
Search
- Page Path
- HOME > Search
Case Report
- Bronchoesophageal fistula in a patient with Crohn’s disease receiving anti-tumor necrosis factor therapy
- Kyunghwan Oh, Kee Don Choi, Hyeong Ryul Kim, Tae Sun Shim, Byong Duk Ye, Suk-Kyun Yang, Sang Hyoung Park
- Clin Endosc 2023;56(2):239-244. Published online December 21, 2021
- DOI: https://doi.org/10.5946/ce.2021.215
-
 Abstract
Abstract
 PDF
PDF PubReader
PubReader ePub
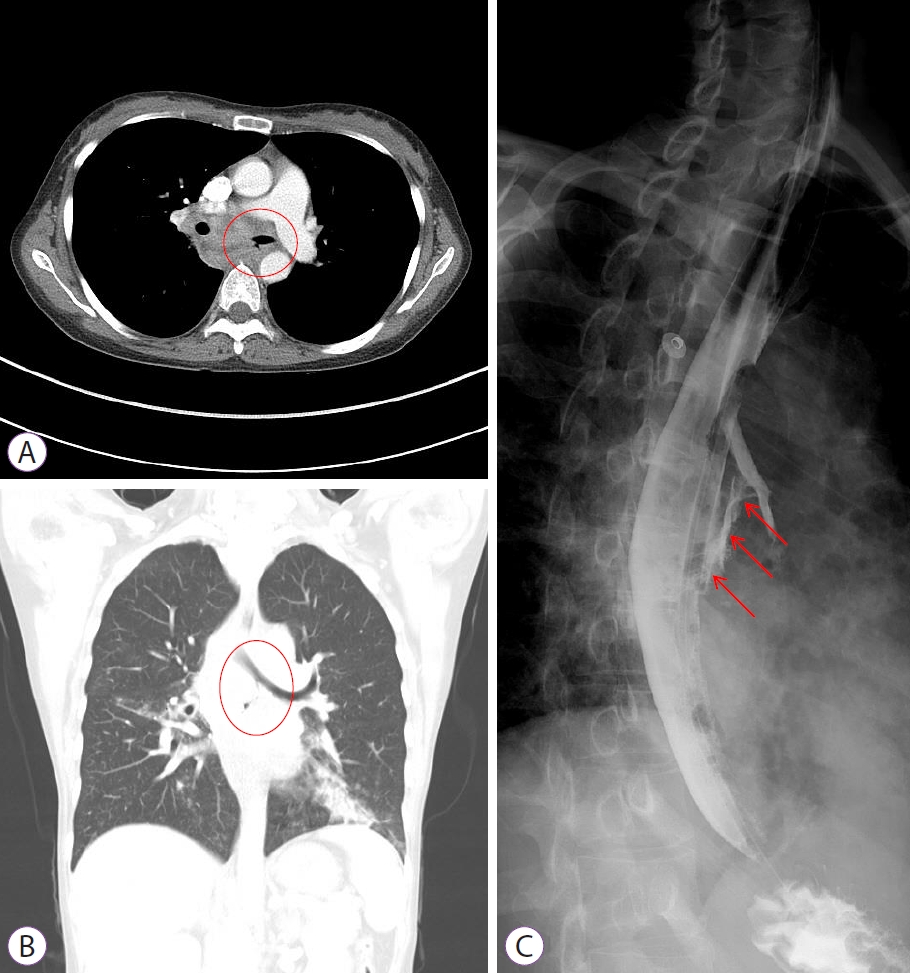
ePub - Tuberculosis is an adverse event in patients with Crohn’s disease receiving anti-tumor necrosis factor (TNF) therapy. However, tuberculosis presenting as a bronchoesophageal fistula (BEF) is rare. We report a case of tuberculosis and BEF in a patient with Crohn’s disease who received anti-TNF therapy. A 33-year-old Korean woman developed fever and cough 2 months after initiation of anti-TNF therapy. And the symptoms persisted for 1 months, so she visited the emergency room. Chest computed tomography was performed upon visiting the emergency room, which showed BEF with aspiration pneumonia. Esophagogastroduodenoscopy with biopsy and endobronchial ultrasound with transbronchial needle aspiration confirmed that the cause of BEF was tuberculosis. Anti-tuberculosis medications were administered, and esophageal stent insertion through endoscopy was performed to manage the BEF. However, the patient’s condition did not improve; therefore, fistulectomy with primary closure was performed. After fistulectomy, the anastomosis site healing was delayed due to severe inflammation, a second esophageal stent and gastrostomy tube were inserted. Nine months after the diagnosis, the fistula disappeared without recurrence, and the esophageal stent and gastrostomy tube were removed.
-
Citations
Citations to this article as recorded by
- (Re-)introduction of TNF antagonists and JAK inhibitors in patients with previous tuberculosis: a systematic review
Thomas Theo Brehm, Maja Reimann, Niklas Köhler, Christoph Lange
Clinical Microbiology and Infection.2024;[Epub] CrossRef - Azathioprine/infliximab/methylprednisolone
Reactions Weekly.2023; 1963(1): 114. CrossRef
- (Re-)introduction of TNF antagonists and JAK inhibitors in patients with previous tuberculosis: a systematic review
- 3,743 View
- 272 Download
- 2 Crossref

Original Article
- Endoscopic Mucosal Resection with Circumferential Mucosal Incision for Colorectal Neoplasms: Comparison with Endoscopic Submucosal Dissection and between Two Endoscopists with Different Experiences
- Dong-Hoon Yang, Min-Seob Kwak, Sang Hyoung Park, Byong Duk Ye, Jeong-Sik Byeon, Seung-Jae Myung, Suk-Kyun Yang, Hyun Gun Kim, Shai Friedland
- Clin Endosc 2017;50(4):379-387. Published online March 7, 2017
- DOI: https://doi.org/10.5946/ce.2016.058
-
Abstract
PDFPubReaderePub
- Background
/Aims: Endoscopic mucosal resection with circumferential mucosal incision (CMI-EMR) may offer benefits comparable to those of endoscopic submucosal dissection (ESD), while requiring less technical proficiency than ESD.
Methods
We retrospectively compared the outcomes of CMI-EMR (n=34) and size-matched ESD (n=102), which were performed by a Korean endoscopist for colorectal epithelial lesions of 20–35 mm. Procedural parameters of CMI-EMRs performed by an American ESD novice ((n=30) were compared with those performed by the Korean endoscopist.
Results
The lesion size was 22.3±3.9 mm and 22.9±2.4 mm in the CMI-EMR and size-matched ESD groups, respectively (p=0.730). The resection time was 12.7±7.0 minutes in the CMI-EMR group and 45.6±30.1 minutes in the ESD group (p<0.001). The en bloc resection rate was 94.1% in the CMI-EMR group and 100% in the ESD group (p=0.061). There were no differences in the en bloc resection and complication rates of CMI-EMRs between a Korean and an American endoscopist.
Conclusions
For the treatment of moderate-size colorectal lesions, CMI-EMR showed a trend toward lower en bloc resection rate, but required shorter procedure time than ESD. CMI-EMR outcomes were similar when performed by a Korean ESD expert and an American ESD novice. -
Citations
Citations to this article as recorded by- Endoscopic mucosal resection with a circumferential incision in the removal of colon neoplasms. Results of a randomized trial.
