
Articles
- Page Path
- HOME > Clin Endosc > Volume 47(3); 2014 > Article
- Focused Review Series: Endoscopic Intervention in Pancreatitis Endoscopic Treatment of Pancreatic Calculi
- Yong Hoon Kim1, Sung Ill Jang2, Kwangwon Rhee3, Dong Ki Lee1
-
Clinical Endoscopy 2014;47(3):227-235.
DOI: https://doi.org/10.5946/ce.2014.47.3.227
Published online: May 31, 2014
1Department of Internal Medicine, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
2Department of Internal Medicine, Hallym University Kangnam Sacred Heart Hospital, Hallym University College of Medicine, Seoul, Korea.
3Department of Internal Medicine, Godoil Hospital, Seoul, Korea.
- Correspondence: Dong Ki Lee. Department of Internal Medicine, Gangnam Severance Hospital, Yonsei University College of Medicine, 211 Eonju-ro, Gangnam-gu, Seoul 135-720, Korea. Tel: +82-2-2019-3214, Fax: +82-2-3463-3882, dklee@yuhs.ac
• Received: April 11, 2014 • Revised: May 7, 2014 • Accepted: May 13, 2014
Copyright © 2014 Korean Society of Gastrointestinal Endoscopy
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- Abstract
- INTRODUCTION
- HISTORY
- DIAGNOSIS
- INDICATIONS FOR TREATMENT
- TECHNIQUES FOR STONE REMOVAL
- DIFFICULTY TREATING PANCREATIC CALCULI
- ENDOSCOPIC PANCREATIC SPHINCTEROTOMY AND BALLOON SPHINCTEROPLASTY
- EXTRACTION BALLOONS, BASKETS, AND FORCEPS
- STONE FRAGMENTATION USING ESWL
- INTRADUCTAL MECHANICAL LITHOTRIPSY AND ELECTRO HYDRAULIC LITHOTRIPSY
- SHORT-TERM AND LONG-TERM OUTCOMES
- BENEFIT TO PANCREAS FUNCTION
- COMPARISON WITH SURGICAL TREATMENT
- NECESSITY OF SURGERY
- CURRENT GUIDELINES
