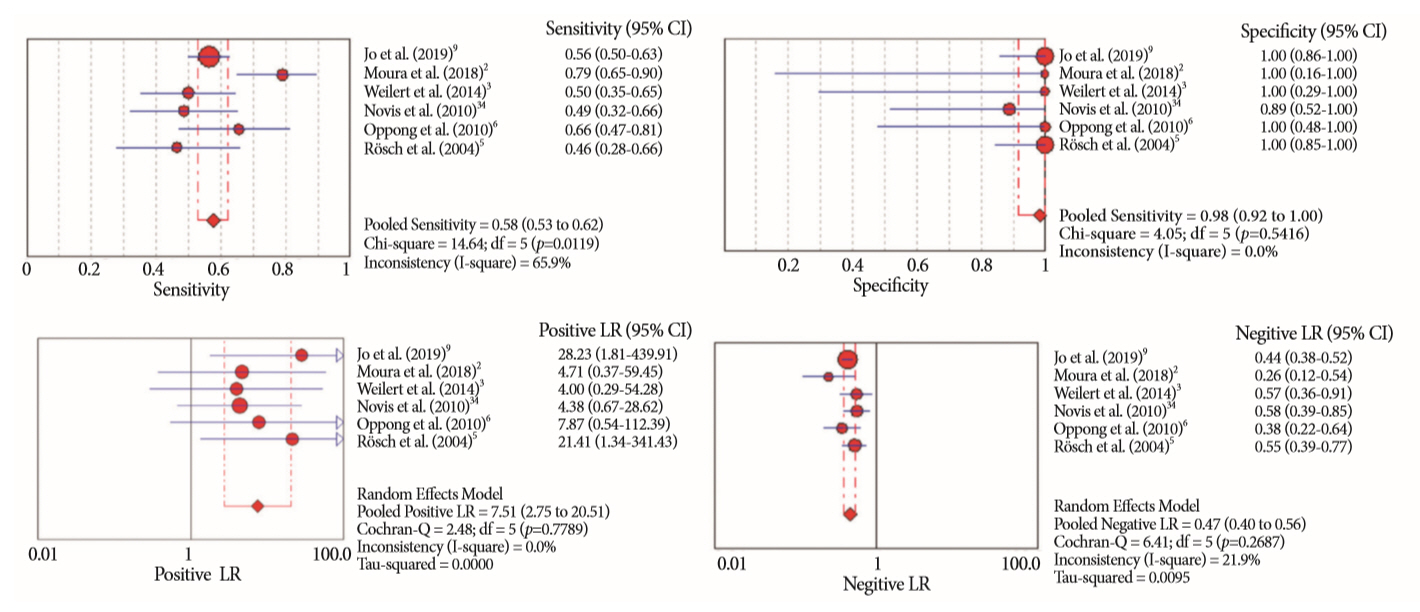
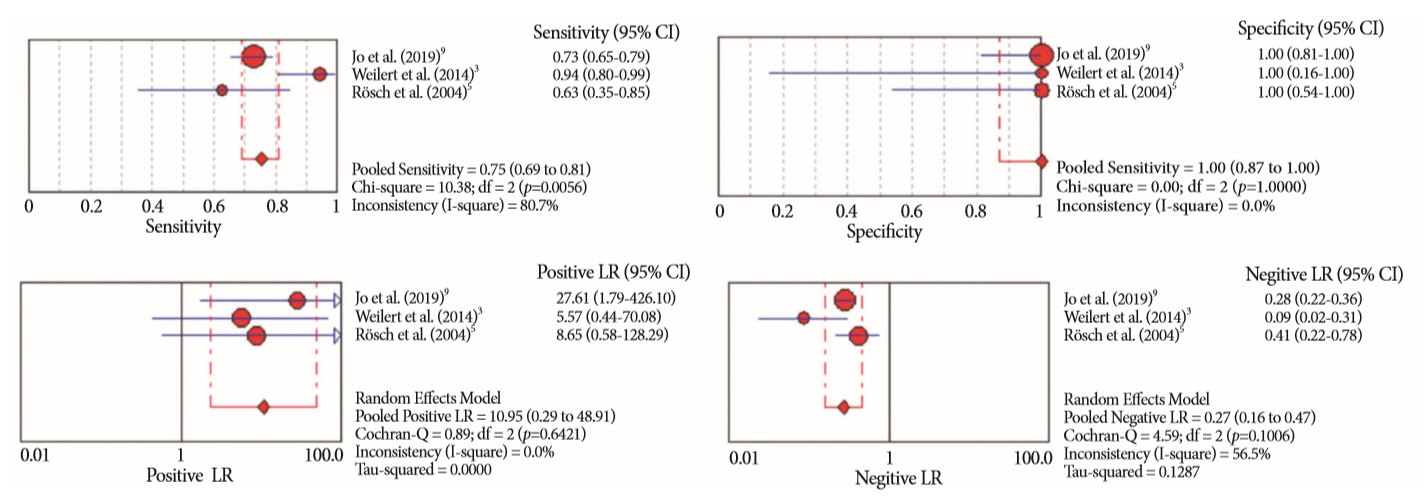
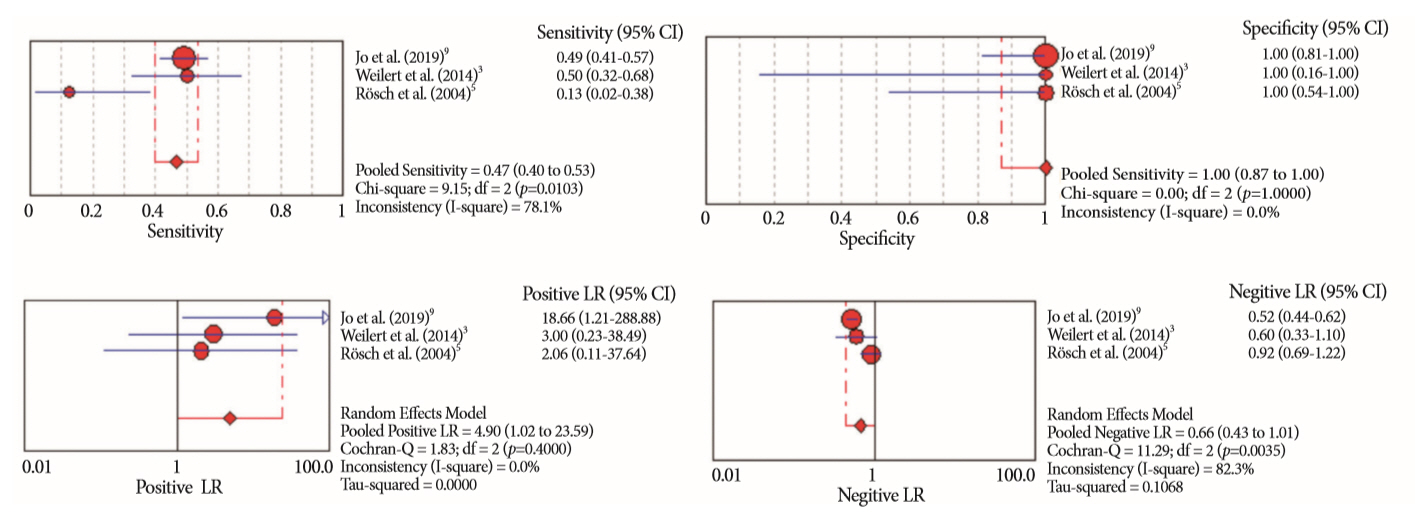
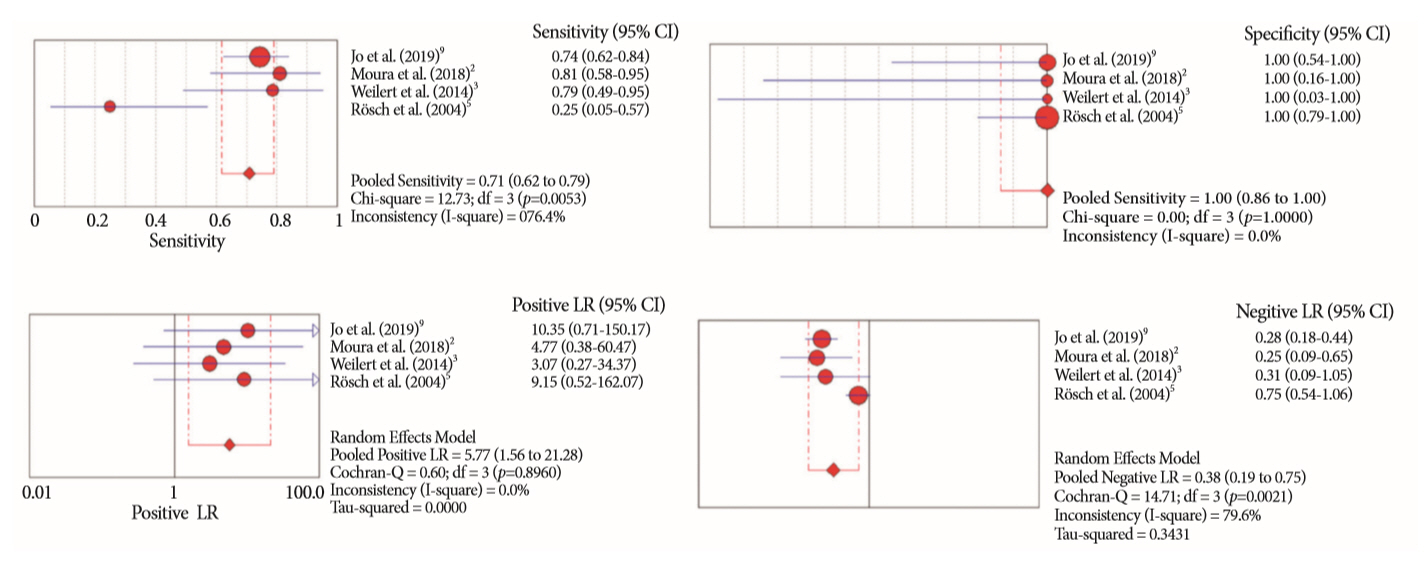
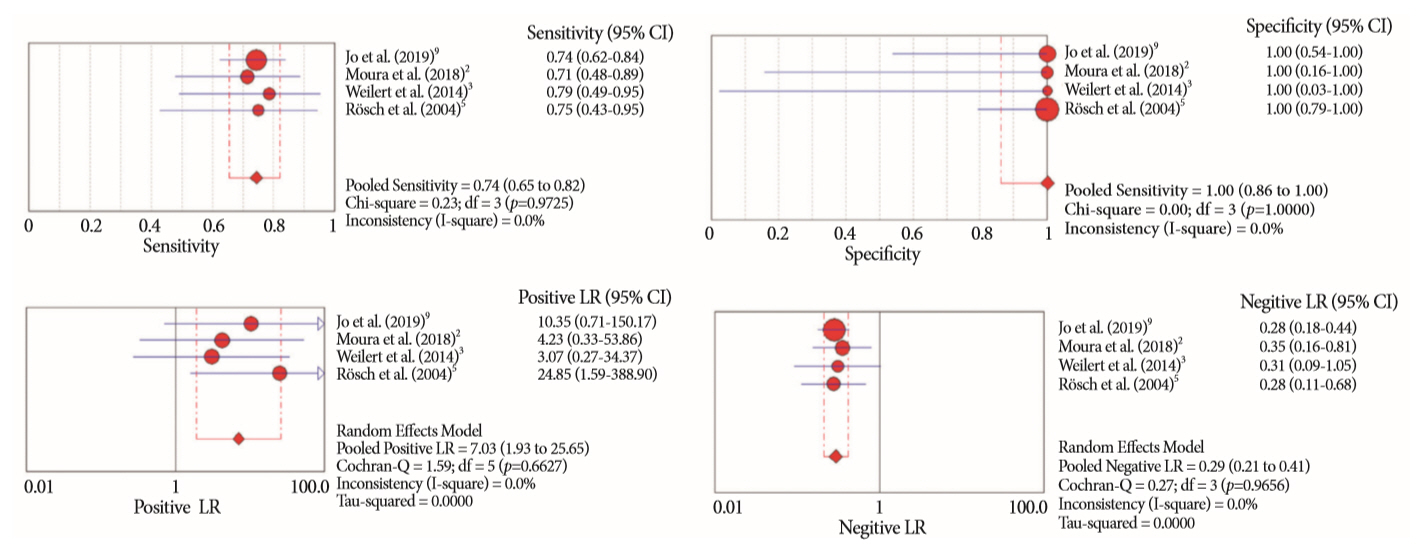
Fig. 1. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram.
Fig. 2. Forest plots of the sensitivity, specificity, positive likelihood ratio (LR) and negative LR of the association of endoscopic ultrasound-guided fine needle aspiration and endoscopic retrograde cholangiopancreatography-based tissue sampling in the diagnosis of suspected malignant biliary strictures. CI, confidence interval.
Fig. 3. Summary receiver operating characteristic (sROC) curve of the association of endoscopic ultrasound-guided fine needle aspiration and endoscopic retrograde cholangiopancreatography-based