E. U. Abdulzhalieva, A. A. Likutov, V. V. Veselov, D. A. Mtvralashvili, O. M. Yugai, E. A. Khomyakov, S. V. Chernyshov, O. I. Sushkov
Koloproktologia.2024; 23(1): 21. CrossRef - Hybrid Endoscopic Resection With Endo-knife and Snare for Colorectal Lesions: A Systematic Review and Meta-analysis
Shinji Yoshii, Takefumi Kikuchi, Yuki Hayashi, Masahiro Nojima, Hiro-o Yamano, Hiroshi Nakase
Techniques and Innovations in Gastrointestinal Endoscopy.2023; 25(2): 135. CrossRef - Multicenter evaluation of recurrence in endoscopic submucosal dissection and endoscopic mucosal resection in the colon: A Western perspective
Mike T Wei, Margaret J Zhou, Andrew A Li, Andrew Ofosu, Joo Ha Hwang, Shai Friedland
World Journal of Gastrointestinal Endoscopy.2023; 15(6): 458. CrossRef - Comparison of precutting endoscopic mucosal resection and endoscopic submucosal dissection for large (20–30 mm) flat colorectal lesions
Chang Kyo Oh, Young Wook Cho, In Hyoung Choi, Han Hee Lee, Chul‐Hyun Lim, Jin Su Kim, Bo‐In Lee, Young‐Seok Cho
Journal of Gastroenterology and Hepatology.2022; 37(3): 568. CrossRef - A systematic review and meta-analysis of endoscopic mucosal resection vs endoscopic submucosal dissection for colorectal sessile/non-polypoid lesions
Endrit Shahini, Roberto Passera, Giacomo Lo Secco, Alberto Arezzo
Minimally Invasive Therapy & Allied Technologies.2022; 31(6): 835. CrossRef - Endoscopic mucosal resection with a circumferential incision in the removal of colorectal neoplasms (preliminary results of the prospective randomized study)
A. U. Abdulzhalieva, A. A. Likutov, D. A. Mtvralashvili, V. V. Veselov, Yu. E. Vaganov, S. V. Chernyshov, O. A. Mainovskaya, O. I. Sushkov
Koloproktologia.2022; 21(4): 21. CrossRef - Efficacy and Safety of Complete Endoscopic Resection of Colorectal Neoplasia Using a Stepwise Endoscopic Protocol with SOUTEN, a Novel Multifunctional Snare
Shinji Yoshii, Marina Kubo, Mio Matsumoto, Takefumi Kikuchi, Yasunari Takakuwa
Clinical Endoscopy.2020; 53(2): 206. CrossRef - Tip-in versus conventional endoscopic mucosal resection for flat colorectal neoplasia 10 mm or larger in size
Soo Min Noh, Jin Yong Kim, Jae Cheol Park, Eun Hye Oh, Jeongseok Kim, Nam Seok Ham, Sung Wook Hwang, Sang Hyoung Park, Byong Duk Ye, Jeong-Sik Byeon, Seung-Jae Myung, Suk-Kyun Yang, Dong-Hoon Yang
International Journal of Colorectal Disease.2020; 35(7): 1283. CrossRef - Long‐term clinical outcomes of endoscopic submucosal dissection for colorectal neoplasia with or without the hybrid technique
DU Kang, JC Park, SW Hwang, SH Park, DH Yang, KJ Kim, BD Ye, SJ Myung, SK Yang, JS Byeon
Colorectal Disease.2020; 22(12): 2008. CrossRef - Pyogenic Liver Abscess Caused by Endoscopic Submucosal Dissection for Early Colon Cancer
Joon Seop Lee, Yong Hwan Kwon
Clinical Endoscopy.2019; 52(6): 620. CrossRef - Endoscopic submucosal dissection in the West: Current status and future directions
Michael X. Ma, Michael J. Bourke
Digestive Endoscopy.2018; 30(3): 310. CrossRef - Introduction of endoscopic submucosal dissection in the West
David Friedel, Stavros Nicholas Stavropoulos
World Journal of Gastrointestinal Endoscopy.2018; 10(10): 225. CrossRef - Filling the Technical Gap between Standard Endoscopic Mucosal Resection and Full Endoscopic Submucosal Dissection for 20–35 mm Sized Colorectal Neoplasms
Sung Noh Hong
Clinical Endoscopy.2017; 50(4): 313. CrossRef
- Endoscopic mucosal resection with a circumferential incision in the removal of colon neoplasms. Results of a randomized trial.
- 8,807 View
- 232 Download
- 13 Web of Science
- 13 Crossref
Case Report
- Single Balloon Enteroscopy-Assisted Endoscopic Retrograde Cholangiopancreatography in Patients Who Underwent a Gastrectomy with Roux-en-Y Anastomosis: Six Cases from a Single Center
- Jae Seung Soh, Dong-Hoon Yang, Sang Soo Lee, Seohyun Lee, Jungho Bae, Jeong-Sik Byeon, Seung-Jae Myung, Suk-Kyun Yang
- Clin Endosc 2015;48(5):452-457. Published online September 30, 2015
- DOI: https://doi.org/10.5946/ce.2015.48.5.452
-
Abstract
PDFPubReaderePub
Patients with altered anatomy such as a Roux-en-Y anastomosis often present with various pancreaticobiliary problems requiring therapeutic intervention. However, a conventional endoscopic approach to the papilla is very difficult owing to the long afferent limb and acute angle of a Roux-en-Y anastomosis. Balloon-assisted enteroscopy can be used for endoscopic retrograde cholangiopancreatography (ERCP) in patients with altered anatomy. We experienced six cases of Roux-en-Y anastomosis with biliary problems, and attempted ERCP using single balloon enteroscopy (SBE). SBE insertion followed by replacement with a conventional endoscope was attempted in five of six patients. The papilla was successfully approached using SBE in all cases. However, therapeutic intervention was completed in only three cases because of poor maneuverability caused by postoperative adhesion. We conclude that in patients with Roux-en-Y anastomosis, the ampulla can be readily accessed with SBE, but longer dedicated accessories are necessary to improve this therapeutic intervention.
-
Citations
Citations to this article as recorded by- Single Balloon Enteroscopy-Guided Endoscopic Retrograde Cholangiopancreatography in Surgically Altered Anatomy: Long vs. Short Type
Chang-Hwan Park
The Korean Journal of Pancreas and Biliary Tract.2021; 26(3): 181. CrossRef - Direct Insertion of a Short-Type Single-Balloon Enteroscope and Using a Stent Retriever to Treat Difficult Bile Duct Stones in Surgically Altered Anatomy
Takashi Sasaki, Naoki Sasahira
Clinical Endoscopy.2021; 54(6): 937. CrossRef - Single-balloon enteroscopy-assisted ERCP in patients with Roux-en-Y anatomy and choledocholithiasis: do technical improvements mean better outcomes?
Jesús Espinel Díez, María Eugenia Pinedo Ramos
Revista Española de Enfermedades Digestivas.2020;[Epub] CrossRef - Application of single balloon enteroscopy-assisted therapeutic endoscopic retrograde cholangiopancreatography in patients after bilioenteric Roux-en-Y anastomosis: Experience of multi-disciplinary collaboration
Wen-Guang Wu, Lu-Cui Qin, Xiao-Ling Song, Ming-Ning Zhao, Wen-Jie Zhang, Jun Gu, Hao Weng, Ying-Bin Liu, Yi Zhang, Chun-Ying Qu, Lei-Ming Xu, Xue-Feng Wang
World Journal of Gastroenterology.2019; 25(36): 5505. CrossRef - Comparison between Enteroscopy-Based and Laparoscopy-Assisted ERCP for Accessing the Biliary Tree in Patients with Roux-en-Y Gastric Bypass: Systematic Review and Meta-analysis
Alberto Machado da Ponte-Neto, Wanderley M. Bernardo, Lara M. de A. Coutinho, Iatagan Rocha Josino, Vitor Ottoboni Brunaldi, Diogo T. H. Moura, Paulo Sakai, Rogério Kuga, Eduardo G. H. de Moura
Obesity Surgery.2018; 28(12): 4064. CrossRef - Impact of a Newly Developed Short Double-Balloon Enteroscope on Stent Placement in Patients with Surgically Altered Anatomies
Koichiro Tsutsumi, Hironari Kato, Hiroyuki Okada
Gut and Liver.2017; 11(2): 306. CrossRef
- Single Balloon Enteroscopy-Guided Endoscopic Retrograde Cholangiopancreatography in Surgically Altered Anatomy: Long vs. Short Type
- 8,101 View
- 79 Download
- 5 Web of Science
- 6 Crossref
Original Article
- Postpolypectomy Fever, a Rare Adverse Event of Polypectomy: Nested Case-Control Study
- Seung-Hoon Lee, Kyung-Jo Kim, Dong-Hoon Yang, Kee Wook Jeong, Byong Duk Ye, Jeong-Sik Byeon, Seung-Jae Myung, Suk-Kyun Yang, Jin-Ho Kim
- Clin Endosc 2014;47(3):236-241. Published online May 31, 2014
- DOI: https://doi.org/10.5946/ce.2014.47.3.236
-
Abstract
PDFPubReaderePub
Background/Aims Although postpolypectomy fever (PPF) without colon perforation or hemorrhage is rare, its incidence and risk factors have not been investigated. The objective of this study was to analyze the incidence and risk factors for PPF among inpatients.
Methods Seven patients with PPF were matched with 70 patients without PPF from a total of 3,444 patients who underwent colonoscopic polypectomy. The PPF incidence during index hospitalization after colonoscopy was calculated, and univariate and multivariate analyses were performed to calculate the adjusted odds ratios (ORs) for risk factors.
Results PPF without bleeding or perforation in the colon occurred in seven patients (0.2%). The median age was 58 years for cases and 61 years for controls. The median interval from polypectomy to occurrence of fever was 7 hours, and the median duration of fever was 9 hours. Polyp size >2 cm (adjusted OR, 1.08; 95% confidence interval [CI], 1.01 to 1.15;
p =0.02) and hypertension (adjusted OR, 14.40; 95% CI, 1.23 to 180.87;p =0.03) were associated with a significantly increased risk of PPF. PPF increased the length of hospitalization.Conclusions Although the crude incidence of PPF is low, PPF may prolong hospitalization. Risk factors for PPF include hypertension and large polyps.