- CONCLUSIONS
- NOTES
- REFERENCES
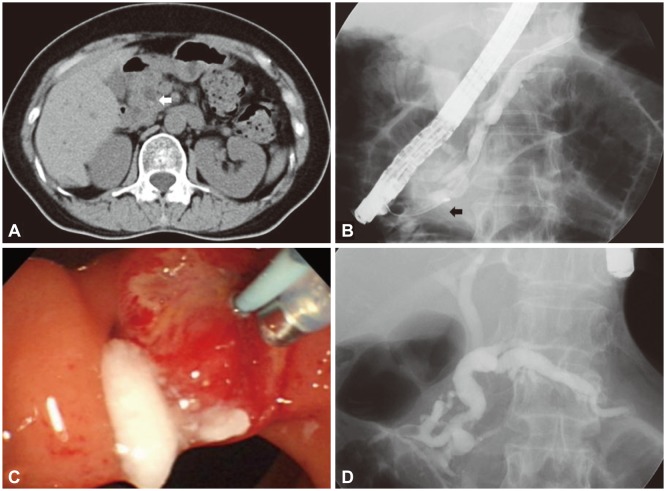
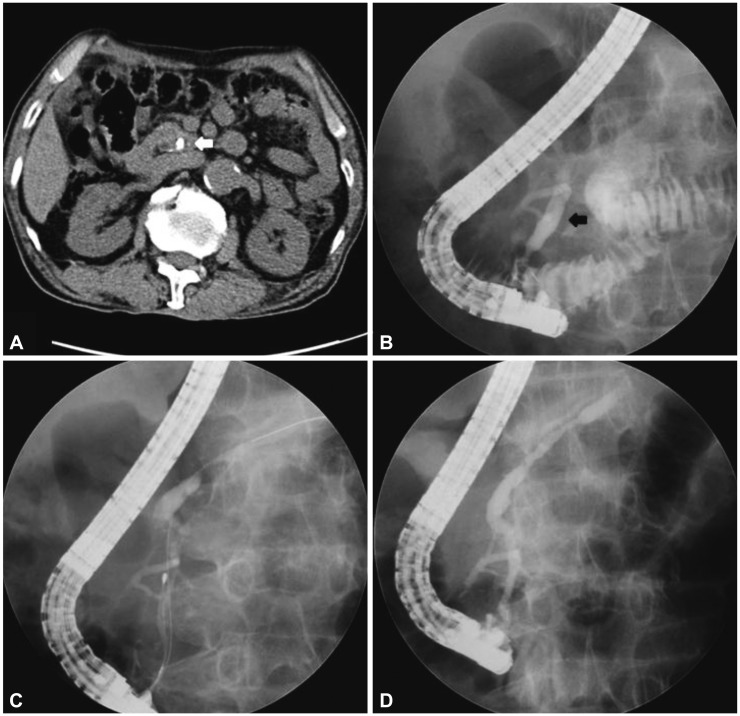
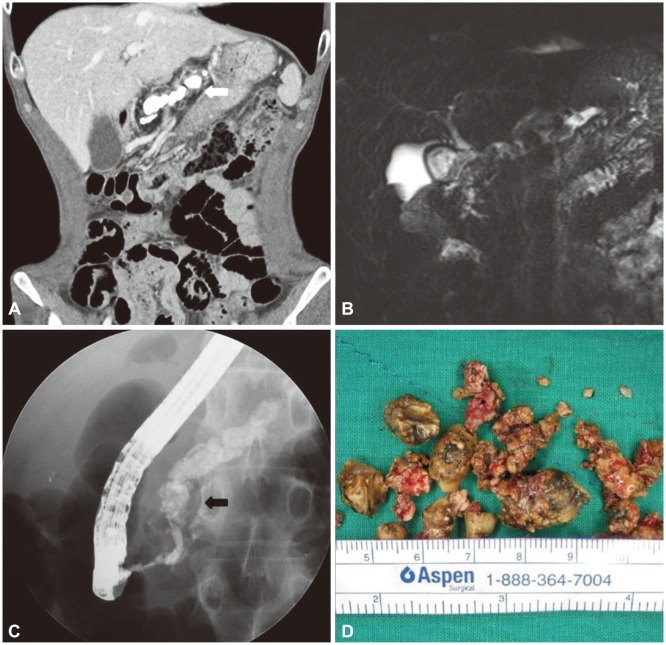

Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Pancreatic duct stones treated by Whipple as a last resort: A case report
Usra I. Ghanem, Peter R. Bael, Izzeddin Bakri, Bashar Jaber, Omar Abu-Zaydeh, Khaled N. Al-Shawa
International Journal of Surgery Case Reports.2024; 115: 109286. CrossRef - Endoscopic Retrograde Cholangiopancreatography for Management of Chronic Pancreatitis
Aliana Bofill-Garcia, Camille Lupianez-Merly
Gastrointestinal Endoscopy Clinics of North America.2024; 34(3): 449. CrossRef - Management of Pancreatic Duct Stones
Christian Gerges, Torsten Beyna, Horst Neuhaus
Gastrointestinal Endoscopy Clinics of North America.2023; 33(4): 821. CrossRef - Transpapillary Pancreatoscopy in an Emergency Hospital
L. L. Generdukayev, Yu. S. Teterin, D. A. Blagovestnov, E. S. Yeletskaya, K. A. Nugumanova, P. A. Yartsev
Russian Sklifosovsky Journal "Emergency Medical Care".2023; 12(2): 316. CrossRef - Rectal indometacin to prevent pancreatitis after extracorporeal shock wave lithotripsy (RIPEP): a single-centre, double-blind, randomised, placebo-controlled trial
Yang-Yang Qian, Nan Ru, Hui Chen, Wen-Bin Zou, Hao Wu, Jun Pan, Bo Li, Lei Xin, Ji-Yao Guo, Xin-Ying Tang, Liang-Hao Hu, Zhen-Dong Jin, Dong Wang, Yi-Qi Du, Luo-Wei Wang, Zhao-Shen Li, Zhuan Liao
The Lancet Gastroenterology & Hepatology.2022; 7(3): 238. CrossRef - ESWL pancreatitis: yet another post-procedural pancreatitis to worry about?