tissue sampling in the diagnosis of suspected malignant biliary strictures. AUC, area under the curve; SE, standard error.
Fig. 4. Forest plots of the sensitivity, specificity, positive likelihood ratio (LR) and negative LR of endoscopic ultrasound-guided fine needle aspiration in the diagnosis of suspected malignant biliary strictures. CI, confidence interval.
Fig. 5. Forest plots of the sensitivity, specificity, positive likelihood ratio (LR) and negative LR of endoscopic retrograde cholangiopancreatography-based tissue sampling in the diagnosis of suspected malignant biliary strictures. CI, confidence interval.
Fig. 6. Forest plots of the sensitivity, specificity, positive likelihood ratio (LR) and negative LR of endoscopic ultrasound-guided fine needle aspiration in the diagnosis of pancreatic lesion causing biliary strictures. CI, confidence interval.
Fig. 7. Forest plots of the sensitivity, specificity, positive likelihood ratio (LR) and negative LR of endoscopic retrograde cholangiopancreatography in the diagnosis of pancreatic lesion causing biliary strictures. CI, confidence interval.
Fig. 8. Forest plots of the sensitivity, specificity, positive likelihood ratio (LR) and negative LR of endoscopic ultrasound-guided fine needle aspiration in the diagnosis of biliary lesions. CI, confidence interval.
Fig. 9. Forest plots of the sensitivity, specificity, positive likelihood ratio (LR) and negative LR of endoscopic retrograde cholangiopancreatography-based tissue sampling in the diagnosis of biliary lesions. CI, confidence interval.