-
Citations
Citations to this article as recorded by- Cold Snare Cut Versus Avulsion for Colonic Mucosal Resection: A Randomized Ex Vivo Porcine Study (the CONVINCE Study)
Neal A. Mehta, James K. Stone, Roberto Trasolini, Yuho Ono, Mandeep S. Sawhney
Techniques and Innovations in Gastrointestinal Endoscopy.2023; 25(4): 315. CrossRef - Cold Endoscopic Mucosal Resection (c-EMR) of Nonpedunculated Colorectal Polyps ≥20 mm
Daryl Ramai, Benjamin Clement, Marcello Maida, Melissa Previtera, Olivia W. Brooks, Yichen Wang, Saurabh Chandan, Banreet Dhindsa, Smit Deliwala, Antonio Facciorusso, Mouen Khashab, Andrew Ofosu
Journal of Clinical Gastroenterology.2023;[Epub] CrossRef - Risk factors of medication‐related osteonecrosis of the jaw in preventive tooth extraction before bone resorption inhibitor administration: A multicenter nested case–control study
Taro Saito, Atsushi Nishikawa, Yuko Hara‐Saito, Andrea Rei Estacio Salazar, Akira Kurokawa, Akihiko Iida, Masahiro Yamaga, Hiroyuki Kano, Yusuke Kato, Yoshiyuki Takata, Hideyoshi Nishiyama, Nobutaka Kitamura, Takahiro Tanaka, Ritsuo Takagi
Oral Science International.2022; 19(2): 79. CrossRef - Postpolypectomy fever in patients with serious infection: a report of two cases
Wang Jing, Li Qinghua, Yang Zhiwen
BMC Gastroenterology.2022;[Epub] CrossRef - RoboCap: Robotic mucus-clearing capsule for enhanced drug delivery in the gastrointestinal tract
Shriya S. Srinivasan, Amro Alshareef, Alexandria V. Hwang, Ziliang Kang, Johannes Kuosmanen, Keiko Ishida, Joshua Jenkins, Sabrina Liu, Wiam Abdalla Mohammed Madani, Jochen Lennerz, Alison Hayward, Josh Morimoto, Nina Fitzgerald, Robert Langer, Giovanni T
Science Robotics.2022;[Epub] CrossRef - Pylephlebitis after sigmoid colonic polypectomy
Yuna Saito, Toshinori Nishizawa, Hiroko Arioka
BMJ Case Reports.2022; 15(12): e253095. CrossRef - Management of Pediatric Postendoscopy Fever
Julia M. Boster, Melissa Iwanowski, Robert E. Kramer
Journal of Pediatric Gastroenterology and Nutrition.2021; 72(2): 250. CrossRef - Cold versus hot polypectomy/endoscopic mucosal resection–A review of current evidence
Raquel Ortigão, Jochen Weigt, Ahmed Afifi, Diogo Libânio
United European Gastroenterology Journal.2021; 9(8): 938. CrossRef - Periprocedural adverse events after endoscopic resection of T1 colorectal carcinomas
Steffi E.M. van de Ven, Yara Backes, Mirrian Hilbink, Tom C.J. Seerden, Koen Kessels, Wouter H. de Vos tot Nederveen Cappel, John N. Groen, Frank H.J. Wolfhagen, Joost M.J. Geesing, Frank ter Borg, Jeroen van Bergeijk, B.W.M. Spanier, Marco W. Mundt, H.J.
Gastrointestinal Endoscopy.2020; 91(1): 142. CrossRef - Colección abscesificada en pared abdominal secundaria a polipectomía colonoscópica. Manejo radiológico
María Luisa García-García, Miguel Ángel Jiménez-Ballester, Enrique Girela-Baena, José Luis Aguayo-Albasini
Gastroenterología y Hepatología.2017; 40(7): 463. CrossRef - Endoscopic shielding technique with a newly developed hydrogel to prevent thermal injury in two experimental models
Vicente Lorenzo‐Zúñiga, Jaume Boix, Vicente Moreno de Vega, Ignacio Bon, Ingrid Marín, Ramón Bartolí
Digestive Endoscopy.2017; 29(6): 702. CrossRef - Colorectal endoscopic mucosal resection (EMR)
Pujan Kandel, Michael B. Wallace
Best Practice & Research Clinical Gastroenterology.2017; 31(4): 455. CrossRef - Abdominal wall abscess secondary to colonoscopic polypectomy. Radiological management
María Luisa García-García, Miguel Ángel Jiménez-Ballester, Enrique Girela-Baena, José Luis Aguayo-Albasini
Gastroenterología y Hepatología (English Edition).2017; 40(7): 463. CrossRef - Complications of endoscopic polypectomy, endoscopic mucosal resection and endoscopic submucosal dissection in the colon
Michael X. Ma, Michael J. Bourke
Best Practice & Research Clinical Gastroenterology.2016; 30(5): 749. CrossRef - What Is Different between Postpolypectomy Fever and Postpolypectomy Coagulation Syndrome?
Hyung Wook Kim
Clinical Endoscopy.2014; 47(3): 205. CrossRef
- Cold Snare Cut Versus Avulsion for Colonic Mucosal Resection: A Randomized Ex Vivo Porcine Study (the CONVINCE Study)
- 7,270 View
- 90 Download
- 15 Web of Science
- 15 Crossref
Reviews
- Korean Guidelines for Postpolypectomy Colonoscopy Surveillance
- Dong-Hoon Yang, Sung Noh Hong, Young-Ho Kim, Sung Pil Hong, Sung Jae Shin, Seong-Eun Kim, Bo In Lee, Suck-Ho Lee, Dong Il Park, Hyun-Soo Kim, Suk-Kyun Yang, Hyo Jong Kim, Se Hyung Kim, Hyun Jung Kim, Multi-Society Task Force for Development of Guidelines for Colorectal Polyp Screening, Surveillance and Management
- Clin Endosc 2012;45(1):44-61. Published online March 31, 2012
- DOI: https://doi.org/10.5946/ce.2012.45.1.44
-
Abstract
PDF
 Supplementary MaterialPubReaderePub
Supplementary MaterialPubReaderePub Postpolypectomy surveillance has become a major indication for colonoscopy as a result of increased use of screening colonoscopy in Korea. In this report, a careful analytic approach was used to address all available evidences to delineate the predictors for advanced neoplasia at surveillance colonoscopy and we elucidated the high risk findings of the index colonoscopy as follows: 3 or more adenomas, any adenoma larger than 10 mm, any tubulovillous or villous adenoma, any adenoma with high-grade dysplasia, and any serrated polyps larger than 10 mm. Surveillance colonoscopy should be performed five years after the index colonoscopy for those without any high-risk findings and three years after the index colonoscopy for those with one or more high risk findings. However, the surveillance interval can be shortened considering the quality of the index colonoscopy, the completeness of polypectomy, the patient's general condition, and family and medical history.
-
Citations
Citations to this article as recorded by- Post-colonoscopy colorectal cancers in a national fecal immunochemical test-based colorectal cancer screening program
Pieter H. A. Wisse, Sybrand Y. de Boer, Marco Oudkerk Pool, Jochim S Terhaar sive Droste, Claudia Verveer, Gerrit A. Meijer, Evelien Dekker, Manon C. W. Spaander
Endoscopy.2024; 56(05): 364. CrossRef - Recurrence rates of advanced colorectal neoplasia (ACN) in subjects with baseline ACN followed up at different surveillance intervals
Martin C.S. Wong, Eman Yee-man Leung, Sam C.C. Chun, Yunyang Deng, Thomas Lam, Raymond S.Y. Tang, Junjie Huang
Digestive and Liver Disease.2023; 55(12): 1742. CrossRef - Risk of recurrent advanced colorectal neoplasia in individuals with baseline non‐advanced neoplasia followed up at 5 vs 7–10 years
Martin C. S. Wong, Eman Yee‐man Leung, Sam C. C. Chun, Yunyang Deng, Thomas Lam, Raymond S. Y. Tang, Junjie Huang
Journal of Gastroenterology and Hepatology.2023; 38(12): 2122. CrossRef - Third Asia-Pacific consensus recommendations on colorectal cancer screening and postpolypectomy surveillance
Joseph J Y Sung, Han-Mo Chiu, David Lieberman, Ernst J Kuipers, Matthew D Rutter, Finlay Macrae, Khay-Guan Yeoh, Tiing Leong Ang, Vui Heng Chong, Sneha John, Jingnan Li, Kaichun Wu, Simon S M Ng, Govind K Makharia, Murdani Abdullah, Nozomu Kobayashi, Masa
Gut.2022; 71(11): 2152. CrossRef - Optimization of the surveillance strategy in patients with colorectal adenomas: A combination of clinical parameters and index colonoscopy findings
Chan Hyuk Park, Yoon Suk Jung, Nam Hee Kim, Jung Ho Park, Dong Il Park, Chong Il Sohn