Lars Aabakken, Vemund Paulsen
The Lancet Gastroenterology & Hepatology.2022; 7(3): 199. CrossRef - Per-oral pancreatoscopy with intraductal lithotripsy for difficult pancreatic duct stones: a systematic review and meta-analysis
Thomas R. McCarty, Zain Sobani, Tarun Rustagi
Endoscopy International Open.2020; 08(10): E1460. CrossRef - Pancreatoscopy in endoscopic treatment of pancreatic duct stones: a systematic review
Christian Gerges, David Pullmann, Markus Schneider, Peter Siersema, Erwin van Geenen, Horst Neuhaus, Torsten Beyna
Minerva Chirurgica.2019;[Epub] CrossRef - Management Algorithm of Pancreatic Calculi
Dong Kee Jang, Jun Kyu Lee
The Korean Journal of Pancreas and Biliary Tract.2019; 24(3): 89. CrossRef - Basket impaction during the extraction of a pancreatic ductal stone
Ankit Dalal, Gaurav K. Patil, Amit P. Maydeo, Arun Iyer, Nikhil Patil
Indian Journal of Gastroenterology.2019; 38(6): 550. CrossRef - Laparoscopic pancreatic duct incision and stone removal and T-type tube drainage for pancreatic duct stone: A case report and review of literature
Yang Bai, Shi-An Yu, Li-Yuan Wang, Dao-Jun Gong
World Journal of Clinical Cases.2018; 6(13): 679. CrossRef - Endoscopic Therapies for Chronic Pancreatitis
Jeffrey M. Adler, Timothy B. Gardner
Digestive Diseases and Sciences.2017; 62(7): 1729. CrossRef - Rectally administered indomethacin to prevent post-ESWL-pancreatitis (RIPEP): study protocol for a randomized controlled trial
Yang-Yang Qian, Hui Chen, Xin-Ying Tang, Xi Jiang, Wei Qian, Wen-Bin Zou, Lei Xin, Bo Li, Yan-Fen Qi, Liang-Hao Hu, Duo-Wu Zou, Zhen-Dong Jin, Dong Wang, Yi-Qi Du, Luo-Wei Wang, Feng Liu, Zhao-Shen Li, Zhuan Liao
Trials.2017;[Epub] CrossRef - Recent Advances in Management of Chronic Pancreatitis