Journal of Gastroenterology and Hepatology.2021; 36(4): 974. CrossRef - Increasing changes in visceral adiposity is associated with higher risk for colorectal adenoma: Multilevel analysis in a prospective cohort
Jung Min Moon, Jong Pil Im, Donghee Kim, Yoo Min Han, Hosim Soh, Ji Hyun Song, Sun Young Yang, Young Sun Kim, Jeong Yoon Yim, Seon Hee Lim, Joo Sung Kim
Journal of Gastroenterology and Hepatology.2021; 36(7): 1836. CrossRef - Strategies for colorectal cancer screening and post-polypectomy surveillance for young adults under age 50
Yoon Suk Jung
Precision and Future Medicine.2021; 5(2): 69. CrossRef - Adherence to Surveillance Guidelines after the Removal of Colorectal Polyps: A Multinational, Multicenter, Prospective Survey
Chang Kyo Oh, Satimai Aniwan, Panida Piyachaturawat, Zhiqin Wong, Thida Soe, Bayasgalan Luvsandagva, Quang Trung Tran, Achmad Fauzi, Jeong-Sik Byeon, Young-Seok Cho
Gut and Liver.2021; 15(6): 878. CrossRef - Colon Polyp Detection in Primary Health Care Institutions of Korea: Detection Rate and Issues with Following the Guidelines
Sang Hyun Park, Kwang Il Hong, Hyun Chul Park, Young Sun Kim, Gene Hyun Bok, Kyung Ho Kim, Dong Suk Shin, Jae Yong Han, Young Kwan Kim, Yeun Jong Choi, Soo Hoon Eun, Byung Hoon Lim, Kyeong Kun Kwack
The Korean Journal of Gastroenterology.2021; 78(6): 328. CrossRef - Effect of Cotinine-Verified Change in Smoking Status on Risk of Metachronous Colorectal Neoplasia After Polypectomy
Yoon Suk Jung, Nam Hee Kim, Mi Yeon Lee, Jung Ho Park, Dong Il Park, Chong Il Sohn
Clinical Gastroenterology and Hepatology.2020; 18(1): 163. CrossRef - Risk of developing metachronous advanced colorectal neoplasia after resection of low-risk diminutive versus small adenomas
Nam Hee Kim, Yoon Suk Jung, Jung Ho Park, Dong Il Park, Chong Il Sohn
Gastrointestinal Endoscopy.2020; 91(3): 622. CrossRef - Colorectal sessile serrated lesion with large size or synchronous neoplasm: a prospective study
Laxmi B. Chavali, Kun Hu, Anish Sheth, Nan Gao, Wei Xiong, Lanjing Zhang
European Journal of Gastroenterology & Hepatology.2020; 32(2): 199. CrossRef - Colorectal Polyp Prevalence According to Alcohol Consumption, Smoking and Obesity
Kyujin Lee, Yong Hwan Kim
International Journal of Environmental Research and Public Health.2020; 17(7): 2387. CrossRef - Comparative systematic review and meta-analysis of 1- to 5-mm versus 6- to 9-mm adenomas on the risk of metachronous advanced colorectal neoplasia
Yoon Suk Jung, Tae Jun Kim, Eunwoo Nam, Chan Hyuk Park
Gastrointestinal Endoscopy.2020; 92(3): 692. CrossRef - The current capacity and quality of colonoscopy in Korea
Jae Ho Choi, Jae Myung Cha, Jin Young Yoon, Min Seob Kwak, Jung Won Jeon, Hyun Phil Shin
Intestinal Research.2019; 17(1): 119. CrossRef - Appropriate Surveillance Interval after Colonoscopic Polypectomy in Patients Younger than 50 Years
Yoon Suk Jung, Nam Hee Kim, Jung Ho Park, Dong Il Park, Chong Il Sohn
Journal of Korean Medical Science.2019;[Epub] CrossRef - Terminology, Molecular Features, Epidemiology, and Management of Serrated Colorectal Neoplasia
Seth D. Crockett, Iris D. Nagtegaal
Gastroenterology.2019; 157(4): 949. CrossRef - Risk of Developing Metachronous Advanced Colorectal Neoplasia After Polypectomy in Patients With Multiple Diminutive or Small Adenomas
Nam Hee Kim, Yoon Suk Jung, Mi Yeon Lee, Jung Ho Park, Dong Il Park, Chong Il Sohn
American Journal of Gastroenterology.2019; 114(10): 1657. CrossRef - Visceral obesity as a risk factor for colorectal adenoma occurrence in surveillance colonoscopy
Jong Pil Im, Donghee Kim, Su Jin Chung, Eun Hyo Jin, Yoo Min Han, Min Jung Park, Ji Hyun Song, Sun Young Yang, Young Sun Kim, Jeong Yoon Yim, Seon Hee Lim, Joo Sung Kim
Gastrointestinal Endoscopy.2018; 88(1): 119. CrossRef - Guideline Adherence to Colonoscopic Surveillance Intervals after Polypectomy in Korea: Results from a Nationwide Survey
Seri Hong, Mina Suh, Kui Son Choi, Boyoung Park, Jae Myung Cha, Hyun-Soo Kim, Jae Kwan Jun, Dong Soo Han
Gut and Liver.2018; 12(4): 426. CrossRef - Risk factors of nonadherence to colonoscopy surveillance after polypectomy and its impact on clinical outcomes: a KASID multicenter study
Chung Hyun Tae, Chang Mo Moon, Seong-Eun Kim, Sung-Ae Jung, Chang Soo Eun, Jae Jun Park, Geom Seog Seo, Jae Myung Cha, Sung Chul Park, Jaeyoung Chun, Hyun Jung Lee, Yunho Jung, Jin Oh Kim, Young-Eun Joo, Dong Il Park
Journal of Gastroenterology.2017; 52(7): 809. CrossRef - Unusual Local Recurrence with Distant Metastasis after Successful Endoscopic Submucosal Dissection for Colorectal Mucosal Cancer
Hyo Jeong Lee, Byong Duk Ye, Jeong-Sik Byeon, Jihun Kim, Young Soo Park, Yong Sang Hong, Yong Sik Yoon, Dong-Hoon Yang
Clinical Endoscopy.2017; 50(1): 91. CrossRef - Determining the optimal surveillance interval after a colonoscopic polypectomy for the Korean population?
Jung Lok Lee, Jae Myung Cha, Hye Min Lee, Jung Won Jeon, Min Seob Kwak, Jin Young Yoon, Hyun Phil Shin, Kwang Ro Joo, Joung Il Lee, Dong Il Park
Intestinal Research.2017; 15(1): 109. CrossRef - Advanced Colonic Neoplasia at Follow-up Colonoscopy According to Risk Components and Adenoma Location at Index Colonoscopy: A Retrospective Study of 1,974 Asymptomatic Koreans
Su Jung Baik, Hyojin Park, Jae Jun Park, Hyun Ju Lee, So Young Jo, Yoo Mi Park, Hye Sun Lee
Gut and Liver.2017; 11(5): 667. CrossRef - The Serrated Polyp Pathway: Is It Time to Alter Surveillance Guidelines?
Brendon O’Connell, Nazar Hafiz, Seth Crockett
Current Gastroenterology Reports.2017;[Epub] CrossRef - Optimizing post‐polypectomy surveillance: A practical guide for the endoscopist
Roel Bogie, Silvia Sanduleanu
Digestive Endoscopy.2016; 28(3): 348. CrossRef - Cap-assisted EMR for rectal neuroendocrine tumors: comparisons with conventional EMR and endoscopic submucosal dissection (with videos)
Dong-Hoon Yang, Yangsoon Park, Sang Hyoung Park, Kyung-Jo Kim, Byong Duk Ye, Jeong-Sik Byeon, Seung-Jae Myung, Suk-Kyun Yang
Gastrointestinal Endoscopy.2016; 83(5): 1015. CrossRef - Colorectal cancer screening of the general population in East Asia
Yasushi Sano, Jeong‐Sik Byeon, Xiao‐Bo Li, Martin C.S. Wong, Han‐Mo Chiu, Rungsun Rerknimitr, Takahiro Utsumi, Santa Hattori, Wataru Sano, Mineo Iwatate, Philip Chiu, Joseph Sung
Digestive Endoscopy.2016; 28(3): 243. CrossRef - Surveillance colonoscopy after endoscopic treatment for colorectal neoplasia: From the standpoint of the Asia–Pacific region
Takahisa Matsuda, Han‐Mo Chiu, Yasushi Sano, Takahiro Fujii, Akiko Ono, Yutaka Saito
Digestive Endoscopy.2016; 28(3): 342. CrossRef - Long-Term Outcome and Surveillance Colonoscopy after Successful Endoscopic Treatment of Large Sessile Colorectal Polyps
Bun Kim, A Ra Choi, Soo Jung Park, Jae Hee Cheon, Tae Il Kim, Won Ho Kim, Sung Pil Hong
Yonsei Medical Journal.2016; 57(5): 1106. CrossRef - Probability of High-Risk Colorectal Neoplasm Recurrence Based on the Results of Two Previous Colonoscopies
Hye Won Park, Seungbong Han, Ji Young Lee, Hye-Sook Chang, Jaewon Choe, Yunsik Choi, Hoonsub So, Dong-Hoon Yang, Seung-Jae Myung, Suk-Kyun Yang, Jin-Ho Kim, Jeong-Sik Byeon
Digestive Diseases and Sciences.2015; 60(1): 226. CrossRef - Distribution of the Colonoscopic Adenoma Detection Rate According to Age: Is Recommending Colonoscopy Screening for Koreans Over the Age of 50 Safe?
Taeseok Bae, Yunhyung Ha, Changkyun Kim, Jihyun Lee, Kwangil Ha, Sanghyun Shin, Youngcheol Lee, Yoonsik Kang
Annals of Coloproctology.2015; 31(2): 46. CrossRef - Risk of adenomas with high‐risk characteristics based on two previous colonoscopy
Kang‐Heum Suh, Ja Seol Koo, Jong Jin Hyun, Jungsoon Choi, Jang Soo Han, Seung Young Kim, Sung Woo Jung, Yoon Tae Jeen, Sang Woo Lee, Jai Hyun Choi
Journal of Gastroenterology and Hepatology.2014; 29(12): 1985. CrossRef - Only the Size of Resected Polyps Is an Independent Risk Factor for Delayed Postpolypectomy Hemorrhage: A 10-Year Single-Center Case-Control Study
Hee Seok Moon, Sun Wook Park, Dong Hwan Kim, Sun Hyung Kang, Jae Kyu Sung, Hyun Yong Jeong
Annals of Coloproctology.2014; 30(4): 182. CrossRef - Prevalence of and Risk Factors for Gastrointestinal Diseases in Korean Americans and Native Koreans Undergoing Screening Endoscopy
Hee Sun Kim, Su Jung Baik, Kyung Hee Kim, Cho Rong Oh, Jung Hyun Lee, Wan Jae Jo, Hye Kyoung Kim, Eun Young Kim, Min Jung Kim
Gut and Liver.2013; 7(5): 539. CrossRef - Proximal colon cancer and serrated adenomas – hunting the missing 10%
Pelvender Gill, Hannah Rafferty, David Munday, Adam Bailey, Lai Mun Wang, James E East, Runjan Chetty, Simon J Leedham
Clinical Medicine.2013; 13(6): 557. CrossRef - Relationship of Non-Alcoholic Fatty Liver Disease to Colorectal Neoplasia
Jue Yong Lee, Ja Won Kim
Korean Journal of Medicine.2013; 84(3): 363. CrossRef - Highlights of International Digestive Endoscopy Network 2013
Kwang An Kwon, Il Ju Choi, Eun Young Kim, Seok Ho Dong, Ki Baik Hahm
Clinical Endoscopy.2013; 46(5): 425. CrossRef
- Post-colonoscopy colorectal cancers in a national fecal immunochemical test-based colorectal cancer screening program
- 10,175 View
- 161 Download
- 38 Crossref
- Korean Guidelines for Colorectal Cancer Screening and Polyp Detection
- Bo-In Lee, Sung Pil Hong, Seong-Eun Kim, Se Hyung Kim, Hyun-Soo Kim, Sung Noh Hong, Dong-Hoon Yang, Sung Jae Shin, Suck-Ho Lee, Dong Il Park, Young-Ho Kim, Hyun Jung Kim, Suk-Kyun Yang, Hyo Jong Kim, Hae Jeong Jeon, Multi-Society Task Force for Development of Guidelines for Colorectal Polyp Screening, Surveillance and Management
- Clin Endosc 2012;45(1):25-43. Published online March 31, 2012
- DOI: https://doi.org/10.5946/ce.2012.45.1.25
-
Abstract
PDFSupplementary MaterialPubReaderePub
Now colorectal cancer is the second most common cancer in males and the fourth most common cancer in females in Korea. Since most of colorectal cancers occur after the prolonged transformation of adenomas into carcinomas, early detection and removal of colorectal adenomas are one of the most effective methods to prevent colorectal cancer. Considering the increasing incidence of colorectal cancer and polyps in Korea, it is very important to establish Korean guideline for colorectal cancer screening and polyp detection. The guideline was developed by the Korean Multi-Society Take Force and we tried to establish the guideline by evidence-based methods. Parts of the statements were draw by systematic reviews and meta-analyses. Herein we discussed epidemiology of colorectal cancers and adenomas in Korea and optimal methods for screening of colorectal cancer and detection of adenomas including fecal occult blood tests, radiologic tests, and endoscopic examinations.
-
Citations
Citations to this article as recorded by- Colorectal cancer screening guidelines for average-risk and high-risk individuals: A systematic review
Caroline Tanadi, Kevin Tandarto, Maureen Miracle Stella, Kenny Wijaya Sutanto, Mario Steffanus, Riki Tenggara, Muhammad Begawan Bestari
Romanian Journal of Internal Medicine.2024; 62(2): 101. CrossRef - Trends in colorectal cancer incidence according to an increase in the number of colonoscopy cases in Korea
Ga Hee Kim, Yeong Chan Lee, Tae Jun Kim, Sung Noh Hong, Dong Kyung Chang, Young-Ho Kim, Dong-Hoon Yang, Chang Mo Moon, Kyunga Kim, Hyun Gun Kim, Eun-Ran Kim
World Journal of Gastrointestinal Oncology.2024; 16(1): 51. CrossRef - Evaluation of the “Burgenland PREvention trial of colorectal cancer Disease with ImmunologiCal Testing” (B-PREDICT)—a population-based colorectal cancer screening program
Stefanie BREZINA, Gernot LEEB, Andreas BAIERL, Evelyn GRÄF, Monika HACKL, Philipp HOFER, Harald LANG, Michaela KLEIN, Karl MACH, Remy SCHWARZER, Wilhelm WLASSITS, Andreas PÜSPÖK, Andrea GSUR
BMC Gastroenterology.2024;[Epub] CrossRef - 2022 Seoul Consensus on Clinical Practice Guidelines for Functional Constipation
Young Sin Cho, Yoo Jin Lee, Jeong Eun Shin, Hye-Kyung Jung, Seon-Young Park, Seung Joo Kang, Kyung Ho Song, Jung-Wook Kim, Hyun Chul Lim, Hee Sun Park, Seong-Jung Kim, Ra Ri Cha, Ki Bae Bang, Chang Seok Bang, Sung Kyun Yim, Seung-Bum Ryoo, Bong Hyeon Kye,
Journal of Neurogastroenterology and Motility.2023; 29(3): 271. CrossRef - Association of HLA-G 3′UTR polymorphisms and haplotypes with colorectal cancer susceptibility and prognosis
Sabrine Dhouioui, Ahmed-Baligh Laaribi, Nadia Boujelbene, Refka Jelassi, Hamza Ben Salah, Hedia Bellali, Hadda-Imene Ouzari, Amel Mezlini, Inès Zemni, Hanene Chelbi, Inès Zidi
Human Immunology.2022; 83(1): 39. CrossRef - An updated review of the methods, guidelines of, and controversies on screening for colorectal cancer
Sameh Hany Emile, Samer Hani Barsom, Steven D. Wexner
The American Journal of Surgery.2022; 224(1): 339. CrossRef - Disparities in Recommendations for Colorectal Cancer Screening Among Average-Risk Individuals: An Ecobiosocial Approach
Sharifah Saffinas Syed Soffian, Azmawati Mohammed Nawi, Rozita Hod, Mohd Rizal Abdul Manaf, Huan-Keat Chan, Muhammad Radzi Abu Hassan
Risk Management and Healthcare Policy.2022; Volume 15: 1025. CrossRef - Apurinic/apyrimidinic endonuclease 1 is associated with poor prognosis after curative resection followed by adjuvant chemotherapy in patients with stage III colon cancer
Ji Hyeong Song, Myung Sun Lee, Eun Young Cha, Kyung Ha Lee, Ji Yeon Kim, Jin Soo Kim
Korean Journal of Clinical Oncology.2022; 18(1): 1. CrossRef - Systematic review of shared decision‐making in guidelines about colorectal cancer screening
Marta Maes‐Carballo, Manuel García‐García, Yolanda Gómez‐Fandiño, Carlos Roberto Estrada‐López, Andrés Iglesias‐Álvarez, Aurora Bueno‐Cavanillas, Khalid Saeed Khan
European Journal of Cancer Care.2022;[Epub] CrossRef - Real-World Use of Colonoscopy in an Older Population: A Nationwide Standard Cohort Study Using a Common Data Model
Ha Il Kim, Jin Young Yoon, Min Seob Kwak, Jae Myung Cha
Digestive Diseases and Sciences.2021; 66(7): 2227. CrossRef - Cecal intubation time in screening colonoscopy
Hyun Young Kim
Medicine.2021; 100(19): e25927. CrossRef - Gastrointestinal and Nongastrointestinal Complications of Esophagogastroduodenoscopy and Colonoscopy in the Real World: A Nationwide Standard Cohort Using the Common Data Model Database
Ha Il Kim, Jin Young Yoon, Min Seob Kwak, Jae Myung Cha
Gut and Liver.2021; 15(4): 569. CrossRef - Optimal postoperative surveillance strategies for stage III colorectal cancer
Min Young Park, In Ja Park, Hyo Seon Ryu, Jay Jung, Minsung Kim, Seok-Byung Lim, Chang Sik Yu, Jin Cheon Kim
World Journal of Gastrointestinal Surgery.2021; 13(9): 1012. CrossRef - Tumor Size >5 cm and Harvested LNs <12 Are the Risk Factors for Recurrence in Stage I Colon and Rectal Cancer after Radical Resection
Hye-Sol Jung, Seung-Bum Ryoo, Han-Ki Lim, Min Jung Kim, Sang Hui Moon, Ji Won Park, Seung-Yong Jeong, Kyu Joo Park
Cancers.2021; 13(21): 5294. CrossRef - Colon Polyp Detection in Primary Health Care Institutions of Korea: Detection Rate and Issues with Following the Guidelines
Sang Hyun Park, Kwang Il Hong, Hyun Chul Park, Young Sun Kim, Gene Hyun Bok, Kyung Ho Kim, Dong Suk Shin, Jae Yong Han, Young Kwan Kim, Yeun Jong Choi, Soo Hoon Eun, Byung Hoon Lim, Kyeong Kun Kwack
The Korean Journal of Gastroenterology.2021; 78(6): 328. CrossRef - Evaluation of the Cut-Off Value of Fecal Immunochemical Test for Colorectal Cancer Screening during Health Checkups
Hye-Ran Park, Eun-Hee Nah, Jong-Seon Lee, Seon Cho
Journal of Laboratory Medicine and Quality Assurance.2021; 43(4): 190. CrossRef - Risk of developing metachronous advanced colorectal neoplasia after resection of low-risk diminutive versus small adenomas
Nam Hee Kim, Yoon Suk Jung, Jung Ho Park, Dong Il Park, Chong Il Sohn
Gastrointestinal Endoscopy.2020; 91(3): 622. CrossRef - Factors Associated With Colonoscopy Compliance Based on Health Belief Model in a Community-Based Colorectal Cancer Screening Program Shanghai, China
Lihua He, Shuna Gao, Sha Tao, Weiyi Li, Juan Du, Yunfang Ji, Yejing Wang
International Quarterly of Community Health Education.2020; 41(1): 25. CrossRef - Prevalence of and Risk Factors for Colorectal Neoplasia in Asymptomatic Young Adults (20–39 Years Old)
Nam Hee Kim, Yoon Suk Jung, Hyo-Joon Yang, Soo-Kyung Park, Jung Ho Park, Dong Il Park, Chong Il Sohn