Seon Mee Park
The Korean Journal of Gastroenterology.2015; 66(3): 144. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
CiteEndoscopic Treatment of Pancreatic Calculi
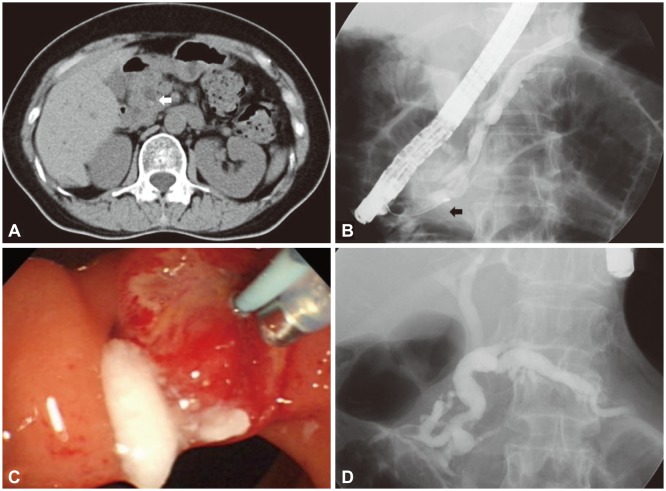
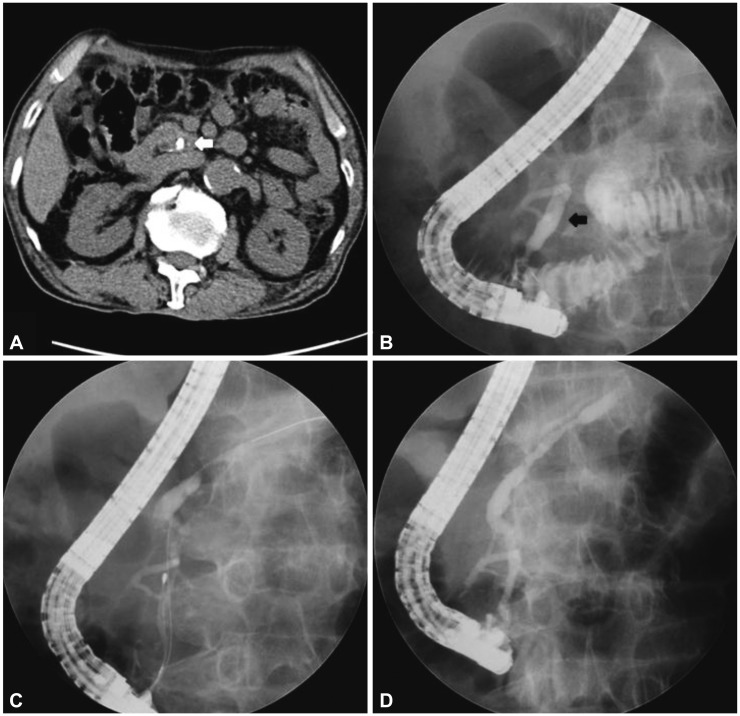
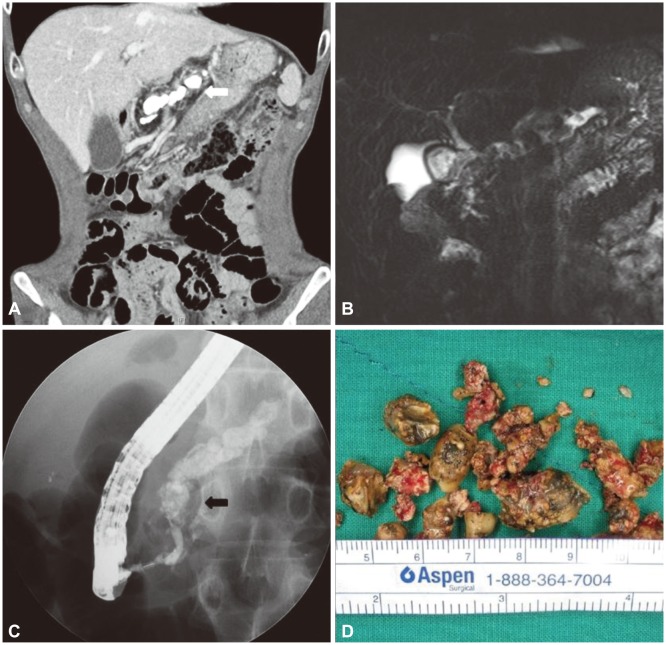
Fig. 1 Endoscopic intervention for pancreatic duct stones (PDSs). (A) Abdominal computed tomographic scan shows a 4 mm sized calcified stone (white arrow) in pancreatic head within dilated pancreatic duct. (B) Small size of the PDSs let basket removal possible (black arrow). (C) PDS was visualized intraluminally. (D) No filling defect was observed in the main pancreatic duct after complete stone removal.
Fig. 2 Endoscopic intervention after extracorporeal shock wave lithotripsy (ESWL) for fragmentation of large stone. (A) Abdominal computed tomographic scan shows 10 mm sized calcified stones (white arrow) in pancreatic head within markedly dilated pancreatic duct. (B) Large pancreatic duct stones in the pancreas head (black arrow) rendered the catheter impassable. (C) After two sessions of ESWL, stones were fragmented to the degree that can be removed with basket. (D) No filling defect was observed in the main pancreatic duct after complete stone removal.
Fig. 3 Surgical treatment for multiple large pancreatic duct stones (PDSs). (A) There are extensive calcified stones in pancreatic duct (white arrow). (B) Magnetic resonance cholangiopancreatography shows markedly dilated pancreatic duct with innumerable internal stones. (C) Pancreatogram via major papilla demonstrates pancreatic duct, full of large PDSs (black arrow), which was an indication for surgical treatment. (D) Multiple PDSs removed by Roux-en Y pancreaticojejunostomy surgery.