Clinical Gastroenterology and Hepatology.2019; 17(1): 115. CrossRef - Optimal colonoscopy surveillance interval period for the adenoma patients who had an adequate polypectomy at baseline colonoscopy
Jian Dong, Minman Wu, Jiarong Miao, Tao Zhi, Tianmei Zhang, Gang Yang, Yarong Chen, Lei Zhang, Qiong Nan
European Journal of Cancer Prevention.2019; 28(1): 10. CrossRef - Impact of family history of colorectal cancer on age‐specific prevalence of colorectal neoplasia
Chan Hyuk Park, Nam Hee Kim, Jung Ho Park, Dong Il Park, Chong Il Sohn, Yoon Suk Jung
Journal of Gastroenterology and Hepatology.2019; 34(3): 537. CrossRef - A Novel Blood‐Based Colorectal Cancer Diagnostic Technology Using Electrical Detection of Colon Cancer Secreted Protein‐2
Minhong Jeun, Hyo Jeong Lee, Sungwook Park, Eun‐ju Do, Jaewon Choi, You‐Na Sung, Seung‐Mo Hong, Sang‐Yeob Kim, Dong‐Hee Kim, Ja Young Kang, Hye‐Nam Son, Jinmyoung Joo, Eun Mi Song, Sung Wook Hwang, Sang Hyoung Park, Dong‐Hoon Yang, Byong Duk Ye, Jeong‐Sik
Advanced Science.2019;[Epub] CrossRef - Increasing Trend in Young-Onset Colorectal Cancer in Asia: More Cancers in Men and More Rectal Cancers
Joseph J.Y. Sung, Han-Mo Chiu, Kyu-Won Jung, Jae Kwan Jun, Masau Sekiguchi, Takahisa Matsuda, Moe H. Kyaw
American Journal of Gastroenterology.2019; 114(2): 322. CrossRef - Bowel preparation for colonoscopy may decrease the levels of testosterone in Korean men
Soo-Hyun Lee, Seung Geon Park, Moon-Jong Kim, Hyejin Chun, Doo-Yeoun Cho, Doohee Hong, Young-Sang Kim
Scientific Reports.2019;[Epub] CrossRef - A Comparative Study Evaluating the Incidence of Colorectal Neoplasia(s) in Candidates for Bariatric Surgery by Screening Colonoscopy, 40–49 Versus 50–65 Years Old: a Preliminary Study
Toygar Toydemir, Görkem Özgen, İsmail Çalıkoğlu, Özdal Ersoy, Mehmet Ali Yerdel
Obesity Surgery.2019; 29(8): 2430. CrossRef - Appropriate Surveillance Interval after Colonoscopic Polypectomy in Patients Younger than 50 Years
Yoon Suk Jung, Nam Hee Kim, Jung Ho Park, Dong Il Park, Chong Il Sohn
Journal of Korean Medical Science.2019;[Epub] CrossRef - The Rise of Colorectal Cancer in Asia: Epidemiology, Screening, and Management
Elias F. Onyoh, Wen-Feng Hsu, Li-Chun Chang, Yi-Chia Lee, Ming-Shiang Wu, Han-Mo Chiu
Current Gastroenterology Reports.2019;[Epub] CrossRef - Colonic Intramucosal Cancer in the Interposed Colon Treated with Endoscopic Mucosal Resection: A Case Report and Review of Literature
Seung-Ho Baek, Jang-Ho Lee, Dong Ryeol Yoo, Hye Yeong Kim, Meihua Jin, Ah-reum Jang, Dong-Hoon Yang, Jeong-Sik Byeon
Clinical Endoscopy.2019; 52(4): 377. CrossRef - IMMUNOCHROMATOGRAPHIC TEST FOR DETECTION OF FECAL OCCULT BLOOD
Anna Viktorovna Nikitina, Y. A. Akinshina, N. E. Nishchakova, E. A. Amelina, S. G. Mardanly
Russian Clinical Laboratory Diagnostics.2019; 64(9): 536. CrossRef - Abdominal Obesity is More Predictive of Advanced Colorectal Neoplasia Risk Than Overall Obesity in Men
Nam Hee Kim, Yoon Suk Jung, Jung Ho Park, Dong Il Park, Chong Il Sohn
Journal of Clinical Gastroenterology.2019; 53(7): e284. CrossRef - Stool-Based miR-92a and miR-144* as Noninvasive Biomarkers for Colorectal Cancer Screening
Hyun Ho Choi, Young-Seok Cho, Ji Hye Choi, Hyung-Keun Kim, Sung Soo Kim, Hiun-Suk Chae
Oncology.2019; 97(3): 173. CrossRef - Association between family history of colorectal cancer and the risk of metachronous colorectal neoplasia following polypectomy in patients aged < 50 years
Nam Hee Kim, Yoon Suk Jung, Jung Ho Park, Dong Il Park, Chong Il Sohn
Journal of Gastroenterology and Hepatology.2019; 34(2): 383. CrossRef - Risk of metachronous neoplasia on surveillance colonoscopy in young patients with colorectal neoplasia
Hyun Gun Kim, Young-Seok Cho, Jae Myung Cha, Jeong Eun Shin, Kyeong Ok Kim, Hyo-Joon Yang, Hoon Sup Koo, Young-Eun Joo, Sun-Jin Boo
Gastrointestinal Endoscopy.2018; 87(3): 666. CrossRef - Systematic review of colorectal cancer screening guidelines for average-risk adults: Summarizing the current global recommendations
Florence Bénard, Alan N Barkun, Myriam Martel, Daniel von Renteln
World Journal of Gastroenterology.2018; 24(1): 124. CrossRef - Stages of Adoption for Fecal Occult Blood Test and Colonoscopy Tests for Colorectal Cancer Screening in Korea
Nhung Cam Bui, Ha Na Cho, Yoon Young Lee, Mina Suh, Boyoung Park, Jae Kwan Jun, Yeol Kim, Kui Son Choi
Cancer Research and Treatment.2018; 50(2): 416. CrossRef - Anatomical distribution and detection rate of colorectal neoplasms according to age in the colonoscopic screening of a Korean population
Suk-young Lee, Wan Hee Song, Sang Cheul Oh, Byung-Wook Min, Sun Il Lee
Annals of Surgical Treatment and Research.2018; 94(1): 36. CrossRef - The prognostic implications of primary tumor location on recurrence in early-stage colorectal cancer with no associated risk factors
Sung Il Kang, Duck-Woo Kim, Yoonjin Kwak, Hye-Seung Lee, Min Hyun Kim, Myung Jo Kim, Heung-Kwon Oh, Sung-Bum Kang
International Journal of Colorectal Disease.2018; 33(6): 719. CrossRef - A combination of clinical risk stratification and fecal immunochemical test is useful for identifying persons with high priority of early colonoscopy
Yoon Suk Jung, Chan Hyuk Park, Nam Hee Kim, Jung Ho Park, Dong Il Park, Chong Il Sohn
Digestive and Liver Disease.2018; 50(3): 254. CrossRef - Guideline Adherence to Colonoscopic Surveillance Intervals after Polypectomy in Korea: Results from a Nationwide Survey
Seri Hong, Mina Suh, Kui Son Choi, Boyoung Park, Jae Myung Cha, Hyun-Soo Kim, Jae Kwan Jun, Dong Soo Han
Gut and Liver.2018; 12(4): 426. CrossRef - Risk of developing metachronous advanced colorectal neoplasia after colonoscopic polypectomy in patients aged 30 to 39 and 40 to 49 years
Nam Hee Kim, Yoon Suk Jung, Jung Ho Park, Dong Il Park, Chong Il Sohn
Gastrointestinal Endoscopy.2018; 88(4): 715. CrossRef - A simple scoring model for advanced colorectal neoplasm in asymptomatic subjects aged 40–49 years
Yoo Mi Park, Hee Sun Kim, Jae Jun Park, Su Jung Baik, Young Hoon Youn, Jie-Hyun Kim, Hyojin Park
BMC Gastroenterology.2017;[Epub] CrossRef - The fecal immunochemical test has high accuracy for detecting advanced colorectal neoplasia before age 50
Nam Hee Kim, Jung Ho Park, Dong Il Park, Chong Il Sohn, Kyuyong Choi, Yoon Suk Jung
Digestive and Liver Disease.2017; 49(5): 557. CrossRef - Colorectal cancer screening with the fecal immunochemical test in persons aged 30 to 49 years: focusing on the age for commencing screening
Yoon Suk Jung, Chan Hyuk Park, Nam Hee Kim, Jung Ho Park, Dong Il Park, Chong Il Sohn
Gastrointestinal Endoscopy.2017; 86(5): 892. CrossRef - Biomedical optical spectroscopy for the early diagnosis of gastrointestinal neoplasms
Qin-Si Wan, Ting Wang, Kun-He Zhang
Tumor Biology.2017; 39(7): 101042831771798. CrossRef - Training in Endoscopy: Colonoscopy
Hyun Joo Jang
Clinical Endoscopy.2017; 50(4): 322. CrossRef - Impact of Age on the Risk of Advanced Colorectal Neoplasia in a Young Population: An Analysis Using the Predicted Probability Model
Yoon Suk Jung, Chan Hyuk Park, Nam Hee Kim, Mi Yeon Lee, Dong Il Park
Digestive Diseases and Sciences.2017; 62(9): 2518. CrossRef - Screening of colorectal cancer: present and future
Marcello Maida, Fabio Salvatore Macaluso, Gianluca Ianiro, Francesca Mangiola, Emanuele Sinagra, Georgina Hold, Carlo Maida, Giovanni Cammarota, Antonio Gasbarrini, Giuseppe Scarpulla
Expert Review of Anticancer Therapy.2017; 17(12): 1131. CrossRef - Advanced Colonic Neoplasia at Follow-up Colonoscopy According to Risk Components and Adenoma Location at Index Colonoscopy: A Retrospective Study of 1,974 Asymptomatic Koreans
Su Jung Baik, Hyojin Park, Jae Jun Park, Hyun Ju Lee, So Young Jo, Yoo Mi Park, Hye Sun Lee
Gut and Liver.2017; 11(5): 667. CrossRef - Risk Factors Such as Male Sex, Smoking, Metabolic Syndrome, Obesity, and Fatty Liver Do Not Justify Screening Colonoscopies Before Age 45
Yoon Suk Jung, Kyung Eun Yun, Yoosoo Chang, Seungho Ryu, Dong Il Park
Digestive Diseases and Sciences.2016; 61(4): 1021. CrossRef - Risk of developing advanced colorectal neoplasia after removing high‐risk adenoma detected at index colonoscopy in young patients: A KASID study
Soo‐Kyung Park, Nam Hee Kim, Yoon Suk Jung, Won Hee Kim, Chang Soo Eun, Bong Min Ko, Geom Seog Seo, Jae Myung Cha, Jae Jun Park, Kyeong Ok Kim, Chang Mo Moon, Yoonho Jung, Eun Soo Kim, Seong Ran Jeon, Chang Kyun Lee, Dong Il Park
Journal of Gastroenterology and Hepatology.2016; 31(1): 138. CrossRef - Colorectal cancer screening of the general population in East Asia
Yasushi Sano, Jeong‐Sik Byeon, Xiao‐Bo Li, Martin C.S. Wong, Han‐Mo Chiu, Rungsun Rerknimitr, Takahiro Utsumi, Santa Hattori, Wataru Sano, Mineo Iwatate, Philip Chiu, Joseph Sung
Digestive Endoscopy.2016; 28(3): 243. CrossRef - Does Low Threshold Value Use Improve Proximal Neoplasia Detection by Fecal Immunochemical Test?
Nam Hee Kim, Hyo-Joon Yang, Soo-Kyung Park, Jung Ho Park, Dong Il Park, Chong Il Sohn, Kyuyong Choi, Yoon Suk Jung
Digestive Diseases and Sciences.2016; 61(9): 2685. CrossRef - High levels of carcinoembryonic antigen and smoking might be markers of colorectal adenoma in Korean males aged 40-49 years
In Cheol Yoon, Jeong Hyeon Cho, Heejin Choi, Young Hoon Choi, Kyu Min Lim, Sung Hwa Choi, Jae Ho Han, Hyeon Ju Jeong, Hong Sub Lee
Yeungnam University Journal of Medicine.2016; 33(1): 13. CrossRef - Endoscopic Resection for Small Rectal Neuroendocrine Tumors: Comparison of Endoscopic Submucosal Resection with Band Ligation and Endoscopic Submucosal Dissection
Byoung Wook Bang, Jin Seok Park, Hyung Kil Kim, Yong Woon Shin, Kye Sook Kwon, Joon Mee Kim
Gastroenterology Research and Practice.2016; 2016: 1. CrossRef - Is a Preoperative Gastrointestinal Endoscopy for Second Primary Cancer Detection in Head and Neck Cancer Necessary? Ten-year Registry Data
Gyeong Mi Heo, Mi Hee Kim, Jin Hwan Kim, Young Soo Rho, Woon Geon Shin
The Korean Journal of Gastroenterology.2016; 68(1): 23. CrossRef - Effect of Previous Gastrectomy on the Performance of Postoperative Colonoscopy
Sunghwan Kim, Jeongmin Choi, Tae Han Kim, Seong-Ho Kong, Yun-Suhk Suh, Jong Pil Im, Hyuk-Joon Lee, Sang Gyun Kim, Seung-Yong Jeong, Joo Sung Kim, Han-Kwang Yang
Journal of Gastric Cancer.2016; 16(3): 167. CrossRef - Diagnostic Value of Methylated Septin9 for Colorectal Cancer Screening: A Meta-Analysis
Shirong Yan, Zijing Liu, Shuang Yu, Yixi Bao
Medical Science Monitor.2016; 22: 3409. CrossRef - Characteristics of and risk factors for colorectal neoplasms in young adults in a screening population
Seung Eun Lee, Hee Bum Jo, Won Gun Kwack, Yun Jin Jeong, Yeo-Jin Yoon, Hyoun Woo Kang
World Journal of Gastroenterology.2016; 22(10): 2981. CrossRef - Background and significance of Korean national cancer screening guideline revision
Won-Chul Lee, Yeol Kim
Journal of the Korean Medical Association.2015; 58(4): 274. CrossRef - Effect of different reconstruction algorithms on computer-aided diagnosis (CAD) performance in ultra-low dose CT colonography
Eun Sun Lee, Se Hyung Kim, Jong Pil Im, Sang Gyun Kim, Cheong-il Shin, Joon Koo Han, Byung Ihn Choi
European Journal of Radiology.2015; 84(4): 547. CrossRef - Comparing the effectiveness of competing tests for reducing colorectal cancer mortality: a network meta-analysis
B. Joseph Elmunzer, Amit G. Singal, Jeremy B. Sussman, Amar R. Deshpande, Daniel A. Sussman, Marisa L. Conte, Ben A. Dwamena, Mary A.M. Rogers, Philip S. Schoenfeld, John M. Inadomi, Sameer D. Saini, Akbar K. Waljee
Gastrointestinal Endoscopy.2015; 81(3): 700. CrossRef - Risk factors for colorectal neoplasia in persons aged 30 to 39 years and 40 to 49 years
Yoon Suk Jung, Seungho Ryu, Yoosoo Chang, Kyung Eun Yun, Jung Ho Park, Hong Joo Kim, Yong Kyun Cho, Chong Il Sohn, Woo Kyu Jeon, Byung Ik Kim, Dong Il Park
Gastrointestinal Endoscopy.2015; 81(3): 637. CrossRef - Non-invasive screening for colorectal cancer in Asia
Han-Mo Chiu, Li-Chun Chang, Wen-Feng Hsu, Chu-Kuang Chou, Ming-Shiang Wu
Best Practice & Research Clinical Gastroenterology.2015; 29(6): 953. CrossRef - Risk Factors for Delayed Post-Polypectomy Bleeding
Min Jung Kwon, You Sun Kim, Song I Bae, Young Il Park, Kyung Jin Lee, Jung Hwa Min, Soo Yeon Jo, Mi Young Kim, Hye Jin Jung, Seong Yeon Jeong, Won Jae Yoon, Jin Nam Kim, Jeong Seop Moon
Intestinal Research.2015; 13(2): 160. CrossRef - Distribution of the Colonoscopic Adenoma Detection Rate According to Age: Is Recommending Colonoscopy Screening for Koreans Over the Age of 50 Safe?
Taeseok Bae, Yunhyung Ha, Changkyun Kim, Jihyun Lee, Kwangil Ha, Sanghyun Shin, Youngcheol Lee, Yoonsik Kang
Annals of Coloproctology.2015; 31(2): 46. CrossRef - The Korean guideline for colorectal cancer screening
Dae Kyung Sohn, Min Ju Kim, Younhee Park, Mina Suh, Aesun Shin, Hee Young Lee, Jong Pil Im, Hyoen-Min Cho, Sung Pil Hong, Baek-hui Kim, Yongsoo Kim, Jeong Wook Kim, Hyun-Soo Kim, Chung Mo Nam, Dong Il Park, Jun Won Um, Soon Nam Oh, Hwan Sub Lim, Hee Jin C
Journal of the Korean Medical Association.2015; 58(5): 420. CrossRef - Age-specific prevalence of serrated lesions and their subtypes by screening colonoscopy: a retrospective study
Hyun Young Kim, Seon Mie Kim, Ji-Hyun Seo, Eun-Ha Park, Nayoung Kim, Dong Ho Lee
BMC Gastroenterology.2014;[Epub] CrossRef - Clinical features and course of ulcerative colitis diagnosed in asymptomatic subjects
Soo-Kyung Park, Byong Duk Ye, Suk-Kyun Yang, Seon-Ok Kim, Jihun Kim, Jong Wook Kim, Sang Hyoung Park, Dong-Hoon Yang, Kee Wook Jung, Kyung-Jo Kim, Jeong-Sik Byeon, Seung-Jae Myung, Jin-Ho Kim
Journal of Crohn's and Colitis.2014; 8(10): 1254. CrossRef - Do We Need Colonoscopy Following Acute Diverticulitis Detected on Computed Tomography to Exclude Colorectal Malignancy?
Young Hoon Choi, Seong-Joon Koh, Ji Won Kim, Byeong Gwan Kim, Kook Lae Lee, Jong Pil Im, Joo Sung Kim, Hyun Chae Jung
Digestive Diseases and Sciences.2014; 59(9): 2236. CrossRef - A Survey of Colonoscopic Surveillance After Polypectomy
Dae Kyung Sohn
Annals of Coloproctology.2014; 30(2): 88. CrossRef - The Prevalence of Colorectal Adenomas in Asymptomatic Korean Men and Women
Moon Hee Yang, Sanjay Rampal, Jidong Sung, Yoon-Ho Choi, Hee Jung Son, Jun Haeng Lee, Young-Ho Kim, Dong Kyung Chang, Poong-Lyul Rhee, Jong Chul Rhee, Eliseo Guallar, Juhee Cho
Cancer Epidemiology, Biomarkers & Prevention.2014; 23(3): 499. CrossRef - Circulating Methylated Septin 9 Nucleic Acid in the Plasma of Patients with Gastrointestinal Cancer in the Stomach and Colon
Hye Seung Lee, Sang Mee Hwang, Taek Soo Kim, Duck-Woo Kim, Do Joong Park, Sung-Bum Kang, Hyung-Ho Kim, Kyoung Un Park
Translational Oncology.2013; 6(3): 290. CrossRef
- Colorectal cancer screening guidelines for average-risk and high-risk individuals: A systematic review
- 12,710 View
- 164 Download
- 72 Crossref
- Korean Guideline for Colonoscopic Polypectomy
- Suck-Ho Lee, Sung Jae Shin, Dong Il Park, Seong-Eun Kim, Hae Jeong Jeon, Se Hyung Kim, Sung Pil Hong, Sung Noh Hong, Dong-Hoon Yang, Bo In Lee, Young-Ho Kim, Hyun-Soo Kim, Hyun Jung Kim, Suk-Kyun Yang, Hyo Jong Kim, Multi-Society Task Force for Development of Guidelines for Colorectal Polyp Screening, Surveillance and Management
- Clin Endosc 2012;45(1):11-24. Published online March 31, 2012
- DOI: https://doi.org/10.5946/ce.2012.45.1.11
-
Abstract
PDFSupplementary MaterialPubReaderePub
There is indirect evidence to suggest that 80% of colorectal cancers (CRC) develop from adenomatous polyps and that, on average, it takes 10 years for a small polyp to transform into invasive CRC. In multiple cohort studies, colonoscopic polypectomy has been shown to significantly reduce the expected incidence of CRC by 76% to 90%. Colonoscopic polypectomy is performed frequently in primary outpatient clinics and secondary and tertiary medical centers in Korea. However, there are no evidence-based, procedural guidelines for the appropriate performance of this procedure, including the technical aspects. For the guideline presented here, PubMed, Medline, and Cochrane Library literature searches were performed. When little or no data from well-designed prospective trials were available, an emphasis was placed on the results from large series and reports from recognized experts. Thus, these guidelines for colonoscopic polypectomy are based on a critical review of the available data as well as expert consensus. Further controlled clinical studies are needed to clarify aspects of this statement, and revision may be necessary as new data become available. This guideline is intended to be an educational device to provide information that may assist endoscopists in providing care to patients. This guideline is not a rule and should not be construed as a legal standard of care or as encouraging, advocating, requiring, or discouraging any particular treatment. Clinical decisions for any particular case involve a complex analysis of the patient's condition and the available courses of action.
-
Citations
Citations to this article as recorded by- Modified underwater endoscopic mucosal resection for intermediate-sized sessile colorectal polyps
Dong Hyun Kim, Seon-Young Park, Hye-Su You, Yong-Wook Jung, Young-Eun Joo, Dae-Seong Myung, Hyun-Soo Kim, Nah Ihm Kim, Seong-Jung Kim, Jae Kyun Ju
Frontiers in Medicine.2023;[Epub] CrossRef - Endoscopic treatment of colorectal polyps and early colorectal cancer
Yunho Jung
Journal of the Korean Medical Association.2023; 66(11): 642. CrossRef - Circumferential submucosal incision prior to endoscopic mucosal resection versus conventional endoscopic mucosal resection for colorectal lesions with endoscopic features of sessile serrated lesions
Chang Kyo Oh, Bo-In Lee, Sung Hak Lee, Seung-Jun Kim, Han Hee Lee, Chul-Hyun Lim, Jin Su Kim, Yu Kyung Cho, Jae Myung Park, Young-Seok Cho, In Seok Lee, Myung-Gyu Choi
Surgical Endoscopy.2022; 36(3): 2087. CrossRef - Polypectomy for Diminutive and Small Colorectal Polyps
Melissa Zarandi-Nowroozi, Roupen Djinbachian, Daniel von Renteln
Gastrointestinal Endoscopy Clinics of North America.2022; 32(2): 241. CrossRef - Risk of post-polypectomy bleeding after endoscopic mucosal resection in patients receiving antiplatelet medication: comparison between the continue and hold groups
Sang Hyun Park, Soo-Kyung Park, Hyo-Joon Yang, Yoon Suk Jung, Jung Ho Park, Chong Il Sohn, Dong Il Park
Surgical Endoscopy.2022; 36(9): 6410. CrossRef - Hot snare polypectomy versus endoscopic mucosal resection for small colorectal polyps: a randomized controlled trial
Seung-Jun Kim, Bo-In Lee, Eun Sun Jung, Joon Sung Kim, Sun-Young Jun, Woohyeon Kim, Hyoju Ham, Minah Kim, Sung Hak Lee, Han Hee Lee, Jae Myung Park, Myung-Gyu Choi
Surgical Endoscopy.2021; 35(9): 5096. CrossRef - Gastrointestinal and Nongastrointestinal Complications of Esophagogastroduodenoscopy and Colonoscopy in the Real World: A Nationwide Standard Cohort Using the Common Data Model Database
Ha Il Kim, Jin Young Yoon, Min Seob Kwak, Jae Myung Cha
Gut and Liver.2021; 15(4): 569. CrossRef - Clinical Practice Guideline for the Management of Antithrombotic Agents in Patients Undergoing Gastrointestinal Endoscopy
Hyun Lim, Eun Jeong Gong, Byung-Hoon Min, Seung Joo Kang, Cheol Min Shin, Jeong-Sik Byeon, Miyoung Choi, Chan Guk Park, Joo Young Cho, Soo Teik Lee, Ho Gak Kim, Hoon Jai Chun
The Korean Journal of Gastroenterology.2020; 76(6): 282. CrossRef - Endoscopic Submucosal Dissection for Colitis-Associated Dysplasia
Dong-Hoon Yang, Imelda Rey
Clinical Endoscopy.2019; 52(2): 120. CrossRef - Prospective analysis of delayed colorectal post-polypectomy bleeding
Soo-Kyung Park, Jeong Yeon Seo, Min-Gu Lee, Hyo-Joon Yang, Yoon Suk Jung, Kyu Yong Choi, Hungdai Kim, Hyung Ook Kim, Kyung Uk Jung, Ho-Kyung Chun, Dong Il Park
Surgical Endoscopy.2018; 32(7): 3282. CrossRef - Endoscopic Instruments and Electrosurgical Unit for Colonoscopic Polypectomy
Hong Jun Park
Clinical Endoscopy.2016; 49(4): 350. CrossRef - Effectiveness of adjuvant radiotherapy after local excision of rectal cancer with deep submucosal invasion: a single-hospital, case–control analysis
Seohyun Lee, Chang Gok Woo, Hyo Jeong Lee, Kyung-Jo Kim, Byong Duk Ye, Jeong-Sik Byeon, Seung-Jae Myung, Suk-Kyun Yang, Young Soo Park, Jin-hong Park, Jong Hoon Kim, Seok-Byung Lim, Jin Cheon Kim, Chang Sik Yu, Dong-Hoon Yang
Surgical Endoscopy.2015; 29(11): 3231. CrossRef - The Feasibility of Performing Colorectal Endoscopic Submucosal Dissection Without Previous Experience in Performing Gastric Endoscopic Submucosal Dissection
Dong-Hoon Yang, Gwi Hong Jeong, Yerim Song, Sang Hyoung Park, Soo-Kyung Park, Jong Wook Kim, Kee Wook Jung, Kyung-Jo Kim, Byong Duk Ye, Seung-Jae Myung, Suk-Kyun Yang, Jin-Ho Kim, Young Soo Park, Jeong-Sik Byeon
Digestive Diseases and Sciences.2015; 60(11): 3431. CrossRef - Association between the Position of Colorectal Polyps and Clinical Outcomes of Polypectomy: Focused on Procedure Time, Complication and Histopatholgic Result
Jung Hyun Park, Jae Hyeok Choi, Hyeong Jung Na, Won Geon Kwak, Jong Sun Choi, Eo Jin Kim, Jae Hak Kim
Intestinal Research.2013; 11(3): 191. CrossRef - Preparation and Patient Evaluation for Safe Gastrointestinal Endoscopy
Seong Hee Kang, Jong Jin Hyun
Clinical Endoscopy.2013; 46(3): 212. CrossRef - International Digestive Endoscopy Network to Strengthen Network for Lower Gastrointestinal Diseases Including Inflammatory Bowel Disease and Colorectal Cancer
Kwang An Kwon
Clinical Endoscopy.2012; 45(3): 251. CrossRef
- Modified underwater endoscopic mucosal resection for intermediate-sized sessile colorectal polyps
- 10,371 View
- 137 Download
- 16 Crossref
 First
First Prev
Prev


